Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
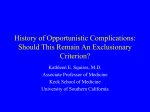
1 28 June, 2011 MULTICENTER STUDY ON THE BURDEN OF ILLNESS OF ORAL SIDE EFFECTS FROM CONDITIONING THERAPY BEFORE CONDITIONING THERAPY (CHEMOAND RADIOTHERAPY) BEFORE STEM CELL TRANSPLANTATION IN PATIENTS DIAGNOSED WITH HEMATOLOGIC DISEASES - ORA-STEM STUDY Numerous oral complications have been associated with cancer therapies. In order to establish recommendations for pre-, interim-, and post-cancer therapy management of oral problems in patients with hematological malignancies receiving high dose conditioning regimen and stem cell transplantation (autologous or allogeneic), an understanding of the scope of oral complications from cancer therapy must be established and be related to time after treatment and treatment regimen. The lack of clarity in this field is reflected in a lack of comprehensive and effective oral management regimens in the clinical arena. With a deeper understanding of oral complications, oral care regimens to minimize such complications can be appropriately formulated and evaluated. There is thus a pressing need to establish the nature, incidence and temporal relationship of oral complications related to conditioning therapies, as well as other types of cancer therapies. The literature reports a wide range of oral complications with varying incidences. Mucositis, or inflammation of the mucosal surfaces, sometimes also called mucosal barrier injury (MBI), is a major dose-limiting side effect of cancer therapy. Severe mucositis has been associated with pain, infection, poor nutrition, increased hospitalization and a major impact on quality of life and economic outcomes. Other reported complications are bleeding, dysphagia (difficulty swallowing), dysgeusia (altered sensation of taste), infection (bacterial, viral, and fungal), pain, trismus, osteonecrosis, osteoradionecrosis, xerostomia/salivary gland dysfunction, caries, periodontal disease, dental growth and developmental disturbances in children and graft-versus-host-disease (GVHD).(1) Recent systematic reviews of these oral complications have confirmed the limitations in knowledge of the incidence and severity of the various additive oral complications. Furthermore, how these common oral complications further complicate clinical and economic outcomes and affect quality of life (QoL) is poorly understood. 1 2 Overall aim The overall aim of the current prospective international observational multicenter study in stem cell transplant patients is to establish the nature, incidence and temporal relationship of oral complications related to conditioning regimen (chemotherapy with or without total body irradiation-TBI), stem cell transplantation and immunologic reactions (mainly GVHD) and to determine what objective and subjective oral complications related to treatment can predict negative clinical and economic outcomes and reduced QoL. Specific Aims To address the gaps in the knowledge of oral complications associated with hematological malignancies receiving high dose conditioning regimen and stem cell transplantation (autologous or allogeneic) the following specific aims will be evaluated. Primary aim 1. What is the incidence, severity and temporal relationship of oral complications related to type of conditioning regimen and how do they develop: 1.1. subjective oral complications 1.1.1. oral pain 1.1.2. xerostomia (dry mouth) 1.1.3. dysgeusia (taste changes) 1.1.4. dysphagia (swallowing difficulties) 1.2. objective oral complications 1.2.1. oral mucositis 1.2.2. oral infections (viral, fungal, bacterial) 1.2.3. submucosal hemorrhage 1.2.4. dental and periodontal diseases and complications 1.2.5. osteonecrosis 1.2.6. GVHD 1.2.7. hyposalivation 2 3 Secondary aims 2. Are there signs to predict oral complications. 2.1. Are there early clinical signs which can be used to predict mucositis and GVHD? 2.2. Does genetic polymorphisms in candidate genes demonstrate an increased risk for the development of severe mucositis and GVHD? 3. How are oral complications related to other confounding variables. 3.1. Demographics (age, sex, race) 3.2. Cancer diagnosis 3.3. Cancer therapy 3.4. Autologous or allogeneic stem cell transplantation 3.5. Antimicrobial prophylaxis or Keratinocyte Growth Factor (KGF) medication 3.6. Ongoing immunosuppression for GVHD 3.7. Recommendations for local special oral care program 3.8. Non-oral signs/symptoms 3.8.1. Nausea/Vomiting 3.8.2. Diarrhea 3.8.3. Fever 3.8.4. Weight 3.8.5. Blood values 4. How do subjective and objective oral complications related to treatment, impact on poor general clinical and economic outcomes. 4.1. Are oral complications identified as a cause of additional hospital visits, prolonged hospital stays or death? 4.2. Can oral complications/infections be related to systemic infection? 4.3. Are oral complications identified as a cause for increased medication/treatment (e.g. antibiotics, morphine)? 4.4. Are oral complications (e.g. xerostomia, taste etc.) possible to relate to poor nutrition/parental nutrition? 5. How is patients’ QoL affected by treatment-related oral complications in the short and long time, specifically 3 4 5.1. subjective oral complications: 5.1.1. oral pain 5.1.2. xerostomia (dry mouth) 5.1.3. dysgeusia (taste changes) 5.1.4. dysphagia (swallowing difficulties). Patient Population Inclusion criteria Patients receiving conditioning regimen (full intensity conditioning, FIC, or reduced intensity conditioning, RIC), followed by stem cell transplantation (autologous or allogeneic) in adults from Gothenburg Sweden, Stockholm Sweden and additional centers. Diagnoses: acute leukemia myelodysplastic syndrome (MDS) aplastic anemia lymphoma including chronic lymphoid leukemia chronic myeloid leukemia myelofibrosis multiple myeloma lymphoma including chronic lymphoid leukemia testis cancer others, such as autoimmune diseases (scleroderma; systemic sclerosis) Exclusion criteria Patients unable to give consent. Children younger than 18 years. 4 5 Publication strategy The Publications Committee (Drs I. v. Bültzingslöwen, M. Brennan, M. Jontell and J-E. Johansson) will decide on publications originated from the Ora-Stem Study. Authors of publication may be I. Project organizers Mike Brennan North Carolina USA, Inger v. Bültzingslöwen, Mats Jontell Gothenburg, Sweden II. Hematologist Jan-Erik Johansson Gothenburg Sweden III. Principal investigator (PI) from each participating centers, i. Karin Garming-Legert, Karolinska Institute, Stockholm Sweden ii. Bengt Hasseus, Peter Johansson, Sahlgrenska Academy, Gothenburg Sweden iii. PI from additional participating centers (to be decided later) Background and Significance The annual incidence of cancer is 11 million cases worldwide.