Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
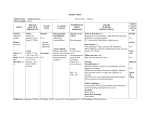
Anaphylaxis 13/5/11 FANZCA Notes = IgE mediated hypersensitivity reaction to an antigen -> profound histamine and serotonin release from basophil and mast cell degranulation. Clinically Within minutes of exposure - stings foods antibiotics contrast media thrombolytics NSAIDs sux & NDNMBD Flush or pallor Urticaria Angioedema Stridor Hypotension - cardiovascular collapse Bronchospasm Abdominal cramps Diarrhoea Coagulopathy Management Stop administering trigger Call for help Position supine (head down) O2 Exclude alternatives Pulse Adrenaline 0.5mg IM IV access Colloid or N/S (SBP >90mmHg) Promethazine 25-50mg IV Hydrocortisone 250mg IV Persistant hypotension/bronchospasm Jeremy Fernando (2011) Adrenaline 0.5mg IM No Pulse CPR Raise legs 2 large IV's 2 L IVF Increasing Adrenaline (adult - 1-4mg) (children - 10-100mcg/kg) H1 & H2 antagonists Extended CPR Persisting hypotension - Ranitidine (H2 antagonism) Adrenaline/Norad infusion Invasive monitoring Colloid Persistant bronchospasm - As per asthmatic emergencies Persisting angioedema - Nebulised adrenaline (1mg) ETT Cricothyroidotomy Tracheostomy Intra-operative Anaphylaxis Presentation Cardiovascuar collapse (most common) Erythema Bronchospasm Angio-oedema Rash Urticaria Most frequent culprits - muscle relaxants, antibiotics, NSAIDS Jeremy Fernando (2011) Management Stop trigger AB - FiO2 1.0 C - lay flat with legs elevated, adrenaline 50mcg IV increments, fluid Promethazine 25-50mg IV Hydrocortisone 100mg IV Adrenaline infusion 0.05-0.1mcg/kg/min Acidosis - 50mL of 8.4% NaHCO3 Check for cuff leak before extubation Bronchodilators as above Anaphylaxis Follow Up 4/3/09 OHOA pages 954-956 Incidence - 1:6,500 Differential - anaphylactoid reaction (histamine or complement activation) drug induced reaction related to genetic status (angio-oedema) machine or operator error asthma systemic mastocytosis malignant hyperthermia vasovagal episode Main Cuprits - NMBD (70%) - antibiotics Clinical presentation - rapid after an IV bolus slower if other route cardiovascular collapse (80%) cutaneous signs (50%) bronchospasm (36%) angio-oedema (24%) Investigations SERUM TRYPTASE - released from secretory vesicles of mast cells take @ 1, 6 and 24 hours serum separated and stored @ 20 C normal - <1ng/mL Jeremy Fernando (2011) - non-specific and anaphylactoid reactions - 1-15ng/mL - true anaphylaxis - levels higher than this RAST TESTING - radioallergosorbent test for antigen-specific IgE antibodies CAP TESTING - an antigen coated capsule is exposed to the patients serum under laboratory conditions if serum contains antigen specific IgE a measurable colour change is produced superceeded RAST testing available for testing pencillin, sux and latex allergy sensitivity low -> thus negative result requires skin testing SKIN or INTRADERMAL TESTING - skin testing has been shown to be diagnostic for anaphylaxis (but not for anaphylactoid reactions) - should take place 4-6 weeks post event to allow regeneration of IgE - antihistamines should not have been given within the last 5 days - use skin prick testing first - test all drugs given before the event - use a saline as a negative control - use histamine solution as a positive control - weal >2mm wider than saline = positive - repeat positive test with a 1:10 dilution to reduce the chance of a false positive - once positive drug detected -> test other drugs in same class - if history is strong, but skin prick test negative -> test intradermally with diluted drugs Management - communicate importance of finding to patient letter medic alert bracelet mark hospital notes inform GP report reaction to Med Safe - avoid all untested and related drugs - do not use an IV test dose - if unsure about IV induction agents -> gas induction - if NMBD reaction -> use a relaxant free anaesthetic, if must be used by guided by skin prick test result, give chlorphenamine (10mg) and hydrocortisone (100mg) IV pre-induction Jeremy Fernando (2011)