Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
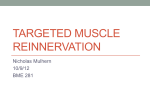
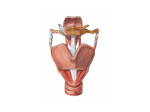
EMG SITE LOCATION USING AN ELECTRODE ARRAY Farrell T.R.1, Hanson W.J. 1, Johannson J.L. 1, Klodd E.J. 1, Edell D.J.2, Sexton S.V. 2, Yuhan, J.A. 2 1 2 Liberating Technologies, Inc., Holliston, MA InnerSea Technology, Inc., Bedford, MA INTRODUCTION Our group is developing a microprocessor-based knee controller that will use myoelectric inputs from the user to assist in the control of the knee joint. While muscle locations are relatively fixed in ablebodied subjects, amputation surgery often causes residual muscles to be located in atypical positions. One challenge is accurately identifying the locations of the residual muscles for electrode placement. the maximum EMG signal was rarely more than 2 cm from the palpated location. METHODS The locations of the residual surface muscles were first palpated and then marked on the surface of the residual thigh. An electrode array consisting of 32 channels of bipolar EMG recordings (bipolar recordings with 4 cm spacing) arranged in roughly a 12 cm diameter circle was placed on the residual limb over the palpated muscle site (Fig. 1) and held in place using an elastic bandage. The user was then asked to perform a movement associated with the targeted muscle. For example, the subject was asked to flex the hip when rectus femoris was targeted. The EMG signals were recorded in real time and used to create a heat map in which larger EMG signals corresponded to ‘hotter’ colors (Fig. 2). The heat map was used to determine the location of the maximum EMG signal. This location was then compared to the palpated location. Figure 2. Heat map created as subject performs hip flexion to activate the rectus femoris. The non-centered red area indicates that largest EMG activity was located near, but not exactly under, the palpated site. DISCUSSION The standard methods of locating EMG sites by iteratively moving an electrode around the surface of a limb assumes that the user is producing the same contraction every time. Our results indicate that being able to view many potential EMG locations simultaneously allows for quick and accurate determination of the locations that produce the maximum EMG amplitudes. While it provided a good estimate, we found that the mechanical displacements created during palpation are not completely indicative of the location of the maximum EMG signal. While this system was developed for finding lower limb muscle sites, we believe a smaller version could also be used to find optimal upper limb sites as well. CONCLUSION The electrode array has proven useful in locating the residual limb sites that create the largest EMG signal. REFERENCE AND CKNOWLEDGEMENTS Figure 1. Muscle sites were palpated and the 32 channel electrode array was centered on the palpated site. RESULTS Results from the first three subjects reveal the largest EMG amplitude was rarely located directly under the palpated site. However, the location that produced U.S. Patent # 5,341,813 “Prosthetic electrode array diagnostic system.” This research and development project was conducted by the QinetiQ North America Technology Solutions Group team and made possible by a contract awarded and administered by the U.S. Army Medical Research & Materiel Command (USAMRMC) and the Telemedicine & Advanced Technology Research Center (TATRC) under contract W81XWH08C0729. American Academy of Orthotists & Prosthetists 37th Academy Annual Meeting and Scientific Symposium March 16-19, 2011