(2) Earlier cancer detection and advances in cancer therapies have provided important management advances to improve survival and quality of life. Common cancer treatment strategies include surgical resection, chemotherapy (CT), radiotherapy (RT), and hematopoietic stem cell transplantations (HSCT). The goal of such treatments is to eliminate all cancer cells. However, side effects from these therapies can limit the effectiveness of treatment and have a marked impact on the patient’s QoL. The oral cavity is a common site of complications related to cancer therapies. The Surgeon General’s report on Oral Health in America estimates that more than 400,000 patients in the U.S. undergoing cancer treatment will develop oral complications annually.(3) To fully understand which oral complications from cancer therapies are important targets for prevention and better management, it is important to understand the burden of illness from cancer and from cancer therapies. Numerous studies have identified, and report a wide range of incidence and severity for different oral complications from cancer therapies. In 1989, the National Institutes of Health Development Consensus Conference on the Oral Complications of Cancer Therapies provided recommendations for oral assessment and oral/dental management prior, during and following cancer therapy.(4) 5 6 These recommendations served to summarize our understanding of the subject at the time. Since the Consensus Conference, there has been a gradual increase in interest in these problems. During this time, there was a movement towards developing preventive and management strategies. The conference brought together leading experts in the field and clearly catalyzed and legitimized the development of a formal specialty discipline of oral oncology. Documentation of the burden of illness has been more successful regarding some oral complications than others. Mucositis, or inflammation of the oral and gastrointestinal mucous membranes, is a painful and dose-limiting side effect of CT and RT. Severe mucositis can: result in delay in the delivery of cancer therapy and/or dose reduction of cancer therapy; prolong hospitalization; require IV narcotics for pain control; and interfere with or prevent oral nutrition, limit oral hygiene and speaking for prolonged periods of time, and increase the risk of systemic infection.(5) The Mucositis Study Section of the Multinational Association of Supportive Care in Cancer (MASCC) and the International Society of Oral Oncology (ISOO) held two Consensus Conferences regarding the impact and treatment of cancer-related oral mucositis. Participants reviewed the available literature on mucositis for quality, and devised recommendations based on the strength of the literature. The main areas of review included the epidemiology of mucositis by cancer regimen, pathophysiology, and clinical research of treatment regimens. Two manuscripts presented the findings of the first consensus conference.(5;6) In 2005, an update of the mucositis literature was completed to include the same areas of review. Over 3000 articles were reviewed for the three year period of the 2005 consensus conference. Compared to the initial review from 1966 to 2001, this amount of articles in a short time period, represents a sharp increase in the interest of research in the field of mucositis, with recent therapies becoming available which appear to have a significant impact in the moderation of this common oral complication.(7) The clinical and economic impact of oral and gastrointestinal mucositis has been shown to exceed $40,000 for HSCT patients who develop oral ulcerations.(8) Increased costs were related to additional days of hospitalization, total parenteral nutrition, and intravenous narcotic therapy. In a retrospective analysis of the economic burden from chemotherapy-induced mucositis in patients treated for solid tumors, the presence of grade 3 or 4 alimentary mucositis resulted in an incremental cost of $3500 per chemotherapy cycle.(9) Limited data on the economic impact from non-mucositis oral complications is available. An economic analysis of amifostine compared to placebo in patients with 6 7 advanced head and neck cancer, demonstrated improvement in xerostomia and mucositis in the amifostine group. Supportive care costs from management of oral complications from radiation therapy were $4,401 for the amifostine group and $5,873 for the control group.(10) In patients who experience more severe oral mucositis (i.e. WHO grade 3-4), approximately 35% will have a delay in chemotherapy, 60% will have a reduced dose of chemotherapy, and 30% will have the regimen discontinued.(5) Additionally, the development of severe mucositis will necessitate a feeding tube to maintain nutrition in 70% of patients, result in fever in 60% of patients, and necessitate hospitalization in 62% of patients.(5) Additionally, at a WHO grade 3 or 4 mucositis, 70% of patients receiving standard dose chemotherapy, and 87% receiving high-dose chemotherapy with a stem cell transplant (SCT), will require feeding tubes to maintain adequate nutrition.(5) Mucositis associated with autologous bone marrow transplants can extend a hospital stay by 6 days with a cost estimated at $27,000 per patient.(11) In another study, human stem cell transplant recipients with oral ulceration had increased costs of $42,749 per patient.(8) Risk factors for the development of mucositis have been identified and include low body mass and certain chemotherapeutic agents (e.g. paclitaxel, doxorubicin, etoposide, 5fluorouracil, and irinotecan).(5;12) Increased risk from specific chemotherapeutic agents is likely the result of direct cytotoxic effects from these agents. Other proposed factors include diagnosis of acute myelogenous leukemia, acute lymphocytic leukemia, or myelodysplastic syndrome; prolonged neutrophil recovery; young age; and conditioning regimen for bone marrow transplantation.(13) However, the pathogenesis of mucositis is poorly understood,(14) and it is unclear why patients of the same age, with the same malignancy and chemotherapy regimens develop mucositis with different frequency and severity. Mucositis demonstrates a wide variety of histologic changes ranging from degeneration of collagen to epithelial hypoplasia (15) the variability of which is likely due to the biologic complexity of mucositis. Recent evidence indicates that genetic predisposition has a role in RT and CT associated alimentary mucositis.(16;17) Differences in radiation-associated ulceration have been demonstrated in dissimilar mouse strains. In this investigation of two different animal models of radiation-associated mucositis, the observed mucosal ulceration was dependent on mouse strain, and not dependent on radiation dosage.(16) In another study, individual genetic differences accounted for variations in CT associated mucositis from a specific CT regimen. Patients undergoing bone marrow transplantation who demonstrated certain 7 8 genetic polymorphisms of a folate-metabolizing enzyme had more severe mucosal toxicity from methotrexate.