Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
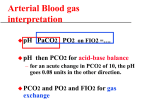
Infectious Etiology of Acute Exacerbations of Chronic Bronchitis* Sanjay Sethi, MD Infectious agents are a major cause of acute exacerbations of chronic bronchitis (AECB) and COPD. Several respiratory viruses are associated with 30% of exacerbations, with or without a superimposed bacterial infection. Atypical bacteria, mostly Chlamydia pneumoniae, have been implicated in < 10% of AECB. The role of bacterial pathogens when isolated from the respiratory tract during AECB has become better defined by application of several newer investigative techniques. Bacterial pathogens can be isolated in significant concentrations from distal airways in 50% of AECB. Specific immune responses to surface exposed antigens of the infecting pathogen have been shown to develop after an exacerbation. Emerging evidence from molecular epidemiology and measurement of airway inflammation further support the role of bacteria in AECB. When properly defined, 80% of AECB are likely to be infectious in origin. (CHEST 2000; 117:380S–385S) Key words: chronic bronchitis; COPD; exacerbation; infection Abbreviations: AECB ⫽ acute exacerbations of chronic bronchitis; NTHI ⫽ nontypeable Haemophilus influenzae; OMP ⫽ outer membrane protein; PSB ⫽ protected specimen brush OPD is a chronic disabling disease. It is characC terized by intermittent acute exacerbations of chronic bronchitis (AECB) associated with worsening symptoms and lung function. These acute exacerbations contribute considerably to the morbidity and the diminished quality of life experienced by people afflicted with COPD.1 AECB are an important cause of mortality, and in a longitudinal study of a cohort of patients with moderate to severe COPD, lower respiratory tract infection was the most common identified cause of death.2 Several etiologic factors alone or in combination cause exacerbations of COPD.3 One major etiologic factor discussed in this article is infection of the lower respiratory tract. Although recognized for several decades, several new lines of evidence utilizing newer research techniques have improved our understanding of the role of infection in acute exacerbations. Definition and Diagnosis The most commonly used definition of an acute exacerbation of chronic bronchitis is a subjective *From the Department of Medicine, Division of Pulmonary and Critical Care Medicine, State University of New York at Buffalo and Department of Veterans Affairs Western New York Healthcare System, Buffalo, NY. Supported by VA Merit Review. Correspondence to: Sanjay Sethi, MD, Veterans Affairs Western New York Healthcare System (151), 3495 Bailey Ave, Buffalo, NY 14215; e-mail: [email protected] 380S increase from baseline of one or more chronic symptoms. These symptoms include shortness of breath, cough, sputum production, sputum purulence, and sputum tenacity. Several other disorders can cause such an increase in symptoms and need to be excluded with reasonable certainty by the evaluating clinician. Differential diagnoses include pneumonia, congestive heart failure, myocardial ischemia, upper respiratory tract infection, pulmonary embolism, recurrent aspiration, and noncompliance with medications.3 In most circumstances, a thorough history and examination are adequate to make the diagnosis. Occasionally, a chest radiograph or ECG is required. Sputum studies are not useful in most episodes of AECB except in certain circumstances, such as recurrent AECB, inadequate response to therapy, and before starting treatment with prophylactic antibiotics. Infectious Etiologies of AECB Three classes of pathogens have been implicated as causing acute exacerbation of COPD by infecting the lower respiratory tract: respiratory viruses, atypical bacteria, and aerobic Gram-positive and Gramnegative bacteria.4 The relative contributions of these three different classes of pathogens may change depending on the severity of the underlying obstructive airway disease. Such changes may also happen within a class, especially for bacterial pathogens. COPD: Working Towards a Greater Understanding Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 Respiratory Viruses Several longitudinal studies of groups of COPD patients in the 1970s examined the role of viruses in causing acute exacerbations of COPD.5–7 Viral infection in these studies was usually documented by serology and occasionally by culture. In these