Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
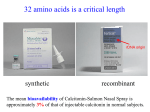
Unit 1 St James Business Park Grimbald Crag Court Knaresborough HG5 8QB Our ref: MMT/AdvisoryNote/Bone Metabolism Date May 2016 To: Practice Prescribing Leads Practice Managers Re: Bone Metabolism Dear Colleague, For the May “Hints and Tips on Prescribing”, the Medicines Management Team would like to focus on prescribing of bisphosphonates and other drugs for the treatment of bone metabolism disorders. Data from the Regional Drugs and Therapeutics Centre (RDTC) indicates that HaRD CCG has a low prescribing frequency of bisphosphonates and other drugs for bone metabolism disorders compared to other CCGs in Yorkshire and Humber. This data also identifies that HaRD is the highest weighted prescriber of denosumab in the Yorkshire and Humber region and prescribes more than 3 times the national average of denosumab. This may be appropriate but we would encourage practices to ensure that appropriate patients have had bone densitometry and are being treated accordingly. Our local HDFT osteoporosis guidelines (below) identifies the full list of patients who should be considered for bone densitometry with supporting advice. http://www.harrogateformulary.nhs.uk/chaptersSubDetails.asp?FormularySectionID=6&SubSectionRef=06. 06&SubSectionID=A100. These guidelines also provide advice on interpreting the results of DEXA scans to determine if treatment is required. It recommends the following treatment options for osteoporosis: First-line - generic alendronate 70 mg once weekly Second-line alternative bisphosphonate, e.g. risedronate 35mg once weekly, if intolerant to alendronate monthly ibandronate may be considered but only has proven efficacy for reduction of vertebral fractures. intravenous zoledronic acid (annual infusion) may be considered if oral bisphosphonate not tolerated. Third line - Strontium ranelate if intolerant of bisphosphonates, or other therapy ineffective (further osteoporotic fracture after at least 12 months therapy). See below for further advice re strontium. Fourth line - Denosumab (by subcutaneous injection 6 monthly) if intolerant of bisphosphonates or other therapy ineffective (had a further osteoporotic fracture after at least 12 months therapy). If no treatment is indicated, give advice about maximising calcium intake and high impact exercise to maintain bone density. Osteoporosis Monthly briefing/letter – May 16 Page 1 of 3 HaRD Medicines Management Team Advice from MHRA re prescribing of strontium Strontium ranelate is now restricted to the treatment of severe osteoporosis in postmenopausal women and adult men at high risk of fracture who cannot use other osteoporosis treatments due to, for example, contraindications or intolerance. Treatment should only be started by a physician with experience in the treatment of osteoporosis. The risk of developing cardiovascular disease should be assessed before starting treatment. Treatment should not be started in people who have or have had: ischaemic heart disease peripheral arterial disease cerebrovascular disease uncontrolled hypertension Cardiovascular risk should be monitored every 6–12 months. Treatment should be stopped if the individual develops ischaemic heart disease, peripheral arterial disease, or cerebrovascular disease, or if hypertension is uncontrolled. Annual Cost of Bone Metabolism Drugs Denosumab prescribed in HaRD CCG (March 2015 – Feb 2016) Osteoporosis Monthly briefing/letter – May 16 Page 2 of 3 HaRD Medicines Management Team Duration of treatment The HDFT guidelines make the following recommendations on the duration of treatment: Generally 3-5 years. Ten years if previous fragility fracture to the spine, femur, pelvis or sacrum – discontinue bisphosphonates after 10 years given increased risk of atypical stress fracture, especially of the femoral shaft, with prolonged usage. Continue for the duration of high dose steroids or active disease causing secondary osteoporosis – although again discontinue bisphosphonates after 10 years given increased risk of atypical stress fracture. Follow-up scans have a definite value in the following situations: For patients with active disease causing secondary osteoporosis, for example primary hyperparathyroidism or rheumatoid arthritis. For patients on continuous steroid therapy, equivalent to prednisolone 5 mg od or more, probably at 1-3 year intervals depending on baseline BMD, disease severity or steroid dose. Where treatment is stopped after 5 years there is no necessity for re-scanning. Evidence suggests that after 10 years from baseline, 5 years on bisphosphonates then 5 years off is as effective as 10 years continuous usage. Re-scanning after 5 years off treatment may be helpful in assessing the need for a further course of treatment. If treatment is not indicated, but T < -1.0 with additional risk factors and within 5 years of menopause or of stopping HRT, then repeat DEXA in 5 years. Action points Check that appropriate patients have had bone densitometry. Ensure that alendronate is used as the first line choice. Ensure treatment is reviewed after 3-5 years, as per the HDFT guidelines. Denosumab should be initiated by a consultant, in accordance with shared care guidelines (SCG), and should be reviewed after 4 years, as per HDFT guidelines. Link to SCG for denosumab: http://www.harrogateformulary.nhs.uk/chaptersSubDetails.asp?FormularySectionID=6&SubSection Ref=06.06.02&SubSectionID=A100 Ensure that patients on denosumab are prescribed calcium and vitamin D supplements as appropriate. Please share this information with all the prescribers in your practice. The prescribing support team is available to help practices with this work. HaRD versions of OptimiseRx and SystmOne and EMIS formularies will be amended to incorporate these recommendations. Should you have any queries, recommendations or ideas about these or future initiatives then we would be pleased to hear from you. Yours sincerely, The Medicines Management Team, HaRD CCG. References BNF vol 70 September 2015. Department of Health Drug Tariff May 2016. Drug Safety Update. May 2014. MHRA. Osteoporosis Monthly briefing/letter – May 16 Page 3 of 3 HaRD Medicines Management Team