(17) The identification of gene products consistently over- or underexpressed might identify therapeutic targets for interventions that would decrease the incidence and duration of cancer treatment-related mucositis. Identifying genetic polymorphisms in such patients could be used to screen for mucositis-prone patients. Microarray analysis of oral mucosa tissue samples before and following chemotherapy will allow us to identify candidate genes which may be important in the pathophysiology of mucositis or as predictors of the development of chemotherapy-associated mucositis. Such genes may form the basis for future screening tests to predict the likelihood of mucositis following treatment with specific CT protocols and identify patients who would benefit from targeted preventative therapy. Numerous preventive care protocols have been proposed to minimize oral complications from cancer therapies. Unfortunately, these protocols are rarely evidencebased and often rely on “expert opinion” or anecdotes. The lack of well-controlled, prospective studies is the primary reason for the limitation in preventive and management protocols. The Institute of Medicine (IOM) report determined that insufficient systematic research is available to assess the prevention and management of the oral problems associated with head and neck cancer, leukemia, and lymphoma. The Surgeon General’s report Oral Health in America calls for both the building of the science and evidence base, and the application of science effectively to improve oral health. This recommendation development process aims to effectively transfer research findings in the field of oncology, including oral complications seen with cancer therapies, and oral management prior to the start of cancer therapy, to the public and health professionals. Well developed, evidence–based management recommendations have the potential to enhance the appropriateness of clinical practice, improve the quality of oral health care, lead to better patient outcomes, improve cost-effectiveness, and identify areas of further research needs. In order to effectively change perceptions of the burden of illness of oral complications from cancer therapies, a complete understanding of the impact of these complications is vital. Concern for underestimating the impact of oral complications may result in avoidance or delay in appropriate care for cancer patients. Considering our limited understanding of the burden of illness in the oral cavity from various cancer therapies, it is difficult to produce evidence-based, preventive and management protocols. Therefore, a prospective multi-center study is necessary to collect data on the burden of illness from various cancer regimens. 8 9 Preliminary Pilot Studies Registration of oral complications using MedView software program The search for new knowledge in oral medicine should be facilitated by prospective use of formalized information gathered in multicenter studies. The Institute of Odontology, Göteborg University, and Department of Computing Science, Chalmers University of Technology, have developed MedView, a prototype for the collection and analysis of large amounts of clinical data. MedView is a computer program that is based on formalized input and registration of all clinical information. MedView provides a suite of tools for formalizing, gathering, and analyzing data. The output applications are focused on visualization and statistical analysis. MedView is aimed at clinical research and is well suited for multicenter studies.(18) MedView program is accessible on the Internet. Each participating center/dentist needs a unique pass word. All clinical information is entered using electronic protocols, where case history and data from the clinical examinations are defined by formalized parameters. The patients can be registered and identified with a code, which is known only to the treating surgeon. The reason is to permit transfer of information within the network without compromising the identity of the patient, and the procedure has been approved by the Swedish Data Inspection Board. During the clinical interview and examination, the operator enters the correct parameter, which is then inserted adjacent to the corresponding question. Clinical information regarding results from biopsies, laboratory tests and other invasive or noninvasive investigations are included, as are diagnoses, treatment modalities and clinical outcomes of performed therapies. The protocols are flexible and can be changed by the user to meet new or altered demands. This is accomplished by MedRecords Creator. These applications enable the addition of new values or parameters on a continuous basis. They can also be used to create entirely new protocols for specific topics or scientific evaluations. The protocols can therefore be created in any language. MedRecords contains a function, which permits the user to simultaneously observe a summary of registered information develop, as values are inserted in the protocol. When the examination is completed, the obtained summary can be copied and pasted into a document or template and printed out. The clinical appearances of mucosal lesions are registered with digital 9 10 images. All images in the entire database are saved in a single picture file. The images are given an identity by the program, and no renaming procedures are required. By a “clickand-drag” procedure, an attachment is made between the individual image and the input protocol. Technically, all images should be taken with 3 CCD cameras in order to ensure a high quality of colour balance. Images from other sources may be included. If the pathologist provides digital images from the histopathological examination, these images can also be attached to the MedRecords file, and the same is possible for x-ray images. Medview generates a database based on formalized and harmonized criteria, where information can be retrieved, visualized and analyzed. The database is placed at the Oral Medicine Department, Institute of Odontology, Sahlgrenska Academy, Göteborg University, Sweden.(19) The Oral Medicine Department, Public Dental Health and Sahlgrenska Academy in Göteborg, has documented oral complications in MedView after peripheral stem cell transplantation (PSCT) for 246 patients from 2005 to 2008 in a pilot study. The aim was to test if the MedView system can be used for this patient group. Oral mucositis, oral pain, eating/drinking problems and taste changes retrieved from this pilot study are reported here. Oral mucositis was documented by the World Health Organization (WHO) mucositis grading scale. The prevalence of grade III or IV mucositis was 65 percent (153 of 236 patients) during the PSCT period. The level of oral pain was registered on a visual analogue scale (VAS). The WHO score correlated well with the self-reported VAS score (Table 1). It can be noted that even when the objective clinical signs of mucositis were mild to moderate (grade I-II), the subjective problems were still considerable for some patients. The maximum WHO score was registered at day +8 after transplantation. Difficulty eating solid foods at one or more occasions during the transplant therapy was registered on a four grade scale. Out of the 246 patients, 159 reported difficulties. The inability to ingest solid foods was most common between days 4 through 13 after treatment. As much as 90 of 246 patients reported inability to drink or ingest liquid foods at some point during the transplant period; the highest concentration of reports being around day 8 after transplantation. Registrations regarding taste changes were made at four, and sometimes eight, months post-transplant check-up in 96 patients. No registration of grade of severity or time of onset was made. Out of the 96 patients, 37 experienced taste changes after transplantation. Of these, 16 had recovered at the time of questioning. 