studies, about 30% of the episodes of AECB were associated with viral infection. Asymptomatic viral infections (diagnosed by fourfold rise in specific antibody titers) were also seen, but the incidence of viral infection in association with exacerbations was significantly greater than during stable periods.5 Figure 1 is a composite of incidence data for specific viral pathogens from three longitudinal studies.5–7 Significant incidence of influenza virus as a cause of AECB stresses the importance of yearly influenza immunization in patients with COPD. In a more recent cross-sectional study, Soler et al8 studied 50 episodes of severe AECB requiring ICU admission and mechanical ventilation. In 38 episodes, adequate paired serologic samples were available for analysis. Viral infection was present in six of these episodes (15.8%), influenza in five episodes, and respiratory syncytial virus in one episode. Interestingly, in three of the five influenza infections, a concomitant pathogen was present. This study would suggest that viral infection decreases in importance in the most severe end of the spectrum of AECB, and is often complicated by concomitant bacterial infection. Atypical Bacteria In recent years, we have seen an increasing recognition of the role of atypical bacterial pathogens in acute bronchitis and community-acquired pneumonia. However, in AECB, several older studies and a few recent studies have implicated atypical bacteria in only 5 to 10% of episodes. Legionella does not appear to cause an isolated bronchial infection, with pneumonic infiltrates invariably associated with its isolation from the lower respiratory tract. Mycoplasma pneumoniae infection has been shown to be a rare cause of AECB.5– 8 Chlamydia pneumoniae has been associated with AECB in 5 to 10% of cases.9,10 In the study of severe exacerbations requiring intensive care by Soler et al,8 C pneumoniae infection was present in 7 of 38 evaluable cases (18%), but a concomitant bacterial pathogen was present in two of these patients. No Mycoplasma infection was documented in these patients. Bacteria Bacteria are isolated from sputum in 40 to 60% of AECB. The three predominant bacterial species isolated are nontypeable Haemophilus influenzae (NTHI), Moraxella catarrhalis, and Streptococcus pneumoniae. Whether this isolation represents infection of the lower airway causing AECB has been a controversial issue for several decades. In the 1950s and 1960s, the British hypothesis included bacterial exacerbations along with mucus hypersecretion as major contributors to the pathogenesis of COPD. With the realization of the central role of tobacco smoke exposure and the emergence of evidence that mucus hypersecretion and worsening airway obstruction were not linked, this hypothesis fell into disfavor. Several longitudinal studies in the 1960s and 1970s demonstrated that the incidence of bacterial isolation during exacerbations of COPD was not different from the incidence during stable COPD. Serologic studies conducted in the same time period compared serum antibody titers to airway bacterial pathogens such as NTHI in COPD patients to titers in control subjects. These studies yielded confusing and contradictory results (reviewed in Murphy and Sethi11). As a consequence of these observations, bacterial infection was discounted as a cause of AECB, with the supposition that isolation of bacteria from sputum represents chronic colonization, an “innocent bystander” role.12 In the last decade, several new lines of evidence have emerged that have reexamined this issue using either new diagnostic modalities or research techniques (Table 1). These new lines of Table 1—New Approaches to Understanding the Role of Bacteria in COPD Exacerbations Figure 1. Viral pathogens that cause acute exacerbations of COPD. RSV ⫽ respiratory syncytial virus. Reprinted with permission from Sethi.4 Bronchoscopic sampling of the lower respiratory tract Immune response to bacterial pathogens in AECB Molecular epidemiology of bacterial pathogens Airway inflammation measurement and correlation with bacteriology CHEST / 117 / 5 / MAY, 2000 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 381S evidence support the role of bacterial infection as a cause of AECB and will be discussed below. Bronchoscopic Sampling of Lower Respiratory Tract in AECB An attractive approach to understanding the role of bacterial infection in AECB is sampling of distal airway secretions for quantitative