Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
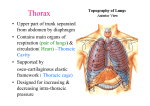
Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy THORACIC WALL, MEDIASTINUM & HEART & PERICARDIUM 27.September.2011 Tuesday THORACIC WALL 1. Thorax The thorax is the part of the body between the neck and abdomen. Posterior surface is formed by the 12 thoracic vertebræ and the posterior parts of the ribs. Anterior surface is formed by the sternum and costal cartilages. Lateral surfaces are formed by the ribs, separated from each other by the intercostal spaces, eleven in number, which are occupied by the intercostal muscles and membranes. The floor of the thoracic cavity is deeply invaginated inferiorly (i.e., is pushed upward) by viscera of the abdominal cavity. Regions • Thoracic wall • Thoracic cavity The thorax includes the primary organs of the respiratory and cardiovascular systems. The majority of the thoracic cavity is occupied by the lungs, which provide for the exchange of oxygen and carbon dioxide between the air and blood. Most of the remainder of the thoracic cavity is occupied by the heart and structures involved in conducting the air and blood to and from the lungs. Additionally, nutrients (food) traverse the thoracic cavity via the esophagus, passing from the site of entry in the head to the site of digestion and absorption in the abdomen. 2. Thoracic Wall The true thoracic wall includes the thoracic cage and the muscles that extend between the ribs as well as the skin, subcutaneous tissue, muscles, and fascia covering its anterolateral aspect. The same structures covering its posterior aspect are considered to belong to the back. The mammary glands of the breasts lie within the subcutaneous tissue of the thoracic wall. The domed shape of the thoracic cage provides its components enabling to: Protect vital thoracic and abdominal organs (most air or fluid filled) from external forces. Resist the negative (sub-atmospheric) internal pressures generated by the elastic recoil of the lungs and inspiratory movements. Provide attachment for and support the weight of the upper limbs. Provide the anchoring attachment (origin) of many of the muscles that move and maintain the position of the upper limbs relative to the trunk, as well as provide the attachments for muscles of the abdomen, neck, back, and respiration. The thorax is one of the most dynamic regions of the body. With each breath, the muscles of the thoracic wall—working in concert with the diaphragm and muscles of the abdominal wall—vary the volume of the thoracic cavity, first by expanding the capacity of the cavity, thereby causing the lungs to expand and draw air in and then, due to lung elasticity and muscle relaxation, decreasing the volume of the cavity and causing them to expel air. 3. Skeleton of Thoracic Wall The thoracic skeleton forms the osteocartilaginous thoracic cage, which protects the thoracic viscera and some abdominal organs. The thoracic skeleton includes 12 pairs of ribs and associated costal cartilages, 12 thoracic vertebrae and the intervertebral (IV) discs interposed between them, and the sternum. The ribs and costal cartilages form the largest part of the thoracic cage; both are identified numerically, from the most superior (1st rib or costal cartilage) to the most inferior (12th). 3.1.Thoracic Vertebrae Characteristic features of thoracic vertebrae include: http://www.twitter/yeditepeanatomy 1 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Most thoracic vertebrae are typical in that they have bodies, vertebral arches, and seven processes for muscular and articular connections Bilateral costal facets (demifacets) on the vertebral bodies, usually occurring in inferior and superior pairs, for articulation with the heads of ribs. Atypical thoracic vertebrae are 1, 10 (sometimes), 11 and 12 have single facets. Costal facets on the transverse processes Spinous processes. Typically, two demifacets paired and the posterolateral margin of the IV disc between them form a single socket to receive the head of the rib of the same identifying number as the inferior vertebra (e.g., head of rib 6 with the superior costal facet of vertebra T6). 