10 11 In conclusion, this pilot study shows that the MedView system can be used in this patient group. The clinical issues that were included seemed relevant; however validated scales should be used whenever possible and further issues be included. It should be pointed out, that the way data was reported changed during the years, leaving room for error. This was probably most obvious regarding why the patients were unable to ingest solid or liquid foods. Our clinical experience is that the most common cause for this is dysgeusia (do not want to eat) or discomfort from the throat or gut instead of oral mucositis. The instrument (MedView) should be calibrated by all participants in a multicenter study to reduce the risk of these kinds of errors. Table 1. The table shows how patients with different grades of oral mucositis, according to the WHO Mucositis grading scale, graded their level of pain on a VAS scale 1-10. Patients Proportion of patients, Proportion of patients, for with WHO for each WHO grade, each WHO grade, who mucositis who graded their level of graded their level of pain as scale, grade pain as being ≥ 5.0 on being ≥ 8.0 on VAS I-IV VAS 22% 3% I 35% 8% II 75% 23% III 87% 54% IV Review of oral complications associated with cancer therapies To determine the most common oral complications associated with cancer therapies reported in the literature, members of the Oral Care Study Section of MASCC/ISOO under the leadership of one of the project organizers - completed a literature search and data collection (Table 2). These preliminary results were presented at a planning meeting of the Oral Care Study Section prior to the annual MASCC/ISOO meeting in Geneva, Switzerland in June, 2005. Two separate searches were completed for RT and CT. The search strategy was adapted from “highly sensitive search strategies for identifying reports of randomized controlled trials in MEDLINE” in the Cochrane Reviewer’s Handbook.(20) Searches were completed with MEDLINE, Cochrane, and ACP Journal Club (Best Evidence) citations. A total of 528 articles were identified by the search strategy. Abstracts were reviewed and articles were chosen based on the presence of original data on oral complications related to a cancer therapy. Narrative reviews were excluded, while systematic reviews were accepted for review. A well-done systematic review has recently been completed for mucositis by 11 12 the Mucositis Study Section of MASCC/ISOO,(5;6) therefore, this oral complication was not included in the search strategy, and articles that reported only mucositis were excluded for further review by evaluators. A total of 176 articles that reported oral complications were selected for review by nine oral health experts. Of these 176 articles, 48 evaluated oral complications associated with CT, while 128 evaluated complications of RT with or without CT. Only 13% of these articles were randomized controlled trials, and 73% of all studies were prospective. The five most commonly reported oral complications in order of incidence included xerostomia, dysphagia, fungal infection, osteoradionecrosis, and dysgeusia (Table 2). A wide incidence range was apparent for all oral complications. Table 2: Oral complications (except mucositis) incidence (of any grade) for all cancer therapies. Oral Complication # Studies Mean (%) Incidence Range (%) Xerostomia 67 63.4 7.7 – 100 Dysphagia 25 54.1 5 – 100 12 41.9 9.5 – 100 Hemorrhages 5 32.1 4 – 72 Fungal Infection 21 26.8 3 – 91.7 Viral Infection 4 23.2 9.9 – 35.7 Oral Pain 7 18.3 7 – 55 (difficulties swallowing) Dysgeusia (taste disturbances) The results of the preliminary review provide important baseline data to understand the scope of oral complications from cancer therapy literature. These findings are vital in the planning of a prospective study to identify the burden of illness of oral complications from cancer therapies. Furthermore, bacterial infections, mucositis, osteonecrosis and GVHD may also cause considerable harm and are of interest to evaluate in the prospective study. The preliminary review has been followed by systematic reviews of the current scientific literature on oral side effects from cancer treatment.(21-32) 12 13 Analysis of gene expression to elucidate genetic predisposition for mucositis Preliminary research studies conducted by the Department of Oral Medicine at Carolinas Medical Center have successfully identified gene changes in the oral mucosa resulting from chemotherapy in patients with acute myeloid leukemia (AML). Microarray analysis was completed for a total of 11 tissue samples from patients and control subjects with RNA isolated from the buccal mucosal biopsies and gene expression analysis with Affymetrix Human Genome U133 Plus 2.0 microarray. In addition to pre- (n=4) and postchemotherapy (n=4) buccal mucosa tissue collected from patients with AML, buccal mucosa samples were collected from three healthy controls (n=3). Comparisons included the following: pre-chemotherapy AML (PreC) vs. healthy control (HC); post-chemotherapy AML (PostC) vs. HC; and PreC vs. PostC. Sufficient RNA was obtained in all 11 samples processed in the preliminary analysis. Thirty-two genes were identified to be differentially expressed. These genes might be involved in the onset and / or control of chemotherapyinduced mucositis as well. These preliminary results suggest that chemotherapy has a significant effect on differential gene expression in oral tissues from AML patients. 