Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
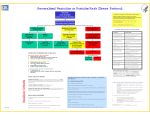
In The Name of God Background: Varicella, commonly known in the United States as Chickenpox Varicella-zoster virus. Generally is a mild self-limiting viral illness with occasional complications varicella is not totally benign A recent study : 1 in 50 cases are associated with complications most dreaded are varicella pneumonia and encephalitis The vaccination against varicella in 1995, which reduced morbidity and mortality Varicella is common and highly contagious and nearly all susceptible children affects before adolescence. Household Transmission rates are 80-90% Second Cases often are more severe Maximum Transmission late winter and spring. Pathophysiology: The varicella-zoster virus enters through the respiratory system and colonizes the upper respiratory tract The virus initially replicates in the regional lymph nodes,the spleen, liver, and .... Frequency: Internationally: Varicella affects nearly all children who do not have immunity. Annual incidence is estimated at 80-90 million cases. Mortality/Morbidity: In healthy children aged 1-14 years, the mortality rate is estimated at 2 deaths per 100,000 cases. Most deaths : encephalitis, pneumonia, secondary bacterial infection, and Reye syndrome. The disease can be serious in neonates, depending on the timing of infection in the mother. Race: Varicella has no racial predilection. Sex: Varicella has no sex predilection. Age: Maximum incidence of varicella is in children aged 1-6 years Persons older than 14 years account for 10% of varicella cases. CLINICAL History: Exposure Varicella spreads primarily by airborne Respiratory droplets. Most patients have a History of Exposure in the home, daycare center, or school. Varicella's incubation period typically is 10-14 days, it may to 21 days. Prodrome Low-grade fever preceding skin manifestations by 1-2 days Complaints of abdominal pain by some children Rash, usually starting on the head and trunk and spreading to the rest of the body intense pruritus Headache Malaise Anorexia Cough and coryza Sore throat Physical: Rash healthy child usually has 250-500 lesions but may have as few as 10 or as many as 1500. starts as a red macule and passes through stages of papule, vesicle, pustule, and crust. Redness or swelling around a lesion should lead to suspicion of bacterial superinfection. Varicella's hallmark is the simultaneous presence of different stages of the rash. Some lesions may appear in the oropharynx. Eye lesions are rare. New lesions continue for 3-5 days. Lesions usually crust by 6 days (2- to 12-d range), and heal completely by 16 days (7to 34-d range). Prolonged eruption of new lesions or delayed crusting and healing can occur with impaired cellular immunity. Fever Fever usually is low-grade but occasionally may be high healthy children, fever typically subsides within 4 days. Prolonged fever should prompt suspicion of complication or immunodeficiency. Outcomes : Congenital varicella syndrome Congenital varicella syndrome occurs in 2% of children born to women who develop varicella during Fetal injury risk is unrelated to the severity of disease in the mother. Zoster exposure during pregnancy has not been associated with fetal injury. Infantile zoster : Infantile zoster usually manifests within the first year. The cause is maternal varicella infection after the 20th week of gestation. Infantile zoster commonly involves the thoracic dermatomes. Transmission Transmission occurs mainly by respiratory droplets containing the virus, making the disease highly contagious even before the rash appears. Papules and vesicles, have high populations of the virus. Varicella's infectious period begins 2 days before skin lesions appear and ends when the lesions crust. Direct person-to-person contact with lesions also spreads the virus. Risk factors for severe varicella A neonate's first month of life, especially if the mother is seronegative. Delivery before 28 weeks of gestation Adolescence and adulthood Steroid therapy: High doses (1-2 mg/kg/d of prednisolone) for 2 weeks. Even short-term therapy Malignancy: The risk is highest for children with leukemia. Almost 30% of patients who are immunocompromised Immunocompromised state (eg, malignancy, antimalignancy drugs, HIV, other congenital or acquired immunodeficient conditions( Pregnancy:, especially pneumonia. DIFFERENTIALS Drug reactions Insect bites WORKUP Lab Studies: unnecessary for diagnosis because varicella is obvious clinically. Most children with varicella have leukopenia in the first 3 days, followed by leukocytosis. Marked leukocytosis may indicate a secondary bacterial infection Most children with significant secondary bacterial infections do not have leucocytosis. Imaging Studies: Chest x-ray Children with high temperatures and respiratory signs should have a chest x-ray to confirm or exclude pneumonia. Chest x-ray findings may be normal or may show diffuse bilateral nodular infiltrates in primary varicella pneumonia. X-rays also may detect of secondary bacterial pneumonia. Other Tests: Lumbar puncture Children with neurological signs should have their (CSF) examined. The CSF of varicella encephalitis may have few or as many as a hundred cells that are polymorphonuclear or mononuclear, depending on the timing of the lumbar puncture. Glucose levels are normal. Protein levels are normal or slightly raised. TREATMENT Medical Care: Manage Pruritus with cool compresses and regular bathing. Trimming the child's Fingernails and having the child wear mittens while sleeping may reduce scratching. Consultations: Consult with an infectious