Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
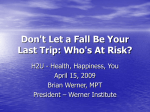
INBALANCE BALANCE SCALE PATIENT NAME: DOB: DATE: WITHIN THE LAST YEAR, HAVE YOU HAD ANY OF THE FOLLOWING: Section A 1. Do you have difficulty getting up from a chair or out of bed? Yes No Office Use Only 3 For instance, it takes more than one try to get up 2 3 4 5 6 7 8 9 10 4 Do you experience a numbness or loss of sensation in your legs? Do you have trouble walking up or down inclined surfaces (hills, ramps)? Do you ever lose your balance when standing still? Do you feel the need to look for support or grab on to something when you are moving around? Do you have problems judging distances when walking? For example, do you feel unsure about stepping off a curb? Do you use an assistive device (cane, walker) to walk around? Have you fallen more than once in the last year? Do you ever feel unsteady or lose your balance when walking? Do you currently take more than two (2) prescription medications? Section B 11 Do you feel dizzy or light-headed? 12 Have you ever suffered a stroke? 13 Have you ever suffered any type of head or neck trauma? 2 3 3 3 4 3 3 2 Yes No Office Use Only 6 780.4 4 434.90 4 716.18 6 368.10 For example, auto accident, sports injury, work-related injury 14 Do objects appear to bounce or jump around? Section C 15 If you experience dizziness, do you notice a spinning sensation when dizzy? 16 If you experience dizziness, do sudden changes in position (such as bending Yes No Office Use Only 3 386.10 4 17 18 down, tilting your head, quickly turning) make your symptoms worse? Have you noticed a decrease in hearing? Do you experience vision problems such as double vision or blurred vision? 2 389.9 3 19 Do you have an increased sensitivity to light and/or sound? 3 368.2 368.8 368.9 388.40 20 21 22 Do you experience dizziness when turning over in bed? Do you experience dizziness when watching a moving object? If you have dizziness, do you feel pain or pressure in your ears during an attack? Have you ever been knocked unconscious? Do you experience frequent headaches or migraines? Does looking up or down cause you to become dizzy? Do you experience a ringing, buzzing, or other sound in your ear(s)? 4 23 24 25 26 S:/FormsPDF/PatientForms/balance test questionaire 4 4 388.8 2 4 346.90 4 2 388.30 Revised 08/05/14