13 14 Experimental Design Methodology Patients who meet the enrolment criteria will be approached and consent will be reviewed and obtained. The MedView computer software will be used for registration of data. Each patient is coded with a letter depending on treating center (A=Gothenburg, B=Stockholm, C=XXX, and so on) and a number (e.g. A/053). A pre-treatment assessment (Phase I) will be completed to include the following: medical conditions, current cancer diagnosis, planned cancer regimen, medications, allergies, social history, patient report of oral problems, dental history, subjective oral complaints, objective measures of oral disease, current laboratory values, dental treatment recommended and untreated dental disease. This pre-treatment assessment will occur 1 week to 8 weeks prior to stem cell transplantation. Before or upon admission to the hospital for conditioning for stem cell transplantation, an assessment (Phase II) of medical condition, medications, subjective and objective oral findings, quality of life measures and laboratory values will be completed. The admission evaluation will occur at day -7 to -1 days. A similar bedside assessment (Phase III) as the admission evaluation will be completed 3 days/week (Monday, Wednesday and Friday) starting day 0, +1, +2 or +3 (depending on day of the week for transplantation) until resolution of neutropenia (i.e. absolute granulocyte count > 0.5 x 109). For patients with continued mucositis or other oral problems requiring hospitalization after resolution of neutropenia, an oral examination will be completed for up to 6 weeks duration after transplant. Additional visits for urgent care for acute oral problems will be documented regarding the nature of the oral problem and treatment provided (Phase IV). This will be documented for up to 6 months for the autologous stem cell transplantation patients and 12 months for the allogeneic transplant patients. Patients will be followed-up (Phase V) in an outpatient setting at 100 days for those treated with an autologous stem cell transplantation. These patients will also receive a questionnaire at 1 year post-transplantation to identify any long-term side effects, thereafter yearly until resolution of side effects. Those treated with allogeneic transplantation will be followed up at 100 days, 6, 9 and 12 months. Thereafter, yearly follow-ups will be performed until resolution of side-effects. The 14 15 assessment will include cancer response to therapy, current medical conditions, medications, subjective and objective oral findings, QoL measures and laboratory values. Study outline of the standardized examination process, see Fig 1. The different Phases correspond to the different sections in the MedView computer software program form. Of the variables that will be measured, the following need detailed description. GVHD GVHD may occur in allogeneic stem cell transplant patients. Graft lymphocytes react on patient antigens. Acute GVHD (aGVHD) occurs within 100 days after transplantation. aGVHD is graded as none (0), mild (I), moderate (II), severe (III) and life threatening (IV) and involves skin, liver and/or GI tract. Symptoms of GVHD 100 days or more post-transplant are diagnosed as chronic GVHD (cGVHD), whether proceeded by aGVHD or not. cGVHD may be limited (skin and/or liver engagement) or extensive (involves skin, nails, hair, mouth, eyes, genitals, liver, lungs, GI-tract, fascia, muscles, skeleton/joints, serous organs, blood, immune system). Oral symptoms are by definition signs of cGVHD, although there are reports on early clinical oral symptoms. This may be of interest to evaluate. Oral signs of GVHD are oral dryness, burning sensation, gingival reactions, mucositis, erythema, lichen, etc. Periodontology measures At Phase II, clinical oral assessment of the percentage of teeth with plaque and supragingival calculus should be documented whilst other periodontal parameters, such as subgingival calculus, bleeding on probing and periodontal pockets can be captured earlier, for example in phase I. If periodontal treatment was done after these measured, it should be documented. Oral hygiene, measured at Phase II Baseline oral hygiene will be measured by the number of teeth with plaque present. Plaque visible with the eye (yes/no) will be registered for each tooth: <20% of teeth with plaque will be graded as good oral hygiene 20-50% is intermediate and >50% of teeth with plaque is considered poor oral hygiene. 15 16 Calculus Calculus is essential to measure since it will facilitate accumulation of plaque. It will be measured as Supragingival calculus measured in Phase II <20% of teeth with calculus 20-50% of teeth with calculus >50% of teeth with calculus Subgingival calculus measured in Phase I <20% of teeth with calculus 20-50% of teeth with calculus >50% of teeth with calculus Pocket depth, measured in Phase I and in Phase II ( if possible) Full pocket depth index will be registered on four surfaces on each tooth at the dental clinic: 1-3 mm (shallow pockets), 4-6 mm (medium deep pockets), >6 mm (deep pockets): <20% of teeth with a least one deep pockets, moderate severity 20-50% of teeth with deep pockets, intermediate severity >50% of teeth with deep pockets, high severity Bleeding on Probing (BoP), measured in Phase I and in Phase II (if possible) Bleeding will be noted (Y/N) with each tooth. The percentage of teeth with the presence of BoP <20% of teeth with BoP 20-50% of teeth with BoP >50% of teeth with BoP Saliva samples to measure salivation The amount of unstimulated whole saliva will be measured by collecting saliva for 5 min. The amount of stimulated whole saliva will be measured during 5 min of chewing paraffin. To be collected at Phase I and at Phase V/+100 days in both autologous and allogeneic transplant patients, in allogeneic transplant patients also at Phase V/1 year. Xerostomia (subjective feeling of dry mouth) is evaluated in all Phases. A question about xerostomia is also to be included in the 1 year-questionnaire to autologous transplant patient. 16 17 Saliva samples for polymorphism study We will obtain saliva DNA samples from cancer patients prior to a conditioning regimen of chemotherapy for autologous or allogeneic stem cell transplantation. These patients will be followed prospectively to document the incidence and severity of mucositis. We will evaluate if genetic polymorphisms in the candidate genes identified in mucositis studies completed by the Department of Oral Medicine, Carolinas Medical Center will demonstrate an increased risk for the development of severe mucositis (WHO grade 3 or 4). A saliva sample will be obtained prior to the start of cancer therapy and sent to Carolinas Medical Center for storage. Saliva for polymorphism study should be taken after the samples to measure salivation. To keep collection of DNA as simple as possible, we will use the Oragene DNA™ system (DNA Genotek Inc.,Ottawa, Ontario, Canada). All that this requires is for the patients to rinse their mouth with water to clear any food debris before spiting 2 ml of saliva into the Oragene™ container. Once the container is closed, the contained reagents release the DNA from buccal epithelial cells in the saliva and stabilize it for long term storage. Samples can be kept at room temperature for several years without deterioration. The container is designed, approved, and comes with packaging for mailing. The median yield from a 2 ml saliva sample is 110 µg of DNA. This is higher than for most other oral epithelial cell sampling systems and more than adequate for future genetic epidemiological studies. Following collection, the sample could be stored locally at room temperature before mailing to the Carolinas Medical Center for storage at -20ºC before further processing and analysis. Approximately 15 candidate genes identified in previous mucositis studies completed by the Department of Oral Medicine at Carolinas Medical Center will be evaluated for polymorphisms that increase the risk for the development of severe oral mucositis. The flow of the study will include the following: 1. Identify candidate genes based on results of prior studies from the Department of Oral Medicine at Carolinas Medical Center 2. Compile single nucleotide polymorphisms (SNPs) within candidate genes. 