disease specialist in the following situations: Progressive or severe varicella Life-threatening complications (eg, encephalitis, pneumonia) Serious secondary bacterial infections, especially group A streptococcal superinfections, which may evolve rapidly into necrotizing fasciitis and toxic shock syndrome Children who develop severe and life-threatening varicella complications may require hospitalization in an ICU Diet: full and unrestricted diet to the child. take sufficient fluids to maintain hydration. Adequate hydration is especially important if the child is receiving acyclovir Activity: No activity restrictions are needed for young children with uncomplicated varicella. MEDICATION Antivirals -- Chickenpox is not always benign. Antiviral drugs are recommended for adolescents, adults, and children on steroid or salicylate therapy and for children who are immunocompromised. Acyclovir is the only adequately studied drug of this class. Antipyretics -- Fever usually is low grade but may be elevated. Acetaminophen probably is the safest drug to use for this purpose. Salicylate usage for varicella is associated with Reye syndrome (NSAIDs) have been suspected of suppressing immune function and promoting infection progress in patients infected with invasive group A streptococci. FOLLOW-UP Further Inpatient Care: Indications for admission to ICU/neonatal ICU Altered consciousness Seizures Difficulty walking Respiratory distress Cyanosis Low oxygen saturation Hospitalize and treat all newborns whose mothers developed varicella less than 5 days before or within 2 days after delivery. Prevention: Vaccination Varicella vaccine consists of live attenuated. The vaccine is safe and highly immunogenic. Protection from 71-100% and is likely to be long term. Breakthrough varicella is mild when it occurs. The vaccine is effective when administered on or after the age of 1 year. Only a single dose is recommended for children younger than 13 years. For older children, the recommended dosage is 2 doses separated by 4-8 weeks. Postexposure prophylaxis, if provided within 72 hours of contact, can prevent or attenuate disease in the exposed individual. Varicella-zoster immune globulin VZIG is used as postexposure prophylaxis in highrisk individuals. Administration as soon as possible after exposure is best, but VZIG can prevent or attenuate varicella if administered within 96 hours of contact. The dose is 125 U/10 kg body weight; 125 U is the minimum dose. Maximum dose is 625 IU. VZIG is administered IM, never IV. The expected duration of protection is approximately 3 weeks. Newborns of mothers who acquired varicella 5 days before to 2 days after delivery Persons with HIV, AIDS, or other immunodeficiency disorders Persons receiving drugs that suppress immune function (eg, systemic steroids) Pregnant women Complications: Secondary bacterial infections rapidly spreading cellulitis, septicemia, and other serious infections may occur. The most common infectious organisms are group A streptococci and Staphylococcus aureus. Signs and symptoms of secondary bacterial infection can be during the first 3-4 days. Suspect secondary infection when systemic manifestations do not improve in 3-4 days, the fever returns or worsens, or the child's condition deteriorates after initial improvement. CNS complications Acute postinfectious cerebellar ataxia is the most common CNS complication Ataxia has sudden onset that usually occurs 2-3 weeks after the onset of varicella. The condition may persist for 2 months. The prognosis for patients with ataxia is good, but a few children may have residual ataxia, incoordination Encephalitis occurs in 1.7 patients per 100,000 cases. The disease manifests during acute varicella a few days after rash onset. Lethargy, drowsiness, and confusion are the usual presenting symptoms. seizures, deep coma. 5-20% mortality rate. Reye syndrome aseptic meningitis, Guillain-Barré syndrome Pneumonia: Pneumonia occurs primarily among older children and adults and can have a fatal outcome. Respiratory symptoms usually appear 34 days after the rash. Herpes zoster: A delayed complication of varicella, herpes zoster infection, occurs months to years after the primary infection in about 15% of patients. The complication is caused by virus persisting in the sensory ganglions. Otitis media: About 5% of children with varicella Thrombocytopenia Hepatitis is a self-limited , Liver involvement is independent of the severity of skin and systemic manifestations. Glomerulonephritis Hemorrhagic varicella Prognosis: excellent prognoses. Children with immunocompromised states are at risk for severe disease and death (eg, the mortality rate among children with leukemia is 7%). Neonatal varicella mortality rates can reach 30%. Patient Education: Bathe the child regularly to reduce itching and prevent secondary infection. Scratching can lead to secondary infection and scarring. Keep the fingernails short. Wearing mittens or socks on the hands at night can help prevent scratching. Do not use medications containing aspirin. Advise parents to take children to the hospital if the following symptoms occur: Unusual redness, swelling, or pain over an area of the rash Refusal to drink fluids Signs of dehydration Confusion, irritability, drowsiness, or difficulty waking Inability to walk or unusual weakness severe headache, stiff neck, and/or back pain Frequent vomiting Difficulty breathing, chest pain, wheezing, fast breathing, or severe cough Fever persisting more than 4 days or fever returns after defervescence The Pleomorphic Rash characteristic of varicella. Papules, Vesicles, and Pustules exist concurrently.