Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
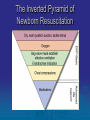
Care of the Newborn Neo-natal Resuscitation Presence Regional EMS July 2016 CE Objectives Review the anatomy and physiology of the neonate, concentrating on the cardio/respiratory changes that occur at birth. Outline the assessment of the new born infant Discuss the use of the “Inverted Triangle” for organizing resuscitation of the neonate, including how much time should be spent on the activities of each level Using a variety of scenarios, demonstrate the resuscitation of the distressed newborn. The Dramatic Trauma of Birth The moving of an infant from the warm water bath of the uterus into the “cold cruel world” and be dramatic and traumatic. But it has to be in order for the new infant to survive. While in the uterus the fetus is totally dependent on the placenta to leech oxygen and nutrients from the mother’s circulation Essentially the fetus’s lungs and GI tract are non functional. The lungs are full of fluid. Blood is bypassed from these areas Blood fresh from the placenta full of oxygen and nutrients enters the fetal body via the umbilical vein at the ductus venous in the liver At the heart, blood bypasses the lungs via two short cuts The foramen ovale between the atria in the heart The ductus arteriosis connecting the pulmonary artery and the aorta At Birth Several things happen to make the lungs functional: Compression of the infant’s chest during delivery through the vagina pushes out 1/3 of fluid Blood flow through the umbilical cord slows in preparation for separation First Breath Stimulated by Hypothermia (20+ degree drop from uterus to outside world) Hypoxia (decrease in blood flow from placenta = decrease in oxygen) Drop in blood pH Initiation of stretch receptors in lung As infant gasps with change in temperature and hypoxia breathing begins As lungs fill with air Remaining fluid in lung is displaced Pulmonary arterioles and capillaries open and resistance to blood flow decreases so lung vessels fill with blood Change in pressure causes blood to flow into lungs rather than through “short cuts” Ductus venosis, ductus arteriosis and foramen ovale are no longer needed Increased pressure in right and left chambers of the heart force Structures closed Blood is diverted away from these structures. “Slam shut” Structures close and transition into ligaments Temperature In addition to the dramatic drop in temperature during delivery Infants have poorly developed thermoregulation Infants have a difficult time maintaining a constant body temperature Keep the newborn WARM Healthy Newborn Not necessarily NORMAL Healthy Newborn A Healthy Newborn should: Be wet and slippery (be careful) Respiratory rate 40-60 per minute Heart rate 130-180 per minute Pink skin of head, chest and abdomen Cyanosis of arms and legs Oxygen saturation of 70-80% but rises rapidly Use APCAR score to document assessment The APGAR Score Standard scoring system used to assess the status of a newborn Assigns a number value to five areas: Appearance Pulse Grimace or irritability Activity or muscle tone Respirations The APGAR Score The APGAR Score Appearance If the skin of the newborn’s entire body is blue (cyanotic) or pale, award 0 points. If the newborn has blue hands and feet with pink skin at the core of the body, award 1 point If the skin of the extremities as well as the trunk is pink, award 2 points. The APGAR Score Pulse Heart rate is one of the most important signs of whether oxygen is reaching the newborn’s tissues following birth. Count the heart rate for at least 30 seconds, preferably with a stethoscope. If you do not have a stethoscope, feel the pulse of the umbilical cord where it joins the abdomen or at the brachial artery. If no pulse is present, award 0 points. If the heart rate is under 100 (also a serious finding), award 1 point. If the heart rate is over 100, award 2 points. The APGAR Score Grimace (reflex irritability) Gently flick the soles of the newborn’s feet, or observe the facial expressions during suctioning. If the newborn displays no reflexive activity to your stimulation, award 0 points. If the newborn displays only some facial grimace, award 1 point If your stimulation causes the newborn to grimace and cough, sneeze, or cry, award 2 points. Activity The APGAR Score This score refers to extremity reflexes/movement, or the degree of flexion of the arms and legs and the resistance to straightening them. The normal newborn’s elbows, knees, and hips are flexed, and you should encounter some degree of resistance when you try to extend them. If during your assessment, the newborn is limp and displays no extremity movement, award 0 points. If the newborn only displays some flexion without active movement, award 1 point. If the newborn is actively moving around, award 2 points. The APGAR Score Respiration Another important assessment sign is the newborn’s breathing effort. The newborn should have regular respirations and a vigorous cry. Distress is indicated by irregular, shallow, gasping, or absent respirations. If the newborn displays no respiratory effort, award 0 points If the newborn displays only a slow or irregular breathing effort with a weak cry, award 1 point If the newborn displays good respirations and a strong cry, award 2 points. The APGAR Score The total of the five numbers is the Apgar score. A perfect score is 10. Calculate the Apgar score at 1 minute and 5 minutes after birth. The APGAR Score 7–10 points—The newborn should be active and vigorous. Provide routine care. 4–6 points—The newborn is moderately depressed. Provide stimulation and oxygen. 