3. Select SNP panel. The idea is to use the fewest number of SNPs that are feasible. Typically this is done by using two approaches: 1) identifying “tag” SNPs that exist in a haplotype with other SNPs so that only one of the SNPs needs to be assayed to get 17 18 information on both, and 2) remove SNPs that have low minor allele frequencies (e.g. <5%), since it is unlikely that such alleles provide much information to association studies. 4. Determine the appropriate platform to assay the selected SNPs. This will depend largely upon the number of SNPs comprising the panel, the number of samples (patients) that are to be evaluated, the number of samples that can be batched together for efficiency, and the turnaround time necessary for the work. 5. Develop assays if necessary. For example, with Taqman many of the assays may already be developed, whereas for Sequenom multiplexed panels we always have to develop novel assays because even if we’ve assayed the variant before, each multiplex behaves a little different. 6. Run the samples. Some pilot studies have to be made and a power analysis to determine the sample size. We also have to consider the question of race: there are differences in the genome between races which clearly can influence interpretation of the results. The polymorphism study can justify that we register race. When the number of SNPs grows beyond a half dozen or so, then the Sequenom platform is often more cost effective. However, this is only the case when a large number of samples are analyzed. The sample would be linked to data from the present study such as sex, race, ethnic background, cancer diagnosis and therapy and oral complications. The sample will be coded by the enrolment site/patient sequential number (e.g. A/053). None of the data collected with the questionnaires will contain personal health identifiers, therefore only researchers at the enrolment site will have a key to determine the donor’s identity. This key will not be provided to other researchers. The samples will be stored for possible future genetic studies that are outside the remit of the current grant proposal. We anticipate seeking separate funding and ethical approval in the future for additional analysis of this material. Appropriate consent will be obtained for this polymorphism study and possible future genetic studies. 18 19 NCI CTCAE v.3 Whenever possible, adverse events will be measured by validated scales (see Variables below). For assessment of several adverse events, the US National Cancer Institute Common Terminology Criteria for adverse events (NCI CTCAE) version 3 (33) will be used. The NCI CTCAE v.3 displays grades 1 through 5 with clinical descriptions of severity for each adverse event (Table 3). Quality of life will be measured by the Oral Mucositis Daily Questionnaire (OMDQ). Table 3. NCI CTCAE v. 3 grading scale, based on the following general guideline GRADE SEVERITY 1 Mild 2 Moderate 3 Severe 4 life-threatening or disabling 5 death related to adverse event(s) Variables Whenever possible, validated instruments to measure symptoms will be used. Oral Findings (Complications) to be included in the study Subjective Oral Findings/Complications: Finding/Complication Method for Instrument data Timing (Phase) collection Oral pain (Severity and Location) Validated Scales - NCI CTCAE v.3 III (34) -.WHO pain ladder (35), adapted (40) Xerostomia (Dryness vs. Viscosity) Scale (one or more) - NCI CTCAE v.3 Taste Changes (Dysgeusia) (Abnormal vs. Decreased) Dysphagia (Difficulty to eat, speak and swallow) Scale - J. Epstein scales (36) III Scale - NCI CTCAE v.3 III I, III, V - VAS scale 19 20 Objective Oral Findings/Complications: Finding/Complication Method for data collection Scales Instrument Timing (Phase) - WHO (II, III, IV, V) (37) - Oral Mucositis Assessment Scale OMAS (III, IV) (8) II, III, IV, V -clinical judgement -culture when necessary -clinical judgement Clinical examination and description II, III, IV, V Clinical examination and description II, III, IV, V Existing dental and periodontal disease -clinical judgement /diagnosis I, II Dental and periodontal complications during cancer therapy -clinical judgement /diagnosis Osteonecrosis -clinical judgement /diagnosis -clinical judgement /diagnosis Salivary probe Clin. and radiographic examination of: number of remaining teeth/implants, caries, rootcanal treated teeth, chronic apical periodontitis, partially erupted wisdom teeth, plaque, calculus, marginal periodontitis Clin. and radiographic examination of: pulpitis, abscesses, pericoronitis, gingival bleeding and so on. Clin. and radiographic examination Clinical examination and description III, IV, V 5 minutes (mL/minutes) I, V Camera I-V when indicated Oral Mucositis Oral infections: viral, fungal or bacterial Submucosal hemorrhages GVHD Stimulated Salivary Flow (paraffin chewing) Others Photo documentation III, IV, V V 20 21 Signs to predict oral complications. Finding/Complication Salivary sample (2 mL from stimulated saliva) for the genetic polymorphism study Method for data collection Instrument Timing (Phase) Salivary probe Gene expression analysis I Timing (Phase) Confounding variables Finding/Complication Method for data collection Instrument Demographics Patient records, Interviewing age, gender, race I (White, Black, Hispanic, Asian, Other) Cancer Diagnosis Patient records Diagnosis Name I Cancer Therapy Patient records I, II Type of transplant Antimicrobial prophylaxis Pat records Patient records Previous CT, RT and investigational therapies; CT for current HSCT Auto or allo Type, dose, duration KGF medication Patient records Type, dose, duration III Immunosuppr. for GVHD Patient records Type, dose, duration III, IV, V Recommendations for Patient records local special oral care programs+individualized patient recommendations Nausea Scale Type, dose, duration III NCI-CTCAE v.3 III Vomit Scale NCI CTCAE v.3 III Diarrhea Scale III, V Fever Patient records Number of episodes during last 24 hours (OMDQ questionnaire) Celsius Weight Patient records Kg or Pound II, III, IV, V II, III Blood values Patient records WBC, PTL II,III,IV,V II II, III 21 22 Outcome Measures General Clinical Outcomes as a result from Oral Findings/Complications Finding/Complication