culture by protected specimen brush (PSB) or by BAL to determine bacterial concentrations in the distal airways. Such an approach has contributed tremendously to our understanding of nosocomial pneumonia. Four studies have been published that have used this methodology, and all of them have shown significant bacterial infection of the distal airways in approximately 50% of patients (Table 2).8,13–15 The bacterial species isolated in these studies represent the same spectrum of pathogens commonly isolated from sputum cultures of patients with AECB. The study of Monso et al13 is especially informative, as it included a control group of 29 patients with stable COPD. Figure 2 demonstrates that AECB was associated twice as often with distal airway infection with ⱖ 103 cfu/mL of pathogenic bacteria, and four times as often with ⱖ 104 cfu/mL of pathogenic bacteria. Soler et al8 examined a more severe population of 50 patients, who received mechanical ventilation for an AECB, and obtained lower airway Figure 2. Culture results of PSB samples from patients with stable COPD or with acute exacerbations. Reprinted with permission from Sethi.4 secretions for culture by bronchoscopy with PSB, BAL, and endotracheal aspirates. A major drawback of their study was that 21 of their 50 patients had received antibiotics prior to the samples being obtained for bacterial cultures. In spite of that, bacterial infection was demonstrated alone in 21 of 50 patients (42%) and with a viral or atypical pathogen in 7 patients (14%). The distribution of the bacterial pathogens isolated in their study is remarkable for the high Table 2—Bronchoscopic Studies in AECB Study Subjects Diagnostic Methods % Bacterial Pathogen Positive Bacterial Pathogens Isolated, No. Haemophilus parainfluenzae, 11 S pneumoniae, 7 H influenzae, 6 M catarrhalis, 3 P aeruginosa, 3 Other Gram-negative, 5 Other Gram-positive, 9 H influenzae, 10 S pneumoniae, 3 P aeruginosa, 2 M catarrhalis, 2 H influenzae, 11 P aeruginosa, 9 S pneumoniae, 4 M catarrhalis, 4 Other Gram-negative, 6 S pneumoniae, 10 Alpha-hemolytic streptococci, 6 M catarrhalis, 2 H influenzae, 1 P aeruginosa, 1 Other Gram-negative, 1 Other Gram-positive, 1 Fagon et al14 50 ICU patients receiving mechanical ventilation PSB 50* Monso et al13 29 outpatients PSB 51.7 Soler et al8 50 ICU patients receiving mechanical ventilation† PSB, BAL, endotracheal aspirate 46 Pela et al15 40 outpatients PSB 52.5 *ⱖ102 cfu/mL was used to define a positive culture, instead of the usual ⱖ103 cfu/mL. †Twenty-one patients had antimicrobial therapy in the 24 h prior to admission to the ICU. 382S COPD: Working Towards a Greater Understanding Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 incidence of Pseudomonas aeruginosa and other Gramnegative bacilli (14 of 50 patients; 28%). Another study, by Eller et al,16 utilizing sputum cultures has also demonstrated an increasing frequency of isolation of these groups of pathogens in exacerbations of severe COPD. Whether this is due to environmental factors (such as antibiotic selection pressure or exposure to hospital flora from frequent exacerbations) or is related to a greater degree of host immune compromise is not clear. The remarkably consistent results of these four studies and the increased rate of isolation of pathogenic bacteria in AECB than in stable COPD support the pathogenic role of bacteria in a proportion of AECB. Immune Responses to Bacterial Pathogens in AECB Demonstration of the development of an immune response to an infecting pathogen satisfies one of the Koch postulates. Several studies in the 1950s and 1960s attempted to demonstrate that patients with COPD have increased serum antibody titers to NTHI as compared to control subjects without COPD. These studies yielded confusing and contradictory results that could be attributed to the limitation of the methods in these studies, such as using a single laboratory strain of NTHI and measuring antibody levels to whole bacteria.11 We recently studied the immune response to NTHI in two patients who had experienced an AECB with methods that would avoid the shortcomings of earlier studies.17 NTHI strains used in these studies were homologous infecting strains, and the immunoassays used were specific for antibodies to surface-exposed epitopes. In addition, as these patients are part of a longitudinal study, we were able to study paired sera collected 1 month prior to the exacerbation (preserum) and sera collected a