3.2. Ribs, Costal Cartilages, and Intercostal Spaces Ribs (L. costae) are curved, flat bones that form most of the thoracic cage. There are three types of ribs that can be classified as typical or atypical: True (vertebrocostal) ribs (1st-7th ribs): They attach directly to the sternum through their own costal cartilages. False (vertebrochondral) ribs (8th, 9th, and usually 10th ribs): Their cartilages are connected to the cartilage of the rib above them; thus their connection with the sternum is indirect. Floating (vertebral, free) ribs (11th, 12th, and sometimes 10th ribs): The rudimentary cartilages of these ribs do not connect even indirectly with the sternum; instead they end in the posterior abdominal musculature. Typical ribs (3rd-9th) have the following components: Head: wedge-shaped and has two facets, separated by the crest of the head; one facet for articulation with the numerically corresponding vertebra and one facet for the vertebra superior to it. Neck: connects the head of the rib with the body at the level of the tubercle. Tubercle: located at the junction of the neck and body; articulates with the corresponding transverse process of the vertebra, and a rough nonarticular part provides attachment for the costotransverse ligament. Body (shaft): thin, flat, and curved, most markedly at the costal angle where the rib turns anterolaterally. The angle also demarcates the lateral limit of attachment of the deep back muscles to the ribs. The concave internal surface of the body has a costal groove paralleling the inferior border of the rib, which provides some protection for the intercostal nerve and vessels. Atypical ribs 1st, 2nd, and 10th-12th ribs are dissimilar. Costal cartilages prolong the ribs anteriorly and contribute to the elasticity of the thoracic wall, providing a flexible attachment for their anterior ends. Intercostal spaces separate the ribs and their costal cartilages from one another. The spaces are named according to the rib forming the superior border of the space—for example, the 4th intercostal space lies between ribs 4 and 5. There are 11 intercostal spaces and 11 intercostal nerves. Intercostal spaces are occupied by intercostal muscles and membranes, and two sets (main and collateral) of intercostal blood vessels and nerves, identified by the same number assigned to the space. Sternum (Breastbone, Tr. iman tahtası) The sternum (G. sternon, chest) is the long, flat bone that forms the middle of the anterior part of the thoracic cage. It directly overlies and affords protection for mediastinal viscera in general and much of the heart in particular. The sternum is commonly known as the breastbone and is divided into three areas, the upper manubrium, the body, and the xiphoid process. The manubrium and body of the sternum lie in slightly different planes superior and inferior to their junction, the manubriosternal joint; hence, their junction forms a projecting sternal angle (of Louis). 4. Thoracic Apertures While the thoracic cage provides a complete wall peripherally, it is open superiorly and inferiorly. The much smaller superior opening is a passageway that allows communication with the neck and upper limbs. The larger inferior opening provides the ring-like origin of the diaphragm, which completely occludes the opening. Structures that pass between the thoracic cavity and the neck through the superior thoracic aperture: Trachea http://www.youtube.com/yeditepeanatomy 2 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Esophagus Nerves, and vessels that supply and drain the head, neck, and upper limbs Joints of Thoracic Wall Although the joints between the bones of the thorax has limited movement ability, the whole outcome of these movements permit expansion of the cavity during inspiration. During inspiration, the thoracic cavity can expand in antero-posterior, vertical and transverse dimensions. 1. Costa transverse joints 2. Sterno costal joint 3. Costachondralis joint 4. Intercondral Joints 5. Sternal Joints Muscles of Thoracic Wall Some muscles attached to and/or covering the thoracic cage are primarily involved in serving other regions. Several (axioappendicular) muscles extend from the thoracic cage (axial skeleton) to bones of the upper limb (appendicular skeleton). Muscles, such as sternocleidomasteoid muscle, abdominal muscles, pectoral muscles, function as accesory muscles of respiraton and work in forced respiration; when the person needs to breathe in and out more than usual; 100 meter sprinters, patients with respiratory problems. Muscles of the thoracic wall – Serratus posterior muscles – Levator costarum muscles – Intercostal muscles(External, internal and innermost) – Subcostal muscle – Transverse thoracic muscle These muscles either elevate or depress the ribs helping to increse the volume of the thoracic cavity. The diaphragm is a shared wall (actually floor/ceiling) separating the thorax and abdomen. Although it has functions related to both compartments of the trunk, its most important (vital) function is serving as the primary muscle of inspiration. 