0–3 points—The newborn is severely depressed. You will probably need to provide extensive care including oxygen with bag-valve-mask ventilations and CPR. Resuscitation of the Newborn: Give every chance Neonatal Assessment and Resuscitation Follow standard precautions. Always put on gloves before handling a newborn. Protecting is critical! the newborn against heat loss Neonatal Assessment and Resuscitation Newborn should begin breathing spontaneously within 15 to 30 seconds after birth Also assure that the airway is clear of all secretion or birth fluids. Perform additional suctioning as needed Heart rate should be 100 beats/min or higher If you do not observe these responses: Gently tap or flick the soles of the feet or rub the back. Begin resuscitation efforts. Neonatal Assessment and Resuscitation Most newborns (80% +) require no resuscitation beyond temperature maintenance, mild stimulation, and suctioning. A minority of the newborns will be so depressed that they also will need chest compressions or resuscitative medications. Signs of Severely Depressed Newborn Respiratory rate over 60 per minute Diminished breath sounds Heart rate over 180 per minute or under 100 per minute Obvious signs of trauma from the delivery process Poor or absent skeletal muscle tone Respiratory arrest, or severe distress Heavy meconium staining of amniotic fluid Weak pulses Cyanotic body (core and extremities) Poor peripheral perfusion Lack of or poor response to stimulation APGAR score under 4 Meconium Fetal fecal matter Greenish black and sticky Presence in amniotic fluid or on newborn infant = Sign of fetal distress Neonatal Resuscitation To keep straight what needs to be done for the newborn in what order. . .Don’t panic!!! Follow the inverted pyramid The Inverted Pyramid of Newborn Resuscitation Management Priorities: Immediate Care of the Newly Born Dry, warm, position, suction, and stimulate the infant. Clear the airway. Assess breathing. Assess heart rate. Assess color. Post Delivery Care Aggressively dry off the infant and wrap in a blanket or towel. Place the infant on one side, with the head slightly lower than the rest of the body. Wrap the infant so only the face is exposed. Keep the blanket or towel warm. Management Priorities: Vaginal Delivery While drying and warming the baby. Clear the airway by suctioning if necessary Check for spontaneous breathing (crying) If the baby is not breathing/crying well Begin resuscitation of the baby as needed. Delivery of placenta is non-emergent. Neonatal Assessment and Resuscitation Observe the newborn for spontaneous respirations, skin color, and movement of the extremities for APGAR Score Evaluate the heart rate at the base of the umbilical cord or the brachial artery. The heart rate is the most important measure in determining the need for further resuscitation. Neonatal Assessment and Resuscitation If cyanosis is present but breathing and heart rate are adequate, provide blow-by oxygen Neonatal Assessment and Resuscitation Provide ventilations by bag-valve-mask with supplemental oxygen at the rate of 40–60 per minute if the newborn displays any of the following: The infant’s breathing is shallow, slow, gasping, or absent following brief stimulation. The infant’s heart rate is less than 100 beats per minute. The infant’s core body remains cyanotic (blue) despite provision of blow-by oxygen. Management Priorities: Bag-Mask Ventilation Extend the head slightly on the neck. Position hands in “EC-clamp.” Ventilate at 40–60 breaths per minute. Courtesy of David J. Burchfield, MD Neonatal Assessment and Resuscitation Reassess after 30 seconds of ventilation. If the breathing has not improved and the heart rate is less than 100/minute, continue ventilations and reassess every 30 seconds. Management Priorities: Assess Heart Rate Palpate a pulse at the base of the umbilical cord. Count for 6 seconds and multiply by 10. If cord pulse cannot be palpated, listen for heartbeat with a stethoscope. Management Priorities: Newborn Resuscitation If the heart rate remains <60 beats/min, after 30 seconds of bag-mask ventilation, begin chest compressions. 