month after the onset of the AECB (postserum). In both patients, the postserum demonstrated bactericidal activity to the homologous strain that was absent in the preserum. Immunoblots with purified outer membrane proteins (OMPs) of the homologous NTHI strains did not reveal significant differences between the presera and postsera indicating development of new antibodies. However, in a radioimmunoprecipitation assay, an immunoassay specific for antibodies to surface-exposed epitopes, the postsera demonstrated development of new antibodies to surface-exposed epitopes of OMP P2 and a high molecular weight OMP of the homologous strains. We were able to demonstrate further that the new antibodies to OMP P2 were responsible for a substantial proportion of the bactericidal activity in the postsera. OMP P2 of NTHI has been shown to have several hypervariable regions on the surface of the bacteria.18 This explains why these bactericidal antibodies were strain-specific for the homologous infecting strain. Development of a specific immune response to the infecting strain of NTHI in this study supports the role of bacterial infection in AECB. Similar evidence with other bacterial species implicated in AECB (see Table 2) would help us better define their role in acute exacerbations. Molecular Epidemiology of Bacterial Pathogens There is increasing recognition that strains of a bacterial species differ considerably in their surface antigenic structure. Earlier reports in which the incidence of bacterial infection during stable and periods of exacerbation of COPD have been compared assumed that all strains of a bacterial species are the same, and that bacterial infection of the lower respiratory tract in COPD is a static process.5 In preliminary studies, we have performed strain typing for NTHI in patients with COPD.19 What has become apparent is that there is a dynamic turnover in these patients of NTHI strains, and there appears to be an association between this dynamic process and the occurrence of AECB. Therefore, a simple comparison of the frequency of isolation of a bacterial species in these patients is inadequate, and application of molecular epidemiology to bacterial isolates from COPD patients is necessary to further elucidate the role of bacterial infection. Airway Inflammation Measurement and Correlation With Bacteriology Bacterial infection of the lower airways during an episode of AECB should be associated with neutrophilic inflammation, as is seen in other mucosal sites such as the middle ear and sinuses. One would therefore expect bacterial exacerbations to be associated with significantly greater neutrophilic airway inflammation than nonbacterial exacerbations. Therefore, sputum culture results should correlate with measures of airway inflammation in AECB. Preliminary data from our laboratory support this hypothesis, with pathogen-positive AECB having substantially increased measures of airway inflammation in expectorated sputum than pathogen-negative AECB.20 Model of Recurrent NTHI Infection in COPD Patients with COPD have recurrent infections with NTHI, which clinically manifest as associated CHEST / 117 / 5 / MAY, 2000 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 383S with increasing symptoms (exacerbation), or without an acute change in symptoms (colonization). Based on emerging evidence that NTHI infection in COPD is a dynamic process and the immune response to infecting strains is predominantly strain specific, we can hypothesize a model to explain recurrent NTHI infections in patients with COPD (Fig 3). The factors that determine the clinical manifestations of an acquisition of a new NTHI strain by a patient with COPD are unknown. In this model, virulence of the infecting strain and the presence of preexisting protective antibody are assumed to be important factors. Absence or a low level of protective antibodies and/or a virulent strain predisposes to development of increased symptoms, ie, an exacerbation, with the opposite predisposing to an acquisition without increased symptoms, ie, a colonization. Exacerbation (and possibly colonization) leads to development of antibodies to the infecting strain, which, with or without antibiotics, successfully clear it from the lower respiratory tract. However, as a substantial proportion of these antibodies are directed to hypervariable regions of OMPs (such as P2), these antibodies are strain specific and do not protect the host from NTHI strains