Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
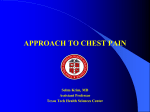
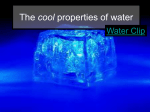
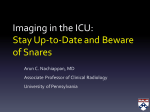
Tension Pneumothorax [Diseases of the pleura] Current Opinion in Pulmonary Medicine. 5(4):269, July 1999. Barton, Erik D. MD, MS. Department of Emergency Medicine, Brigham & Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA. Abstract The diagnosis of tension pneumothorax has typically been taught as the presence of hemodynamic compromise with an expanding intrapleural space air mass. This may occur quickly or gradually, depending on the degree of lung injury and respiratory state of the patient. Experimentally, tension pneumothorax is a multifactorial event that manifests a state of central hypoxemia, compensatory mechanisms, and mechanical compression on intrathoracic structures. Studies using animal models suggest that overt hypotension is a delayed finding that immediately precedes cardiorespiratory collapse. Recognition of early signs and symptoms associated with tension pneumothorax, eg, progressive hypoxemia, tachycardia, and respiratory distress, can alert medical personnel to the need for rapid decompression before physiologic decompensation. Abbreviations: NT needle thoracostomy, TT tube thoracostomy, Tension pneumothorax is an insidious, life-threatening event most commonly encountered in the prehospital, emergency department, trauma unit, and critical care settings. The pathophysiology of tension pneumothorax is a progressive accumulation of air in the pleural space that exerts mechanical pressure on intrathoracic structures. If it is left untreated, significant respiratory compromise and cardiovascular collapse can occur. Expedient recognition of risk factors and early signs and symptoms of tension pneumothorax are necessary for rapid intervention to prevent this outcome. Case 1 A 38-year-old man was brought into the trauma unit at 7 AM, approximately 3 hours after he reportedly fell from his roof while trying to climb into a second story window. He was intoxicated and was found by his mother, crawling on the grass toward the front door. On arrival, he was awake, responsive, and following commands. His vital signs were a blood pressure of 100/70 mm Hg, heart rate of 110 bpm, and oxygen saturation of 93% on 15 liters by face mask. Primary survey was notable for decreased breath sound and crepitus over the left chest. This patient was believed to be relatively stable by the trauma surgeons, and a portable chest radiograph was ordered. Over the next several minutes, the patient’s blood pressure deteriorated to 70/40 mm Hg, heart rate increased to 150 bpm, and oxygen saturation decreased to 89% despite continued oxygen therapy. An immediate needle thoracostomy (NT) was performed with release of air followed by a tube thoracostomy (TT). The patient’s hemodynamic parameters stabilized immediately after decompression. The chest radiograph showed a left pneumothorax with mediastinal shift to the right, widened rib spaces, posterior rib fractures on the left, and a flattened left hemidiaphragm (Fig. 1). No other injuries were found after a complete trauma workup. Case 2 A 59-year-old woman with significant chronic obstructive pulmonary disease was brought into the emergency department in severe respiratory decompensation. After initial attempts with [beta]-agonist therapy and steroids, she was endotracheally intubated using a rapid-sequence intubation protocol. After a few minutes of being ventilated using a bag-valve-mask device, she became cyanotic from the neck up, with a loss of oxygen saturation reading. Lung compliance worsened with increased resistance on the ventilation bag. Her chest was hyperexpanded and she had absent breath sounds over both lung fields and the abdomen. A recheck of the endotracheal tube showed it to be properly placed in the vocal cords. Her pulse was no longer palpable. The patient underwent bilateral NT with the release of a large amount of air on both sides. Bilateral TT procedures completely decompressed the tension pneumothorax, and the patient had a return of normal color and pulse. A persistent bronchopleural fistula prolonged the patient’s hospital course until she finally underwent corrective surgery. Figure 1. Chest radiograph of a left tension pneumothorax in a trauma patient (Case 1) Note the mediastinal shift to the right, widened rib spacing, and posterior rib fractures on the left. A flattening of the left hemidiaphragm is also present (not shown). Discussion The temporal nature of tension pneumothorax is highly variable and is most likely related to the respiratory status and degree of lung parenchymal injury of the patient. Tension pneumothorax can develop quickly, within a few minutes following lung injury, especially