6. Vasculature of Thoracic Wall In general, the pattern of vascular distribution in the thoracic wall reflects the structure of the thoracic cage—that is, it runs in the intercostal spaces, parallel to the ribs. 7.1. Arteries of Thoracic Wall The arterial supply to the thoracic wall derives from the branches of the: Thoracic aorta Subclavian artery Axillary artery The intercostal arteries course through the thoracic wall between the ribs. 4.2. Veins of Thoracic Wall The intercostal veins accompany the intercostal arteries and nerves and lie most superior in the costal grooves. There are 11 posterior intercostal veins and one subcostal vein on each side. The posterior intercostal veins anastomose with the anterior intercostal veins (tributaries of internal thoracic veins). Most posterior intercostal veins (4-11) end in the azygos/hemiazygos venous system, which conveys venous blood to the superior vena cava (SVC). 5. Nerves of Thoracic Wall The 12 pairs of thoracic spinal nerves supply the thoracic wall. As soon as they leave the IV foramina in which they are formed, the mixed thoracic spinal nerves divide into anterior and posterior (primary) rami or branches. The anterior rami of nerves T1-T11 form the intercostal nerves that run along the extent of the intercostal spaces. The intercostal nerves pass to and then continue to course in or just inferior to the costal grooves, running inferior to the intercostal arteries (which, in turn, run inferior to the intercostal veins). The neurovascular bundles (and especially the vessels) are thus sheltered by the inferior margins of the overlying rib. 6.1. Dermatomes http://www.twitter/yeditepeanatomy 3 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Through its posterior ramus and the lateral and anterior cutaneous branches of its anterior ramus, most thoracic spinal nerves (T2-T12) supply a strip-like dermatome of the trunk extending from the posterior median line to the anterior median line. The skin area supplied by a segment of the spinal cord. 6.2. Atypical Intercostal nerves 1st intercostal nerve 2nd intercostal nerve 7th-11th intercostal nerve 12th intercostal nerve 7. Breasts The breasts are the most prominent superficial structures in the anterior thoracic wall, especially in women. The breasts (L. mammae) consist of glandular and supporting fibrous tissue embedded within a fatty matrix, together with blood vessels, lymphatics, and nerves. Both men and women have breasts; normally they are well developed only in women. The mammary glands are in the subcutaneous tissue overlying the pectoralis major and minor muscles. At the greatest prominence of the breast is the nipple, surrounded by a circular pigmented area of skin, the areola (L. small area). The mammary glands within the breasts are accessory to reproduction in women. They are rudimentary and functionless in men, consisting of only a few small ducts or epithelial cords. Usually, the fat present in the male breast is not different from that of subcutaneous tissue elsewhere, and the glandular system does not normally develop. 7.1. Female Breasts The amount of fat surrounding the glandular tissue determines the size of non-lactating breasts. The roughly circular body of the female breast rests on a bed that extends transversely from the lateral border of the sternum. The arterial supply of the breast: 1. Medial mammary branches 2. Lateral mammary branches, lateral thoracic and thoracoacromial arteries 3. Posterior intercostal arteries 2nd-4th The venous drainage of the breast is mainly to the axillary vein, but there is some drainage to the internal thoracic vein. The lymphatic drainage of the breast is important because of its role in the metastasis of cancer cells. Most lymph, especially from the lateral breast quadrants, drains to the axillary lymph nodes. Most of the remaining lymph, particularly from the medial breast quadrants, drains to the parasternal lymph nodes or to the opposite breast, whereas lymph from the inferior quadrants may pass deeply to abdominal lymph nodes. The nerves of the breast derive from anterior and lateral cutaneous branches of the 4th-6th intercostal nerves. MEDIASTINUM (Interpleaural space) The thoracic cavity is divided into three major spaces: the central compartment or mediastinum that houses the thoracic viscera except for the lungs and, on each side, the right and left pulmonary cavities housing the lungs. The mediastinum (Mod. L. middle septum, L, mediastinus, midway), occupied by the mass of tissue between the two pulmonary cavities, is the central compartment of