that are antigenically different (Fig 3). Such strains then replace the previous strain in a repetitive manner. This model would suggest that identifying virulence factors in NTHI strains and identifying antigens on the surface of NTHI that are shared among several strains and can elicit a protective antibody response are important areas of research. Conclusion When strictly defined as suggested above, it is likely that 80% of AECB are infectious in origin, with Figure 3. Model of recurrent infection by NTHI in patients with COPD. 384S 40 to 50% caused by bacteria, 30% by viruses, and 5 to 10% by atypical bacteria. Concomitant infections by more than one infectious pathogen appear to occur in 10 to 20% of patients. Several lines of evidence demonstrate bacterial infection to be a cause of AECB. Tracheobronchial airway infection in COPD is a complex dynamic process. Understanding this process and the host immune response to it should lead to new ways of abrogating these infections. References 1 Seemungal TA, Donaldson GC, Paul EA, et al. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1998; 157:1418 –1422 2 Burrows B, Earle RH. Course and prognosis of chronic obstructive lung disease: a prospective study of 200 patients. N Engl J Med 1969; 280:397– 404 3 American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77–S120 4 Sethi S. Management of acute exacerbations of chronic bronchitis. Infect Dis Clin Pract 1998; 7:S300 –S308 5 Gump DW, Phillips CA, Forsyth BR, et al. Role of infection in chronic bronchitis. Am Rev Respir Dis 1976; 113:465– 473 6 Buscho RO, Saxtan D, Shultz PS, et al. Infections with viruses and Mycoplasma pneumoniae during exacerbations of chronic bronchitis. J Infect Dis 1978; 137:377–383 7 Smith CB, Golden C, Kanner R, et al. Association of viral and Mycoplasma pneumoniae infections with acute respiratory illness in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis 1980; 121:225–232 8 Soler N, Torres A, Ewig S, et al. Bronchial microbial patterns in severe exacerbations of chronic obstructive pulmonary disease (COPD) requiring mechanical ventilation. Am J Respir Crit Care Med 1998; 157:1498 –1505 9 Blasi F, Legnani D, Lombardo VM, et al. Chlamydia pneumoniae infection in acute exacerbations of COPD. Eur Respir J 1993; 6:19 –22 10 Miyashita N, Niki Y, Nakajima M, et al. Chlamydia pneumoniae infections in patients with diffuse panbronchiolitis and COPD. Chest 1998; 114:969 –971 11 Murphy TF, Sethi S. Bacterial infection in chronic obstructive pulmonary disease. Am Rev Respir Dis 1992; 146:1067– 1083 12 Tager I, Speizer FE. Role of infection in chronic bronchitis. N Engl J Med 1975; 292:563–571 13 Monso E, Ruiz J, Rosell A, et al. Bacterial infection in chronic obstructive pulmonary disease: a study of stable and exacerbated outpatients using the protected specimen brush. Am J Respir Crit Care Med 1995; 152:1316 –1320 14 Fagon J-Y, Chastre J, Trouillet J-L, et al. Characterization of distal bronchial microflora during acute exacerbation of chronic bronchitis. Am Rev Respir Dis 1990; 142:1004 –1008 15 Pela R, Marchesani FF, Agostinelli C, et al. Airways microbial flora in COPD patients in stable clinical conditions and during exacerbations: a bronchoscopic investigation. Monaldi Arch Chest Dis 1998; 53:262–267 16 Eller J, Ede A, Schaberg T, et al. Infective exacerbations of chronic bronchitis: relation between bacteriologic etiology and lung function. Chest 1998; 113:1542–1548 COPD: Working Towards a Greater Understanding Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 17 Yi K, Sethi S, Murphy T. Human immune response to nontypeable Haemophilus influenzae in chronic bronchitis. J Infect Dis 1997; 176:1247–1252 18 Sikkema DJ, Murphy TF. Molecular analysis of the P2 porin protein of nontypeable Haemophilus influenzae. Infect Immunol 1992; 60:5204 –5211 19 Sethi S, Muscarella K, Murphy TF. Dynamics of respiratory tract colonization by nontypeable Haemophilus influenzae in patients with COPD [abstract 185]. Presented at: American Society for Microbiology General Meeting; May 19 –23, 1996; New Orleans, LA 20 Sethi S, Muscarella K, Evans N, et al. Comparison of airway inflammation in acute bacterial and non-bacterial exacerbations of COPD [abstract 822]. Presented at: American Thoracic Society/American Lung Association International Conference; April 23–28, 1999; San Diego, CA CHEST / 117 / 5 / MAY, 2000 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21947/ on 05/10/2017 385S