in patients on positive pressure ventilation or with significant underlying parenchymal disease (eg, Case 2). Conversely, cardiovascular compromise may develop more slowly in spontaneously respiring patients because of a temporal delay in overcoming compensatory mechanisms and negative inspiratory pressures. Some patients (eg, Case 1) present several hours after acute trauma or the development of a spontaneous pneumothorax with evidence of only mild cardiovascular compromise caused by an accumulating air mass; however, after a critical point in the progression of tension pneumothorax is reached, severe and rapid decompensation may occur unexpectedly if the diagnosis is not initially appreciated. For this reason, any history of blunt or penetrating trauma to the chest wall with even mild cardiovascular instability should heighten the awareness of this condition and prompt early intervention. The physician should not attempt to first confirm the diagnosis with a chest radiograph. Pathophysiology The recognition of “tension physiology,” or hypotension and respiratory compromise in the presence of a pneumothorax, has been the hallmark in diagnosing tension pneumothorax [1]. The underlying lung parenchymal injury is thought to act as a one-way valve that allows the entry of air into the intrapleural space on inspiration but does not allow reverse flow to the atmosphere on expiration. The resultant expanding air mass exerts pressure that causes a collapse of the ipsilateral lung and a shift of the mediastinum toward the contralateral side. This shift is thought to be associated with compression of the vena cava and right heart structures, causing decreased diastolic filling and cardiac output. In addition is significant shunting of blood to underventilated areas of the lung with subsequent ventilation-toperfusion mismatch. The result is hypoxemia, acidosis, and shock. Acute trauma to the thorax remains one of the most easily recognizable causes of tension pneumothorax. Either blunt or penetrating mechanisms can lead to significant underlying parenchymal injury and, overall, approximately 5% of multiple-trauma patients have a pneumothorax. To assume that a penetrating chest wall injury results only in an open pneumothorax and to not convert to a tension pneumothorax are inappropriate. Any evidence of cardiorespiratory compromise should warrant emergent thoracostomy in these patients. Iatrogenic interventions are becoming increasingly recognized as a significant cause of tension pneumothorax. Several reports of tension pneumothorax associated with percutaneous central venous catheter placements and transthoracic needle biopsies have been published. In some cases, symptoms have not appeared until several days after the procedure [2]. Less-invasive procedures, eg, the placement of a thoracic epidural catheter [3] or even the use of local anesthesia on the chest wall, have been reported to cause tension pneumothorax [4]. Several cases of tension pneumothorax associated with other procedures more removed from the thorax, eg, abdominal laparoscopy [5, 6]or percutaneous dilation tracheostomy [7], have also been reported. Spontaneous pneumothorax is another risk factor for tension pneumothorax. Primary spontaneous pneumothorax is typically caused by rupture of the subpleural emphysematous blebs, usually located in the apices of young, healthy patients without other lung disease [8]. Tension pneumothorax develops in a few of these patients, and they may be treated conservatively if they are asymptomatic and the pneumothorax volume is small (< 15%). Secondary spontaneous pneumothorax occurs in patients with underlying lung disease, and the frequency is directly related to the severity of their disease [9]. These patients typically are more symptomatic because of decreased pulmonary reserve and are at much higher risk for tension pneumothorax, especially when undergoing invasive procedures or mechanical ventilation. Experimental sudies Experimentally, tension pneumothorax has been described as a state in which intrapleural pressures become positive throughout the respiratory cycle in spontaneously breathing patients [10] (Fig. 2). Any compensation by negative inspiratory forces has been overcome, resulting in progressive cardiorespiratory compromise. The earliest animal (dogs) studies suggested that a mechanical compression, or “kinking,” of the central venous and right heart structures was the cause of cardiovascular collapse [11, 12]. Canine mediastinums, however, were found to be more mobile and fenestrated, allowing communication from one hemithorax to the other [13, 14]. Thus, intrapleural pressures caused by expanding air masses may be more directly transmitted to central structures in dogs and not necessarily representative of human physiology. Subsequent