Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
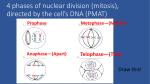
The image above illustrates an NADH-TR stain showing dark type 1 and pale type 2 fibers.
The latter would appear dark in ATPase stain. At least two subtypes are now identified
among type 2 fibers using different methods of staining. All of the muscle fibers in a given
motor unit are of the same histochemical types, either type 1 or type 2, suggesting that the
neuron determines the type of muscle fibers. The fibers of adjacent motor units overlap and
intermingle resulting in a characteristic mosaic or checkerboard pattern.
This H&E image shows a large group of atrophic fibers [center] next to a
group of normal fibers (left), a typical example of group atrophy.
The denervated muscle fibers are in the vicinity of intact axons and may become
reinnervated by collateral sprouting. Since the motor neuron determines the
muscle fiber type, all of the re-innervated fibers are converted to a single
histochemical fiber type with loss of the normal checkerboard pattern.
This phenomenon is called "type grouping." The image above illustrates typical
type grouping in an ATPase stain. Note the area of dark type 2 fibers next to a
large area of pale type 1 fibers. Normal checkerboard pattern is lost.
The frontal chest radiograph showed a large antrerior mediastinal soft tissue
mass on the right side adjacent to the heart. A plain and contrast enhanced CT Chest
showed a large, well defined, lobulated, anterior and superior mediastinal mass with
cystic components. In view of the clinical presentation this lesion was thought to be
thymoma.
Amytrophic lateral sclerosis:
weakness, atrophy, fasciculations
hyperreflexia
Note atrophy in ALS
Lou Gehrig—famous
N.Y. Yankee first
baseman who had
ALS and thus it is
commonly called “Lou
Gehrig disease.”
note thin ventral
roots in ALS
patient-why?
Lumbosacral radiculopathy.
Sagittal MRI showing loss of
intervertebral disc height at L5/S1.
Herniations of the nucleus
pulposus are noted at L4/5 and
L5/S1
Think about patient’s problems,
physical exam and tests you
would request to verify your
diagnosis!
Chief complaint
Right leg pain
History of present illness
42 year old female with an eight week
history of mostly right leg pain. The pain
radiates to the sole and outside of her foot
and is accompanied by numbness and
tingling. This episode of pain started as back
pain but within a week had moved to being
mostly in her leg.
Physical exam
42 year old healthy female who stands through
most of the history. She has an absent ankle jerk on
the right leg. There are no focal motor deficits, and
the neurological exam is otherwise negative.
She has a markedly positive straight leg test and
crossed straight leg test (raising the affected and
unaffected leg recreates her leg pain).
Imaging studies
MRI scan shows a large disc herniation at L5-S1.
There is also disc degeneration present at the L5-S1
disc. The axial scan (not shown) shows that the disc
impinges on the right S1 nerve root.
This is an image of an MRI of the normal
lumbar spine [low back]. The vertebrae are
marked with numbers; one can see lumbar
vertebrae 2 through 5 and finally the S1
vertebra [which is the Sacral #1 vertebrae].
The discs are in-between the vertebrae and
are number accordingly. For example, the
L3/4 disc has a black arrow pointing to it.
The discs always have 2 numbers for
identification. The Red arrow points to the
fluid in spinal canal; this fluid appears as a
whitish color on the MRI. The Blue arrow
points to a nerve roots in the canal.
MRI delineates a mass of the distal 6
centimeters of the spinal cord
involving the conus medullaris,
(which ends at the upper aspect of
L2).
Think about this patient’s neurological
deficits/problems!
A 34-year-old man suffered from severe neck
and shoulder radicular pain of 1 year
duration. His pain soon became electric-like,
shooting in nature and involving the left
upper limb and ulnar side of the left hand.
Neurologically, he had minimal sensory
impairment over the left C7 dermatome.
An MRI of the cervical spine demonstrated a
C6-C7 herniated nucleus pulposus ((at right)
A needle electromyogram examination
confirmed the presence of a C6-C7
radiculopathy.
bony metastasis affecting
cauda equina
see the conus just dorsal to it?
possible deficits in comparison to
conus lesions?
Representative of Case History #1
DUCHENNES MUSCULAR DYSTROPHY
•marked enlargement of calves
•hyperlordosois
•decreased tendon reflexes
•normal sensation
Gower’s Sign
Representative of Case History #2
•in A, patient is
attempting to raise
eyelids as high as
possible
MYASTHENIA GRAVIS
•In B, same patient
has had an iv
injection of Tensilon,
an
acetylcholinsterase
inhibitor. Eyelids go
higher for a while
A
B
Cervical or lumbar? Arrow points to ?????
Think of the neurological
deficits/pathways/tests
associated with SCD!
Write a practice question
For me! Please make E
the answer so I can
answer it correctly