Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
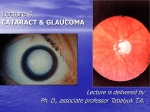
Management of Combined Phacolytic/Phacomorphic Glaucoma as a Complication of Nd:YAG Laser Peripheral Iridotomy in a Patient with Mature Cataract K. Camille DiMiceli, MD Herbert J. Ingraham, MD Department of Ophthalmology, Geisinger Health System Danville, PA Authors have no financial interest Purpose/Methods: To discuss the management of a complicated phacolytic/ phacomorphic glaucoma case incited by Nd:YAG laser peripheral iridotomy with accidental disruption of the anterior capsule. A retrospective study of the patient’s chart was performed as well as photo documentation. The patient was followed over the course of several weeks before and after cataract surgery. Case Presentation An 87 year old female with a history of mature cataracts, narrow angle glaucoma, and chronic macular holes OU presents with severe right eye pain, nausea and vomiting. Yag:Nd LPI was performed OD at an outside office for narrow angle one day prior. Leakage of white milky material was noted from LPI site post laser. Patient was referred to Geisinger for further management. Exam: Va: OD: CF at ½ foot; OS: CF at 1 foot Pressure: OD: 62mmHg; OS: 8mmHg Pupils: OD: 3mm, fixed and mid-dilated, extensive synechiae; OS: 3mm reactive Conj: 1+ injection OU Cornea: OD: 1+ edema OS: clear AC: OD: very shallow; crystalline material; OS: narrow angle Iris: OU: patent PI superiorly; OD with white crystalline material Lens: OD: fluffy cortical material with 4+brunescent nucleus; OS: 4+ brunescent cataract Fundus: OU: no view Pathophysiology Our patient had refused cataract surgery in the past because of multiple medical problems and poor visual prognosis secondary to bilateral chronic macular holes. The mature intumescent lenses that developed caused phacomorphic angle closure glaucoma. Traumatic rupture of the anterior capsule with Yag:Nd laser released high molecular weight proteins, which blocked the trabecular meshwork and caused acute severe elevated IOP. (4,7) Macrophages are the main cellular component of the AC reaction that ensues upon release of the lens proteins. 7 Treatment: Medical Therapy: It is recommend to always attempt to lower IOP and allow time for inflammation to subside prior to lens removal. Our treatment consisted of the following: Topical beta-adrenergic antagonist Oral carbonic anhydrase inhibitors (Acetazolamide) are faster and slightly more effective than topical agents. There is no additive effect of using the two together. When using Acetazolamide, the 250mg tabs act more quickly than 500mg sustained release caps. Aggressive topical steroids to quell inflammation Mydriatic v. Miotic: We used Pilocarpine which took effect once the IOP was under better control. Miotics can theoretically worsen IOP by increasing pupillary block and anterior displacement of the lens-iris diaphragm. Mydriatics can worsen angle closure, but are helpful for use prior to surgery. There is no clinical difference when either agent is used. 5 IV Mannitol is the next step, but was not necessary in our case. Surgical Options: Removal of the inciting lens and debris is the definitive treatment of lens induced glaucomas. We were able to stabilize the patient and manage medically for one week prior to surgery. ICCE was historically done to prevent phacoanaphylaxis, 1 but was replaced by ECCE as early as 1957. ECCE is the most commonly performed procedure.4 Peripheral iridectomy is not necessary if a PCIOL is placed and there are no significant PAS. 5 Phacoemulsification may be appropriate if the view is sufficient, if the zonules are secure, and the lens is not excessively dense. MSICS (manual small incision cataract surgery) is advocated as a safe, efficient and cost-effective treatment in developing countries. 8 Spontaneous recovery: uncommon, but reported in patient who refused surgery. 3 Surgery: In our patient we chose to do ECCE with iris stretch based on the presence of the following: An extremely dense mahogany nucleus Extensive synechiae from chronic angle closure Poorly dilating pupil Ruptured anterior capsule ECCE was performed on the fellow eye to treat the phacomorphic glaucoma. Results: Final Results: on Travatan qhs OU OD: BCVA: 4/400 (large stage 4 macular hole) IOP: 12mmHg OS: BCVA: 20/50+ (small stage 4 macular hole); IOP: 12mmHg Conclusions: In lens induced glaucomas the preoperative IOPs are markedly elevated (generally 40mmHg and higher) and visual acuity can be quite poor (average HM-LP). 5 Despite this dismal presentation, after lens extraction the IOP can be adequately controlled, often without medication, and the vision can be restored if there is no other significant ocular pathology. In the management of this case we systematically went through our armamentarium of medications to control IOP and inflammation prior to and in preparation for the definitive treatment of cataract extraction. When possible, medical therapy should be used to temporize this tenuous condition and to create a safer surgical environment. References: 1. Mandal AK and Gothwal VK. “Intraocular Pressure Control and Visual Outcome in Patients with Phacolytic Glaucoma Managed by Extracapsular Cataract Extraction with or without Posterior Chamber Intraocular Lens Implantation.” Ophthalmic Surgery and Lasers, Nov. 1998, vol 29, no. 11, pp 880-889. 2. Epstein David. “Diagnosis and Management of Lens-induced Glaucoma. Ophthalmology, Mar 1982, vol 89, no. 3 pp 227-229. 3. Blaise P, Duchesne B, Guillaume S and Galand A. “Spontaneous Recovery in Phacolytic Glaucoma.” Journal of Cataract and Refractive Surgery, Sept 2005, vol 31, pp 1829-1830. 4. Lane S, Kopietz L, Lindquist T, Leavenworth N. “Treatment of Phacolytic Glaucoma with Extracapsular Cataract Extraction.” Ophthalmology, June 1988, vol. 95, no. 6, pp 749753. 5. McKibbin M, Gupta A, Atkins AD. “Cataract Extraction and Intraocular Lens Implantation in Eyes with Phacomorphic or Phacolytic Glaucoma.” Journal of Cataract and Refractive Surgery, June 1996, vol. 22, 633-636. 6. Rosenberg LF, Krupin T, Tang LiQi, Hong PH, Ruderman JM. “Combination of Systemic Acetazolamide and Topical Dorzolamide in Reducing Intraocular Pressure and Aqueous Humor Formation.” Ophthalmology, vol. 105, no. 1, pp 88-92. 7. Ueno H, Tamai A, Iyota K, and Moriki T. “Electron Microscopic Observation of the Cells Floating in the Anterior Chamer in a Case of Phacolytic Glaucoma.” Japanese Journal of Ophthalmology, vol 33: 103-113, 1989. 8. Venkatesh R, Tan CSH, Kumar TT, Ravindran RD. “Safety and Efficacy of Manual Small Incision Cataract Surgery for Phacolytic Glaucoma.” British Journal of Ophthalmology 2007, 91: 279-281.