studies using spontaneously respiring goats [10] and sheep [15] with intact mediastinums more similar to humans demonstrated a significant hypoxemia, with the development of tension pneumothorax in the absence of significant arterial hypotension. This gave rise to the hypothesis for central hypoxia and respiratory acidosis, rather than a direct compression of central venous structures, as a cause of cardiovascular collapse. The progressive hypoxemia has been attributed primarily to increasing pulmonary vascular shunting in conjunction with increasing lung parenchymal collapse. These studies demonstrated a preservation of cardiac output and arterial pressures with tension pneumothorax that was thought to be related to three compensatory mechanisms: 1) incomplete transmission of increased intrapleural pressure on the mediastinum on contralateral pleural space, 2) increased spontaneous respiratory effort and intrathoracic pressure fluctuations that maintain venous return, and 3) a baroreceptor-mediated reflex or catecholamine-induced tachycardia that compensates for a decrease in left ventricular stroke volume [15]. More recently, animal studies using positive-pressure ventilation have been performed to assess the hemodynamic changes associated with progressive pneumothorax. The combined extrinsic pressures of positive-pressure ventilation and increasing intrapleural air would be expected to cause earlier mechanical compression and hemodynamic instability compared with a spontaneously breathing subject. Carvalho et al. [16] used anesthetized and mechanically ventilated sheep to directly measure cardiac output and pulmonary blood flow during a stepwise, progressive pneumothorax to +25 cm H2O of intrapleural pressure. With increased intrapleural pressure came a significant decrease in pulmonary arterial and bronchial arterial blood flow on the ipsilateral side, corresponding to a decrease in cardiac output (Fig. 3). These findings demonstrated a direct mechanical compressive effect on the ipsilateral lung. In addition were a significant hypoxemia and hypercarbia induced by alveolar collapse and progressive ventilation-toperfusion inequality. When pleural pressures were returned to baseline with resolution of the pneumothorax, hemodynamic parameters normalized, whereas hypoxemia and hypercarbia persisted. Similarly, a decrease in lung compliance occurred after the insult and persisted with the ventilation-to-perfusion abnormalities. Figure 3. Effect of pleural pressure (Ppl), measured in right pleural space, on cardiac output (QT) and mean differential pulmonary arterial blood flows. *Significantly different compared with baseline values, P < 0.001. Values are means ± SE; n, number of animals. Solid circle, increasing Ppl; hollow circle, decreasing Ppl. Top two dashed lines, QT; solid lines, left pulmonary arterial flow (Qlpa); bottom two dashed lines, right pulmonary arterial flow (Qrpa). (From Carvalho et al.[16]; with permission.) T In the authors’ laboratory, the authors used mechanically ventilated swine to induce a stable, progressive pneumothorax to tension and assessed the changes in hemodynamics and oxygenation [17]. Pigs were chosen because they have been demonstrated to be good models of human respiratory and cardiovascular systems [18]. With a progressive introduction of pleural space air came an immediate decrease in oxygen saturation, which continued to decrease throughout the experiment (Fig. 4). Oxygen saturation levels were recorded at less than 50% just before cardiovascular collapse and were associated with a significant acidemia. A smaller, progressive decrement in cardiac output occurred early in the experiment, with a dramatic decrease at tension pneumothorax volumes of more than 85% total lung capacity (Fig. 5). Mean arterial pressures and heart rates remained relatively stable until approximately 47% total lung capacity pneumothorax was reached. After this point was a progressive decrease in mean arterial pressures and increase in heart rate. Central venous pressures showed a progressive increase as mean intrapleural pressures increased with the progressive pneumothorax. The central venous pressure measures were significantly higher than the mean intrapleural pressure measures in a linear fashion, demonstrating preservation of venous blood flow to the heart (Fig. 6). At the point of cardiovascular collapse (> 85% total lung capacity pneumothorax) was a dramatic decrease in carbon monoxide, heart rate, and mean arterial pressure. At this point, central venous pressure and mean intrapleural pressure levels equalized (15 mm Hg), suggesting complete occlusion of central venous return. Figure 4. The effects of progressive tension pneumothorax on oxygen saturation in ventilated swine (mean ± SD). (From Barton et al.