Method for Instrument Timing data collection (Phase) Systemic infection Patient records Type of infection, symptoms, duration, CRP, temperature (type, dose, duration) II, III, IV, V Add. antibiotic therapy Patient records Narcotic analgesics Patient records Oral or i.v. Type, dose, duration (type, dose, duration) III, IV, V Other add. medication Patient records Nutrition Patient records III Patient records Total Parenteral Nutrition; Enteral Nutrition (Feeding Tube); solid, liquid, enteral vs. parenteral Kg Weight Survival Patient records Y/N, days VI III, IV, V III, IV, V III, , V Economic Outcomes as a result from Oral Findings/Complications Finding/Complication Method for data collection Instrument Timing (Phase) Days of Hospitalization Patient records Days III, IV Emergency Department or Additional Hospital Visits Patient records Emergency Dental Consultations Clinical examinations or patient history Number of Visits, III, IV Location of Visits, Timing (Days after Tx) Number of Visits, III, IV, V Location of Visits, Timing (Days following transplantation) 22 23 Quality of Life (QoL) QoL variables potentially affected by oral complications Finding/ Method for Instrument Complication data collection Quality of Life issues Questionnaire Oral Mucositis Daily related to symptoms from once a week for Questionnaire the oral cavity in-patients. (OMDQ) (38) Follow-up after 1 year. For allogeneic once a year thereafter Global questions on Questionnaire Study specific Oraeffects of oral cavity on Once/week for Stem questions general well-being in-patients. Follow-up after 1 year. For allogeneic once/year thereafter Timing (Phase) III, V III, V See MedView for a full version of the study form. 23 24 Statistic analyses and Sample size Analyses will be primarily descriptive in nature. Continuous variables will be assessed by Student’s t-test or Wilcoxon Rank-Sum test, and dichotomous variables by chisquare or Fisher exact test, with a critical value of 0.05. For multivariate analyses, variables thought to have prognostic value will first be analyzed by univariate analysis and appropriate variables (p<0.1) will be entered into a multivariable logistic regression analysis. Odds ratios will be calculated to represent the relative risk of the predictor variables. Analyses will be performed with the SAS statistical program (SAS Institute Inc., Cary, North Carolina, USA). Primary Aim – Sample Size The overall aim of the current prospective international observational multicenter study is to establish the nature, incidence and temporal relationship of oral complications related to conditioning regimen Estimated risk of patient-reported oral complications among subjects undergoing HSCT Sample sizes were selected (conservatively) to provide acceptable precision for estimates of risk for oral complications. The source of the expected incidences is included in Table 4. These samples sizes were determined with α = 0.05 and differing levels of acceptable absolute precision. Table 4. Expected incidence of oral complications after HSCT and estimated sample size to reach a statistically significance level of 95%. Oral Complication Estimate source Expected Incidence Sample Size Precision Mucositis Preliminary study 65% Xerostomia (31) 40% Oral Pain (29) 45% Dysphagia Preliminary literature review 54% 237 133 83 244 140 86 251 148 91 252 +/- 6% +/- 8% +/- 10% +/- 6% +/- 8% +/- 10% +/- 6% +/- 8% +/- 10% +/- 6% 139 93 +/- 8% +/- 10% 24 25 GVHD* (39) 7-54% 62-252 Dysgeusia Preliminary study 38% Oral Viral (25) 43% Oral Fungal (24) 38% 246 133 88 254 148 93 252 142 91 +/- 6% +/- 8% +/- 10% +/- 6% +/- 8% +/- 10% +/- 6% +/- 8% +/- 10% +/- 6% +/- 8% +/- 10% * Dependent on donor matching with acute GVHD 20-48% for matched related-donor and up to 90% for an unrelated donor. 35%-60% of patients with acute GVHD will have oral manifestations. Using the most conservative estimate, a total of 254 patients will need to be enrolled to obtain 6% precision for the main oral complications listed in Table 4. Ethical approval / Informed consent A separate ethical application will have to be done for each country involved. In the US, there are 18 specified identifiers that are not allowed, decided by US Government (see Appendix 1). Of most significance, birth dates or dates of the examinations can not be included, so will need to code as day -4 to day +20 etc…, depending when the stem cells are given. Some national adjustments may have to be done. Study Timeline Start of study 2011. 25 26 Fig 1. Allogeneic Check-up At 100 days Check-up At 6 months Check-up At 9 months Check-up At 12 months Tx (day 0) Oral exam Check-up 6-8 weeks 1-2 days before before Bedside examinations from day 0 (or +1 day), mon, wed, fri until resolution of neutropoenia or, if patient continues to have mucositis until discharge Check-up At 100 days Questionnaire at 12 months Autologous PHASE I PHASE II PHASE III PHASE IV PHASE V 26 27 Contact List Name E-mail Skype Mike Brennan +1 704-355-5774 [email protected] mike.brennan01 Inger v. Bültzingslöwen +46 (0)703-922072 [email protected] Katjavb Karin Garming-Legert +46 (0)705-488326 [email protected] karingl1 Bengt Hasseus +46 (0)730-882425 [email protected] Peter Johansson +46 (0)762-645902 [email protected] Jan Erik Johansson [email protected] Mats Jontell +46 (0)702-268105 [email protected] 27 28 Reference List 1. Dreizen S. Description and incidence of oral complications. NCI Monogr. 1990;9:11-5. 2. World Health Organization: Cancer 2005 [cited 5 A.D. Sep 26]: . Available from http://www.who.int/cancer/en/. 3. Executive summary. In: U.S.Department of Health and Human Services, editor. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institute of Health; 2005. p. 1-13. 4. NCI Monogr., 1990. 5. Sonic ST, Elting LS, Keefe D, Peterson DE, Schubert M, Hauer-Jensen M, Bekele BN, Raber-Durlacher J, Donnelly JP, Rubenstein EB, et al. Perspectives on cancer therapyinduced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer 2004;100(S9):1995-2025. 6. Rubenstein EB, Peterson DE, Schubert M, Keefe D, McGuire D, Epstein J, Elting LS, Fox PC, Cooksley C, Sonis ST, et al. Clinical practice guidelines for the prevention and treatment of cancer therapy-induced oral and gastrointestinal mucositis. Cancer 2004;100(S9):2026-46. 7. Spielberger R, Stiff P, Bensinger W, Gentile T, Weisdorf D, Kewalramani T, Shea T, Yanovich S, Hansen K, Noga S, et al. Palifermin for oral mucositis after intensive therapy for hematologic cancers. N.Engl.J.Med. 2004;351:2590-8. 8. Sonis ST, Oster G, Fuchs H, Bellm L, Bradford WZ, Edelsberg J, Hayden V, Eilers J, Epstein JB, LeVeque FG, et al. Oral mucositis and the clinical and economic outcomes of hematopoietic stem-cell transplantation. J.Clin.Oncol. 2001;19(8):2201-5. 9. Elting LS, Cooksley C, Chambers M, Cantor SB, Manzullo E, Rubenstein EB. The burdens of cancer therapy. Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer 2003;98(7):1531-9. 