Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
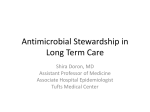
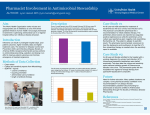
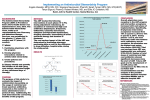
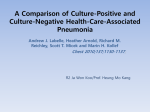
Presentation Number: 264 Category: A1. Infectious Diseases - Anti-infective Agents Retrospective Review And Analysis of the Clinical Impacts of an Antimicrobial Stewardship Program Katie Gordon PGY1 Pharmacy Resident Providence Alaska Medical Center Anchorage, Alaska Deemed exempt from IRB due to quality improvement project 1 Disclosure Statement Katie Gordon, Pharm.D. Potential Conflicts of interest: None Sponsorship: None Proprietary information or results of ongoing research may be subject to different interpretations. Presentation of this slide indicates my agreement to abide by the non-commercialism guidelines provided on the CE Requirements page. 2 Learning Objectives Describe the components of an antimicrobial stewardship program Explain the criteria for health care associated pneumonia versus community-acquired pneumonia Target audience: Pharmacists 3 Providence Alaska Medical Center Location: ◦ Anchorage, Alaska ◦ Population Estimate: 300,549 as of 2014 ◦ 1 of 3 hospitals in Anchorage ◦ Largest hospital in Alaska ◦ Highest level of acuity of care in Alaska Demographics: ◦ 394 bed, tertiary care, community hospital ◦ Level 2 Trauma Center ◦ Level 3 NICU ◦ Safety net hospital ◦ Decentralized pharmacy model 4 Background IDSA recommended components for Secondary Supplements to AMS AMS program includes: Programs ◦ Essential ◦ Infectious disease physician ◦ Clinical pharmacist with infectious disease training ◦ Optimal ◦ ◦ ◦ ◦ ◦ Clinical microbiologist Information system specialist Infection control professional Hospital epidemiologist Hospital administrative support Primary Core Strategies ◦ Prospective audit with intervention and feedback ◦ Formulary restriction and preauthorization ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ Education Guidelines and clinical pathways Antimicrobial cycling Antimicrobial order forms Combination therapy Streamlining or de-escalation of therapy Dose optimization Parenteral to oral conversion EMR, CPOE, and clinical decision support Computer based surveillance Clinical microbiology support Process measures 5 Background PAMC’s AMS program was initiated August 26, 2013 The objective of this study is to evaluate clinical outcomes of patients admitted with community-acquired pneumonia in relation to the start of an antimicrobial stewardship program in order to assess: • Inpatient mortality • 30-day readmission rate • Rate of C. difficile infection during admission • Length of stay • Duration of antimicrobial agents 6 Methodology Retrospective analysis Assessed for non-inferiority ◦ Year prior to AMS program initiation ◦ Year one post-AMS program initiation Inclusion: ◦ Primary ICD-9 code of 486.0 consistent with CAP ◦ August 26, 2012-August 26, 2014 7 Methodology Exclusion: ◦ Pregnant ◦ Incarcerated ◦ <18 years of age ◦ Admitted for <24 hours ◦ Concurrent infection requiring antibiotics ◦ LOS >60 days ◦ Met criteria for HCAP ◦ Immunocompromised ◦ Antibiotics in preceding 90 days ◦ Hospitalization of 5 days or more ◦ Chronic dialysis within 30 days ◦ Home infusion therapy ◦ Residence in extended care facility ◦ Hospitalization for ≥2 days in preceding 90 days 8 Methodology 1180 Patients (Excluding LOS <1 day, age <18 yo) Exclusion Criteria 790 Patients 390 Patients Included 9 Results Comorbidities 70.00% p 0.221 60.00% 50.00% p 0.734 40.00% p 0.440 p 0.360 30.00% p 0.784 p 0.229 20.00% p 0.375 10.00% 0.00% HTN COPD DM Year Prior Asthma HF A.fib Tobacco Year 1 of AMS 10 Results Clinical Outcomes 14% 12% 10% p 0.425 8% 6% p 0.571 p 0.425 4% p 1.0 2% 0% Inpt Mortality Readmit Readmit PNA/SOB Rate of C.diff acquisition Year Prior 4.05% 6.76% 2.70% 0.90% Year 1 2.98% 8.93% 4.17% 0.60% 11 Results Inpatient Mortality (% Yes) 12% 10% 8% 6% 4% 2% 0% Q3 2012 Q4 2012 Q1 2013 Q2 2013 Pre-AMS Post-AMS Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q3 2013 Q3 2013 12 Results Readmission within 30 days d/t PNA/SOB (% Yes) 7% 6% 5% 4% 3% 2% 1% 0% Q3 2012 Q4 2012 Q1 2013 Q2 2013 Pre-AMS Post-AMS Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q3 2013 Q3 2013 13 Results Clinical Outcomes 10 p 0.054 9 8 p 0.041 7 p 0.129 6 5 4 3 2 1 0 Mean Length of Stay Mean Days Inpt Abx Mean Days Total Abx Year Prior 6.95 5.57 9.48 Year 1 5.86 5.11 8.78 14 Results Length of Stay (Days) 10 9 8 7 6 5 4 Q3 2012 Q4 2012 Q1 2013 Q2 2013 Pre-AMS Post-AMS Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q3 2013 Q3 2013 15 Results Common CAP Antibiotics Total days of inpt abx 5.9 0.6 5.7 0.5 5.5 5.3 p 0.001 p <0.001 p <0.001 0.4 0.3 5.1 4.9 0.2 4.7 0.1 4.5 0 CTX Azith PreAMS LVQ PostAMS 16 Conclusions The antimicrobial stewardship (AMS) program at PAMC has not had negative impacts on clinical outcomes as related to communityacquired pneumonia Decrease in mean length of stay and duration of antimicrobials Fluoroquinolone usage has decreased Ceftriaxone and azithromycin usage has increased Future directions for continuation of this project include: ◦ Analysis after initiation of the community-acquired pneumonia clinical pathway ◦ Analysis of other commonly intervened upon disease states ◦ Integration of procalcitonin levels and rapid diagnostics (Biofire® Viral Panel) 17 References Dellit TH, Owens RC, McGowan JE, et al. Infectious disease society of America and the society for healthcare epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. CID. 2007;44:159-177. CDC. Vital signs: Improving antibiotic use among hospitalized patients. MMWR. March 2014;63(09):194-200. Ibrahim OM, Polk RE. Antimicrobial use metrics and benchmarking to improve stewardship outcomes. Infect Dis Clin N Am. 2014;28:195-214. Schmitt S, McQuillen DP, Nahass R, et al. Infectious disease specialty intervention is associated with decreased mortality and lower healthcare costs. CID. 2014;58(1):22-28. The Joint Commission: Specifications Manual for Joint Commission National Quality Core Measure (2010B). https://manual.jointcommission.org/releases/archive/TJC2010B1/Pneumon ia.html. Accessed August 10, 2014. 18