[17]; with permission.) These studies demonstrate two factors that contribute to the ultimate cardiorespiratory collapse associated with tension pneumothorax. A significant hypoxemia is early and progressive and is typically caused by mechanical alveolar compression and worsened ventilation-to-perfusion inequalities. Compensatory mechanisms, eg, elevation in heart rate and increased respiratory excursions, may initially serve to preserve hemodynamics in spontaneously breathing patients. Earlier mechanical compressive effects of tension pneumothorax seem to exist in subjects on positive pressure ventilation; however, at what stage compressive forces become significant in tension pneumothorax is unclear because these effects are typically noted in the presence of severe hypoxemia. Ultimately, significant hemodynamic compromise, or “tension physiology,” is a late finding and heralds a preterminal event requiring immediate intervention. These studies demonstrate two factors that contribute to the ultimate cardiorespiratory collapse associated with tension pneumothorax. A significant hypoxemia is early and progressive and is typically caused by mechanical alveolar compression and worsened ventilation-to-perfusion inequalities. Compensatory mechanisms, eg, elevation in heart rate and increased respiratory excursions, may initially serve to preserve hemodynamics in spontaneously breathing patients. Earlier mechanical compressive effects of tension pneumothorax seem to exist in subjects on positive pressure ventilation; however, at what stage compressive forces become significant in tension pneumothorax is unclear because these effects are typically noted in the presence of severe hypoxemia. Ultimately, significant hemodynamic compromise, or “tension physiology,” is a late finding and heralds a preterminal event requiring immediate intervention. Treatment Decompression of any tension pneumothorax or suspected tension pneumothorax is the mainstay of therapy. NT with either a commercial device or a large-bore, sheathed catheter is a rapid maneuver promoted by most emergency and trauma specialists. For many years, placement of an NT device had been typically performed in the midclavicular line at the second intercostal space of the anterior chest; however, the inability to penetrate the parietal pleura in patients with thick musculature or excessive subcutaneous tissue in that area has led to treatment failures [19, 20]. More recently, the American College of Surgeons has recommended use of the fourth or fifth intercostal space at the anterior axillary line (at the same location used for TT) as the point of entry [21]. This space avoids the pectoralis and latissimus dorsi muscles and typically contains less adipose tissue than the anterior chest wall. Several problems with NT decompression have been observed. Inadequate needle length, inability to penetrate the chest wall, catheter kinking or a failure to drain, and poor retention or dislodgment of these devices have all been reported anecdotally and in the literature [19, 20]. In several cases, NT procedures have had to be repeated to ensure adequate decompression until formal TT could be performed [22]. Thus, NT is promoted as a temporizing measure only and is not considered a definitive treatment for cases of tension pneumothorax. Figure 5. The hemodynamic effects of progressive tension pneumothorax on cardiac output (C.O.), heart rate, mean arterial pressure (MAP), central venous pressure (CVP), and mean intrapleural pressure (MIP) in ventilated swine. (From Barton et al.[17]; with permission.) The definitive treatment of patients with tension pneumothorax is still TT and should be performed before fluid resuscitation or chest radiography if the diagnosis is suspected. For acute, traumatic tension pneumothorax, a largebore chest tube should be used to ensure adequate drainage of both air and blood. Smaller-bore tubes may be considered for other causes in which drainage of blood or other effusions is not necessary. Adequate drainage should be maintained until the underlying parenchyma has healed and no further air leak is detected. With the expanding scope of practice observed in many emergency medical systems, the use of prehospital thoracostomy has come under much scrutiny in the past several years. Some believe that emergency medical service providers who may be inadequately trained in the recognition of a suspected tension pneumothorax, use of proper technique, or the ability to care for potential complications should avoid these procedures. Retrospective studies, however, have demonstrated appropriate response and few adverse outcomes with prehospital NT and TT procedures [22, 23]. One unique approach to decompression in the field that has been described is a modified thoracostomy without chest tube placement [24]. This technique uses a rapid, simple thoracostomy for intubated patients and avoids the risks and excess time involved to place a chest tube in a nonsterile environment. Converting a potential tension pneumothorax or hemothorax to an open pneumothorax decreased scene time, was easier to perform, and did not necessitate the skill for chest tube insertion. Figure 6. The relationship between MIP, CVP, and cardiac output with progressive tension pneumothorax. Note the equalization of mean intrapleural pressure (MIP) and central venous pressure (CVP) at the point of collapse of cardiac output. (From Barton et al.