10. Bennett CL, Lane D, Stinson T, Glatzel M, Buntzel J. Economic analysis of amifostine as adjunctive support for patients with advanced head and neck cancer: preliminary results from a randomized phase II clinical trial from Germany. Cancer Invest. 2001;19(2):107-13. 11. Ruescher TJ, Sodeifi A, Scrivani SJ, Kaban LB, Sonis ST. The impact of mucositis on a-hemolytic streptococcal infection in patients undergoing autologous bone marrow transplantation for hematologic malignancies. Cancer 1998;82(11):2275-81. 28 29 12. Raber-Durlacher JE, Weijl NI, Abu Saris M, de Koning B, Zwinderman AH, Osanto S. Oral mucositis in patients treated with chemotherapy for solid tumors: a retrospective analysis of 150 cases. Support Care Cancer 2000;8:366-71. 13. Rapoport AP, Miller Watelet LFM, Linder T, Eberly S, Raubertas RF, Lipp J, Duerst R, Abboud CN, Constine L, Andrews J, et al. Analysis of factors that correlate with mucositis in recipients of autologous and allogeneic stem-cell transplants. J.Clin.Oncol. 1999;17(8):2446-53. 14. Sonis S, Edwards L, Lucey C. The biological basis for the attenuation of mucositis: the example of interleukin-11. Leukemia 1999;13(6):831-4. 15. Lockhart PB, Sonis ST. Alterations in the oral mucosa caused by chemotherapeutic agents: A histologic study. J.Dermatol.Surg.Oncol. 1981;7(12):1019-25. 16. Dorr W, Spekl K, Martin M. Radiation-induced oral mucositis in mice: strain differences. Cell Prolif. 2002;35(s1):60-7. 17. Ulrich CM, Yasui Y, Storb R, Schubert MM, Wagner JL, Bigler J, Ariail KS, Keener CL, Li S, Liu H, et al. Pharmacogenetics of methotrexate: toxicity among marrow transplantation patients varies with the methylenetetrahydrofolate reductase C677T polymorphism. Blood 2001;98(1):231-4. 18. Jontell M, Mattsson U, Torgersson O, Jontell M, Mattsson U, Torgersson O. MedView: an instrument for clinical research and education in oral medicine. Oral Surg.Oral Med.Oral Pathol.Oral Radiol.Endod. 2005;99(1):55-63. 19. Jontell M, Torgersson O. Meadview: a computerised teaching aid in oral medicine and oral pathology 2010 [cited 2010 Jan 19]:1-13. Available from http://www.rhu.se/activities/projects/financed_projects/i-j/jontell_mats_99_final.pdf. 20. Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions 4.2.5 2005 [cited 5 A.D. May 31]: . Available from http://www.cochrane.dk/cochrane/handbook/hbook.htm. 21. Migliorati CA, Woo SB, Hewson I, Barasch A, Elting LS, Spijkervet FK, Brennan MT. A systematic review of bisphosphonate osteonecrosis (BON) in cancer. Support.Care Cancer. Forthcoming. 22. Hong CH, Napenas JJ, Hodgson BD, Stokman MA, Mathers-Stauffers V, Elting LS, Spijkervet FK, Brennan MT, Dental Disease Section OCSGMAoSCiCMISoOOI. A systematic review of dental disease in patients undergoing cancer therapy. Oral Care Study Group, Multi-national Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO). Support.Care Cancer. Forthcoming. 23. Hovan AJ, Williams PM, Stevenson-Moore P, Wahlin YB, Ohrn KE, Elting LS, Spijkervet FK, Brennan MT. A systematic review of dysgeusia induced by cancer therapies. Support.Care Cancer. Forthcoming. 29 30 24. Lalla RV, Latortue MC, Hong CH, Ariyawardana A, mato-Palumbo S, Fischer DJ, Martof A, Nicolatou-Galitis O, Patton LL, Elting LS, et al. A systematic review of oral fungal infections in patients receiving cancer therapy. Support.Care Cancer 2010 May 8. 25. Elad S, Zadik Y, Hewson I, Hovan A, Correa ME, Logan RM, Elting LS, Spijkervet FK, Brennan MT. A systematic review of viral infections associated with oral involvement in cancer patients. Support.Care Cancer. Forthcoming. 26. Brennan MT, Elting LS, Spijkervet FK. Systematic reviews of oral complications from cancer therapies, Oral Care Study Group, MASCC/ISOO: methodology and quality of the literature. Support.Care Cancer. Forthcoming. 27. Brennan MT, Spijkervet FK, Elting LS. Systematic reviews and guidelines for oral complications of cancer therapies: current challenges and future opportunities. Support.Care Cancer. Forthcoming. 28. Peterson DE, Doerr W, Hovan A, Pinto A, Saunders D, Elting LS, Spijkervet FK, Brennan MT. Osteoradionecrosis in cancer patients: the evidence base for treatmentdependent frequency, current management strategies and future studies. Support.Care Cancer. Forthcoming. 29. Epstein JB, Hong C, Logan RM, Barasch A, Gordon SM, Oberlee-Edwards L, McGuire D, Napenas JJ, Elting LS, Spijkervet FK, et al. A systematic review of orofacial pain in patients receiving cancer therapy. Support.Care Cancer. Forthcoming. 30. Bensadoun RJ, Riesenbeck D, Lockhart PB, Elting LS, Spijkervet FK, Brennan MT. A systematic review of trismus induced by cancer therapies in head and neck cancer patients. Support.Care Cancer. Forthcoming. 31. Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN, Dutilh J, Fulton JS, Jankovic L, Lopes NN, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support.Care Cancer 2010 Mar 17. 32. Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN, Dutilh J, Fulton JS, Jankovic L, Lopes NN, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: management strategies and economic impact. Support.Care Cancer. Forthcoming. 33. Colevas AD, Setser A. The NCI common terminology criteria for adverse events (CTCAE) v 3.0 is the new standard for oncology clinical trials. J.Clin.Oncol. 2004 Jul 15;22(14S):6098. 34. National Cancer Institute. Common terminology criteria for adverse events (CTCAE). Version 3.0 ed. Bethesda, MD: Cancer Therapy Evaluation Program; 2003. 35. WHO Expert Committee on Cancer Pain Relief and Active Supportive Care. Cancer pain relief and palliative care: report of a WHO expert committee [meeting held in Geneva from 3 to 10 July 1989]. Geneva: World Health Organization; 1990. Report No.: 804. 1-75 p. 30 31 36. Epstein JB, Phillips N, Parry J, Epstein MS, Nevill T, Stevenson-Moore P. Quality of life, taste, olfactory and oral function following high-dose chemotherapy and allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2002;30(11):785-92. 37. World Health Organization. WHO handbook for reporting results for cancer treatment. Geneva: World Health Organization; 1979. Report No.: 48. 1-45 p. 38. Stiff PJ, Erder H, Bensinger WI, Emmanouilides C, Gentile T, Isitt J, Lu ZJ, Spielberger R. Reliability and validity of a patient self-administered daily questionnaire to assess impact of oral mucositis (OM) on pain and daily functioning in patients undergoing autologous hematopoietic stem cell transplantation (HSCT). Bone Marrow Transplant. 2006;37(4):393-401. 39. Schubert MM, Correa ME. Oral graft-versus-host disease. Dent.Clin.North Am. 2008;52(1):79-109. 40. Elting LS, Keefe DM, Sonis ST, Garden AS, Spijkervet FK, Barasch A, Tishler RB, Canty TP, Kudrimoti MK, Vera-Llonch M. Patient-reported measurements of oral mucositis in head and neck cancer patients treated with radiotherapy with or without chemotherapy: demonstration of increased frequency, severity, resistance to palliation, and impact on quality of life. Cancer. 2008;113(10):2704-13. 31