3:1 compression to ventilation ratio 90 compressions and 30 breaths/min (120 “events” per minute) Reassess heart rate after 30 seconds Neonatal Assessment and Resuscitation Use either the handencircling technique or the two-finger technique. Coordinate chest compressions with ventilations at a ratio of 3:1. Neonatal Assessment and Resuscitation: Review Key Concept: The Inverted Pyramid: If Chest Compressions not affective, need ALS care and medications Neonatal Assessment and Resuscitation ALS If heart rate is < 60 beats/min after another 30 seconds CPR, consider intubation. Prepare epinephrine dose of 0.01 to 0.03 mg/kg (0.1 to 0.3 mL/kg of the 1:10,000 solution) ET/IV/IO. Neonatal Resuscitation BLS Shock Treatment The newborn may be in shock due to fluid loss. Shock symptoms: Poor perfusion Weak pulses Poor response to resuscitation. Shock treatment: Rapid transport. Neonatal Resuscitation ALS Shock Treatment Assure adequate oxygenation and ventilation. Obtain intravenous access: Intravenous: first choice Intraosseous: second choice Umbilical venous: if trained and equipped 10–20 mL/kg normal saline or Ringer’s lactate ALS Check Blood Glucose Infants have poor glucose reserves The stress of delivery may deplete glucose stores Give 2-4 ml/kg (1-2 ml/pound) of 10% dextrose IV/IO for low blood glucose Key Concepts: Newborn Resuscitation Oxygen therapy :Not appropriate to give supplemental oxygen to all infants only those in distress Monitoring: After resuscitation, reassess infant status throughout transport. Hypothermia: Keep the baby warm during transport.--Cover head with a knit cap. Newborn hypoglycemia: Assess blood glucose after 30 minutes. Once infant is stable or at first opportunity Post Delivery Care Clamp Wait and cut the umbilical cord until pulsation of cord stops Place 2 clamps First clamp approximately 7 inches from baby. Second clamp approximately 2-3 inches from first Cut with sterile scissors. Clamp and Cut the Cord Monitor ends for bleeding, if bleeding occurs place another clamp proximal to the initial clamp. Neonatal Resuscitation Pearls of Wisdom Good assessments and care in first 15 minutes of life Keep your head Follow the triangle. Review Answer the following questions as a group. If doing this CE individually, please e-mail your answers to: [email protected] Use “July 2016 CE” in subject box. You will receive an e-mail confirmation. Print this confirmation for your records, and document the CE in your PREMSS CE record book. Review Scenario 1: You and your partner are dispatched to the local shopping mall for a 17 year old female with severe abdominal pain. When you arrive you find your patient lying on the floor of the bathroom and discover that she has just given birth. The newborn is face down on the bathroom floor. The mother is stable. Review The infant is a 31 week gestation baby girl . You dry, warm, position, suction and stimulate the infant but despite these interventions the infant remains flaccid with irregular respiratory effort and a weak cry. Central cyanosis is also present and the heart rate is 40. Review 1. 2. 3. 4. Calculate the AGPAR score of this newborn infant. What are the BLS treatment priorities for this newborn infant? If the respirations don’t improve in heart rate doesn’t go up in 30-45 seconds, what must be done? The infants heart rate has not improve, now what will you do? Review 5. What is the appropriate rate of compressions and the compressions to ventilations ratio during CPR for the newborn? 6. Resuscitation is taking priority with this infant, but you think the umbilical cord should be secured. Where should the clamps be placed? Where should the cord be cut? 7. The infant’s heart rate does not improve. ALS providers decide to gain vascular access. What are the choices for this? 8. The infant appears to weigh about 4 pounds. How much of what concentration of epinephrine should be considered by ALS providers? 9. The infant has a low blood sugar of 40. What are the options for this problem? 10. The infant is now crying. Her respirations are spontaneous at a rate of 44. Her pulse has improved to 140. Her head and chest are pink but her arms and legs are still cyanotic. She is moving her arms and legs weakly. What is her APCAR score now? Answers 1. 2. 3. 4. APGAR Score is 2 Position head down. Continue to dry, suction and stimulate, apply blow by oxygen. Being ventilations with Bag-valve-mask at a rate of 40-60 Begin chest compressions 5. 3:1 compression to ventilation ratio 90 compressions and 30 breaths/min (120 “events” per minute) 6. Once the cord has stopped pulsating, place the first clamp 7 inches from infant. Second clamp goes 2-3 inches from the first. Cut between the clamps. 7. IV or IO or ET (if intubated) 8. 0.01 to 0.03 mg/kg (0.1 to 0.3 mL/kg) of Epinephrine 1:10,000 solution ET/IV/IO. This is .02 mg or 0.2 ml for this child. 9. Give 10% dextrose IV/IO at 1-2 ml/pound. This is 4-8 ml for this child. 10. APCAR is 8