Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Effects of long-term benzodiazepine use wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
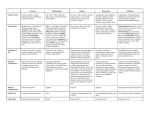
Plants Animals (toads) Seeds Powders Capsules Designed to be smoked Some are now reclassified and illegal Legal highs are manufactured, often in unlicensed laboratories in China and south east Asia, using a variety of chemicals which are often very similar to those contained in illegal drugs, but are often far less researched. In some cases, chemists attach a few additional molecules to an illegal drug’s chemical formula in order to make sure the new variant evades UK drug laws. They are sold either over the internet, in head shops or on the streets by drug dealers. Because they are cheaper to buy than illegal drugs and widely available over the internet, they can be more appealing and accessible to young people. Stimulate receptor › Opiates Increase release of neurotransmitter Prevent reuptake of transmitter IV mcat use › Reported in London, Barnsley, Lancashire, South Wales › Very damaging to soft tissue resulting in severe cytoxic reactions o Opiates: euphoria, analgesia, drowsiness o morphine like o partial agonists o Stimulants: overactive, talkative, confident o entactogens o amphetamines and cocaine o Depressants: relaxation, disinhibition o cannabinoids o alcohol o benzodiazepines o Hallucinogens: altered perception, mood change o solvents o LSD and psylocibin Effects › Euphoria, relaxation, drowsiness › Nausea and vomiting (novice users) › Pinpoint pupils Adverse consequences › Respiratory depression › Anorexia, constipation, weight loss Withdrawal › Runny eyes and nose, hot and cold sweats › Dilated pupils › Stomach cramps and muscle aches › Insomnia Effects › Euphoria › Overactivity, talkativeness, energy, confidence › Empathy › Perceptual awareness, illusions (dance drugs) Adverse consequences › Hypertension › Dehydration (dance drugs) › Blood clotting Withdrawal symptoms › Dysphoria with insomnia and nightmares › Fatigue and prolonged sleep episodes Effects › Tingling in body and head – dizziness and lightheadedness, tachycardia › Intensification of mental associations › Relaxed, calm, disconnected from reality, incoherent conversation › Heightened perception and distortion of time › Drowsiness, muscle weakness › Increased appetite Withdrawal › Craving, irritable › Insomnia, strange dreams, loss of appetite Effects › Altered perceptions with visual, tactile and auditory hallucinations › Intensification of colours and sound › Mood change Adverse consequences › Flashbacks › Psychosis Alcohol Benzodiazepines Opioids Stimulants Cannabis Psychotomimetics Enzyme induction reduces plasma levels of aminophylline (asthma) and coumarin (anticoagulant). Alcohol slows glucose production and reduces glycogen stores – risk of hypoglycaemia. H2 antagonists (gastric ulcer) block gastric ADH – increase BAC. Chlorpropamide (diabetes), mushrooms and metronidazole (fungal infections) block acetaldehyde dehydrogenase – disulfiram like reaction. H2 antagonists and alcohol induce enzymes reducing plasma levels of long acting benzodiazepines. Oral contraceptives increase effects of long acting ones. Risk of respiratory depression and death when used with other depressants. Antihistamines can enhance analgesia and reduce emetic effect. Avoid MAOIs – encephalopathy with meperidine. Risk of hypertension, CVA, heart attack and sudden death with other sympathomimetics. Potentiated by MAOIs. Combined amphetamine and beta blockers may cause alpha adrenergic overactivity – hypertension. Interactions are rare. Psychosis may occur with disulfiram or SSRIs. Enzyme induction reduces plasma levels of theophylline and propranalol. Stimulant effects may be increased with other stimulants – seizures,hyperthermia. Legal highs mimic or are variations on “known” substances The pharmacology is not well researched Effects and adverse consequences are as the existing categories of substances Treatment should follow the same pathway as any other substance use treatment package 39 year old male, married with a twelve week old son History of compulsive behaviour from age 17 including promiscuity, drinking, drug taking notably cocaine Low moods - started taking ketamine to combat them. Taking ¾ gram per day Dislikes psychedelic effects – believes he has telepathic powers and can communicate to a god or aliens, vivid memory recall of sexual abuse Neglecting wife, child and career. Wife has asked him to move out 37 year old male, single, unemployed ‘Legal highs’ since April 2010 including mephedrone, methylone, naphyrone, MDAI, 5-AIA, ‘Benzofury’, ‘Ivory wave’, methoxetamine on a near-daily basis Describes effects as ‘cosmic, spiritual, out of this world, unbelievable’. ‘TV talking to me’,’forces pulling me to do things’, ‘seeing mist and light’ Evidence of dependence: tolerance, salience, relief dosing (for comedowns) and continued use despite harms (including probable police charge for possession with intent to supply; and total expenditure of £20 000+)