the thoracic cavity. It is covered on each side by mediastinal pleura and contains all the thoracic viscera and structures except the lungs. Mediastinum extends from superior thoracic aperture superiorly to the diaphragm inferiorly and from sternum and costal cartilages anteriorly to to the bodies of the thoracic vertebrae posteriorly. The looseness of the connective tissue and the elasticity of the lungs and parietal pleura on each side of the mediastinum enable it to accommodate movement as well as volume and pressure changes in the thoracic cavity, for example, those resulting from movements of the diaphragm, thoracic wall, and tracheobronchial tree during respiration, contraction (beating) of the heart and pulsations of the great arteries, and passage of ingested substances through the esophagus. The mediastinum is divided into superior and inferior parts for purposes of description. • Superior mediastinum http://www.youtube.com/yeditepeanatomy 4 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy – Superior to sternal angle Inferior mediastinum: Inferior to sternal angle • Anterior mediastinum – Between the anterior surface of pericardium and posterior surface of the sternum • Middle mediastinum – Pericardium, heart and beginings of the great vessels emerging from the heart lie here • Posterior mediastinum – Lies posterior to the pericardium and diaphragm Some structures, such as the esophagus, pass vertically through the mediastinum and therefore lie in more than one mediastinal compartment. Contents of the superior mediastinum 1) Thymus 2) Great vessels related to the heart with the veins 3) Inferior continuation of the cervical viscera (trachea anteriorly and esophagus posteriorly) and related nerves (left recurrent laryngeal nerve) 4) Thoracic duct and lymphatic trunks 5) Prevertebral muscles Anterior mediastinum It lies between the sternum anteriorly and the pericardium posteriorly. Superiorly it continues with the superior mediastinum starting at the level of sternal angle. Contents of the anterior mediastinum Remnants of thymus Branches of the internal thoracic artery Posterior Mediastinum The posterior mediastinum (the posterior part of the inferior mediastinum) is located inferior to the sternal angle, posterior to the pericardium and diaphragm, and between the parietal pleura of the two lungs. Contents of the posterior mediastinum • Thoracic aorta • Thoracic duct • Posterior mediastinal lymph nodes • Azygos and hemiazygos veins • Esophagus • Esophageal nerve plexus • Thoracic sympathetic trunks • Thoracic splanchnic nerves HEART & PERICARDIUM . HEART The heart, slightly larger than a clenched fist, is a double, self-adjusting suction and pressure pump, the parts of which work in unison to propel blood to all parts of the body. The right side of the heart (right heart) receives poorly oxygenated (venous) blood from the body through the superior vena cava (SVC) and inferior vena cava (IVC) and pumps it through the pulmonary trunk and arteries to the lungs for oxygenation. The left side of the heart (left heart) receives well-oxygenated (arterial) blood from the lungs through the pulmonary veins and pumps it into the aorta for distribution to the body. The heart has four chambers: right and left atria and right and left ventricles. The atria are receiving chambers that pump blood into the ventricles (the discharging chambers). The synchronous pumping actions of the heart's two atrioventricular (AV) pumps (right and left chambers) constitute the cardiac cycle. The cycle begins with a period of ventricular elongation and filling (diastole) and ends with a period of ventricular shortening and emptying (systole). The wall of each heart chamber consists of three layers, from superficial to deep: Endocardium, a thin internal layer Myocardium, a thick, helical middle layer composed of cardiac muscle. http://www.twitter/yeditepeanatomy 5 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Epicardium, a thin external layer Externally, the atria are demarcated from the ventricles by the coronary sulcus (atrioventricular groove), and the right and left ventricles are demarcated from each other by anterior and posterior interventricular (IV) sulci (grooves). The heart appears trapezoidal from an anterior or posterior view, but in three dimensions it is shaped like a tipped-over pyramid with its apex (directed anteriorly and to the left), a base (opposite the apex, facing mostly posteriorly), and four sides. The four surfaces of the heart are the: Anterior (sternocostal) surface Diaphragmatic (inferior) surface Right pulmonary surface Left