[17]; with permission.) Conclusions Tension pneumothorax can be an elusive diagnosis and most often results in physiologic decompensation. Early signs and symptoms include a progressive respiratory distress, tachycardia, and hypoxemia. Temporally, this can occur quickly, especially in mechanically ventilated patients, or more gradually, depending on the degree of underlying lung injury. Hypotension has been shown to be a delayed finding that foreshadows cardiovascular collapse. Emergent decompression is typically performed in the prehospital or hospital settings in cases in which a tension pneumothorax is suspected, without relying on other diagnostic modalities to confirm its presence. References 1. Steier M, Ching N, Roberts EB, Nealon TF Jr: Pneumothorax complicating continuous ventilatory support. J Thorac Cardiovasc Surg 1974, 67:17–23. 2. Plewa MC, Ledrick D, Sferra JJ: Delayed tension pneumothorax complicating central venous catheterization and positive pressure ventilation. Am J Emerg Med 1995, 13:532–535. 3. Zaugg M, Stoehr S, Weder W, Zollinger A: Accidental pleural puncture by a thoracic epidural catheter. Anaesthesia 1998, 53:69–71. 4. Kaye AD, Eaton WM, Jahr JS, Nossaman BD, Youngberg JA: Local anesthesia infiltration as a cause of intraoperative tension pneumothorax in a young healthy woman undergoing breast augmentation with general anesthesia. J Clin Anesth 1995, 7:422–-424. 5. Perez JE, Alberts WM, Mamel JJ: Delayed tension pneumothorax after laparoscopy. Surg Laparosc Endosc 1997, 7:70–72. 6. Dawson R, Ferguson CJ: Life-threatening tension pneumothorax during laparoscopic cholecystectomy. Surg Laparosc Endosc 1997, 7:271–272. 7. Berrouschot J, Oeken J, Steiniger L, Schneider D: Perioperative complications of percutaneous dilation tracheostomy. Laryngoscope 1997, 107:1538–1544. 8. Mitlehner W, Friedrich M, Dissmann W: Value of computer tomography in the detection of bullae and blebs in patients with primary spontaneous pneumothorax. Respiration 1992, 59:221–227. 9. Light RW: Pneumothorax. In Pleural Diseases, edn 3. Edited by Light RW. Baltimore: Williams & Wilkins; 1995:242– 277. 10. Rutherford RB, Holcombe HH, Brickman RD, Tubb JM: The pathophysiology of progressive tension pneumothorax. J Trauma 1968, 8:212–227. 11. Simmons DH, Hemingway A, Ricchiuti N: Acute circulatory effects of pneumothorax in dogs. J Appl Physiol 1958, 12:255–261. 12. Kilburn KH: Cardiorespiratory effects of large pneumothorax in conscious and anesthetized dogs. J Appl Physiol 1963, 8:279–283. 13. Maloney JV Jr, Schmutzer KJ, Raschke E: Paradoxical respiration and “pendelluft.” J Thorac Cardiovasc Surg 1961, 41:291–298. 14. Bennett RA, Orton EC, Tucker A, Heiiler CL: Cardiopulmonary changes in conscious dogs with induced progressive pneumothorax. Am J Vet Res 1989, 50:280–284. 15. Gustman P, Yerger L, Warner A: Immediate cardiovascular effects of tension pneumothorax. Am Rev Respir Dis 1983, 127:171–174. 16. Carvalho P, Hilderbrandt J, Charan NB: Changes in bronchial and pulmonary arterial blood flow with progressive tension pneumothorax. J Appl Physiol 1996, 81:1664–1669. 17. Barton ED, Rhee P, Hutton KC, Rosen P: The pathophysiology of tension pneumothorax in ventilated swine. J Emerg Med 1997, 15:147–153. 18. Mount LE, Ingram DL: The Pig as a Laboratory Animal. New York: Academic Press; 1971:65–90. 19. Britten S, Palmer SH: Chest wall thickness may limit adequate drainage of tension pneumothorax by needle thoracocentesis. J Accid Emerg Med 1996, 13:426–427. 20. Pattison GT: Needle thoracocentesis in tension pneumothorax: insufficient cannula length and potential failure [letter]. Injury 1996, 27:758. 21. American College of Surgeons: Advanced Trauma Life Support, edn 4. Chicago, IL: in press. 22. Barton ED, Epperson M, Hoyt DB, Fortlage D, Rosen P: Prehospital needle aspiration and tube thoracostomy in trauma victims: a six-year experience with aeromedical crews. J Emerg Med 1995, 13:155–163. 23. Coats TJ, Wilson AW, Xeropotamous N: Pre-hospital management of patients with severe thoracic injury. Injury 1995, 26:581–585. 24. Deakin CD, Davies G, Wilson A: Simple thoracostomy avoids chest drain insertion in prehospital trauma. J Trauma 1995, 39:373–374.