pulmonary surface Right atrium The right atrium forms the right border of the heart and receives venous blood from the SVC, IVC, and coronary sinus. The ear-like right auricle is a conical muscular pouch that projects from this chamber like an add-on room, increasing the capacity of the atrium as it overlaps the ascending aorta. The interior of the right atrium has a smooth, thin-walled, posterior part (the sinus venarum) on which the venae cavae (SVC and IVC) and coronary sinus open, bringing poorly oxygenated blood into the heart. The interatrial septum separating the atria has an oval, thumbprint-size depression, the oval fossa (L. fossa ovalis), which is a remnant of the oval foramen (L. foramen ovale) and its valve in the fetus. Right ventricle The right ventricle forms the largest part of the anterior surface of the heart, a small part of the diaphragmatic surface, and almost the entire inferior border of the heart. The right ventricle receives blood from the right atrium through the right AV (tricuspid) orifice. Tendinous cords (L. chordae tendineae) attach to the free edges and ventricular surfaces of cusps, much like the cords attaching to a parachute. The tendinous cords arise from the apices of papillary muscles, which are conical muscular projections with bases attached to the ventricular wall. Regurgitation of blood (backward flow of blood) from the right ventricle back into the right atrium is blocked during ventricular systole by the valve cusps. The interventricular septum (IVS), is obliquely placed partition between the right and left ventricles. Left Atrium The left atrium forms most of the base of the heart. The valveless pairs of right and left pulmonary veins enter the atrium. The tubular, muscular left auricle, its wall trabeculated with pectinate muscles, forms the superior part of the left border of the heart. A semilunar depression in the interatrial septum indicates the floor of the oval fossa; the surrounding ridge is the valve of the oval fossa (L. valvulae foramen ovale). The interior of the left atrium has: Pectinate muscles Four pulmonary veins (two superior and two inferior) An interatrial septum A left AV orifice through which the left atrium discharges the oxygenated blood it receives from the pulmonary veins into the left ventricle. Left Ventricle The left ventricle forms the apex of the heart, nearly all its left (pulmonary) surface and border, and most of the diaphragmatic surface. Because arterial pressure is much higher in the systemic than in the pulmonary circulation, the left ventricle performs more work than the right ventricle. The interior of the left ventricle has: A smooth-walled, non-muscular, superoanterior outflow part, the aortic vestibule, leading to the aortic orifice and aortic valve. A double-leaflet mitral valve that guards the left AV orifice. The mitral valve has two cusps. The semilunar aortic valve, between the left ventricle and the ascending aorta, is obliquely placed. Vasculature of the Heart The blood vessels of the heart comprise the coronary arteries and cardiac veins, which carry blood to and from most of the myocardium. http://www.youtube.com/yeditepeanatomy 6 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Arterial Supply of the Heart The coronary arteries, the first branches of the aorta, supply the myocardium and epicardium. The right and left coronary arteries arise from the corresponding aortic sinuses. Anastomoses between the branches of the coronary arteries exist, which enables the development of the collateral circulation. The coronary arteries supply both the atria and the ventricles. The right coronary artery (RCA) arises from the right aortic sinus of the ascending aorta and runs in the coronary sulcus. The left coronary artery (LCA) arises from the left aortic sinus of the ascending aorta, and runs in the coronary sulcus. Venous Drainage of the Heart The heart is drained mainly by veins that empty into the coronary sinus and partly by small veins that empty into the right atrium. Lymphatic Drainage of the Heart A single lymphatic vessel, formed by the union of various lymphatic vessels from the heart ends in the inferior tracheobronchial lymph nodes, usually on the right side. STIMULATING, CONDUCTING, AND REGULATING SYSTEMS OF HEART Stimulating and Conducting System of the Heart The conducting system consists of nodal tissue that initiates the heartbeat and coordinates contractions of the four heart chambers, and highly specialized conducting fibers for conducting them rapidly to the different areas of the heart. The impulses are then propagated by the cardiac striated muscle cells so that the chamber walls contract simultaneously. Impulse generation and conduction can be summarized as follows: The SA node (pacemaker of the heart; in the right atrium) initiates an impulse that is rapidly conducted to cardiac muscle fibers in the atria, causing them to contract. The impulse spreads by myogenic conduction, which rapidly transmits the impulse from the SA node to the AV node (in the right atrium). The signal is distributed from the AV node through the AV bundle and its branches (the right and left bundles), which pass on each side of the IVS to supply subendocardial branches to the papillary muscles and the walls of the ventricles. Innervation of the Heart Innervation of the heart is through the autonomic nerves (both sympathetic and parasympathetics) from the cardiac plexus. Septal Defects Atrial Septal Defects (ASD): A congenital anomaly of the interatrial septum, usually incomplete closure of the oval foramen, is an atrial septal defect (ASD). Ventricular Septal Defects (VSD): The membranous part of the IVS is the common site of ventricular septal defects (VSDs). VSDs rank first on all lists of cardiac defects. A VSD causes a left to right shunt of blood through the defect. Valvular Heart Disease Disorders involving the valves of the heart disturb the pumping efficiency of the heart. Valvular heart disease produces either stenosis (narrowing) or insufficiency. Stenosis is the failure of a valve to open fully, slowing blood flow from a chamber. Insufficiency or regurgitation, on the other hand, is failure of the valve to close completely, usually owing to nodule formation on (or scarring and contraction of) the cusps so that the edges do not meet or align. This allows a variable amount of blood (depending on the severity) to flow back into the chamber it was just ejected from. Both stenosis and insufficiency result in an increased workload for the heart. Because valvular diseases are mechanical problems, damaged or defective cardiac valves can be replaced surgically in a procedure called valvuloplasty. Coronary Artery Disease or Coronary Heart Disease: Coronary artery disease (CAD) is one of the leading causes of death. It has many causes, all of which result in a reduced blood supply to the vital myocardial tissue. Myocardial Infarction: With sudden occlusion of a major artery by an embolus (G. embolos, plug), the region of myocardium supplied by the occluded vessel becomes infarcted (rendered virtually bloodless) and http://www.twitter/yeditepeanatomy 7 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy undergoes necrosis (pathological tissue death). The most common cause of ischemic heart disease is coronary artery insufficiency resulting from atherosclerosis. Angina Pectoris: Pain that originates in the heart is called angina or angina pectoris (L. angina, strangling pain + L. pectoris, of the chest). Individuals with angina commonly describe the transient (15 sec to 15 min) but moderately severe constricting pain as tightness in the thorax, deep to the sternum. The pain is the result of ischemia of the myocardium that falls short of inducing the cellular necrosis that defines infarction. PERICARDIUM The pericardium is a fibroserous membrane that covers the heart and the beginning of its great vessels. The pericardium is a closed sac composed of two layers. The pericardium is a closed sac composed of two layers: 1) Fibrous pericardium (external) continuous with the central tendon of the diaphragm 2) Serous pericardium (internal) Parietal layer Visceral layer (epicardium) Visceral and parietal layers are continuous with each other where the great vessels enter and leave the heart. Inner surface is lined by the parietal layer of the serous pericardium and these layers are strictly attached to each other. The fibrous pericardium protects the heart against sudden overfilling because it is so unyielding and closely related to the great vessels that pierce it superiorly. The pericardial cavity is the potential space between opposing layers of the parietal and visceral layers of serous pericardium. It normally contains a thin film of fluid that enables the heart to move and beat in a frictionless environment. There are two potential spaces, i.e. sinuses in pericardium; transverse pericardial sinus and oblique pericardial sinus. The arterial supply of the pericardium is mainly from a slender branch of the internal thoracic artery. The venous drainage of the pericardium is from the pericardiacophrenic veins. The nerve supply of the pericardium is from the phrenic nerves). http://www.youtube.com/yeditepeanatomy 8