Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
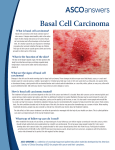
The American Society of Clinical Oncology (ASCO) Net Health Benefit (NHB) Assessment Tool: Which Implications for Value Assessment of Cancer Therapies? Rémuzat 1 C, Chouaid 2 C, Auquier 3 P, Borget 4 I, Kornfeld 1 M, Toumi 3 M 1Creativ-Ceutical, Paris, France; 2Centre Hospitalier Intercommunal, DHU-ATVB, Créteil, France; INSERM U955 and Université Paris Est (UPEC), UMR U955, Faculté de médecine, Créteil, France3Faculté de Médecine, Laboratoire de Santé Publique, Aix-Marseille Université, Université de la Méditerranée, Marseille, France; 4Institut Gustave Roussy, Villejuif, France BACKGROUND • • Financial toxicity concept was recently introduced in the United States related to financial distress resulting from out-of-pocket payments of costly cancer medicines [1]. In this context, the American Society of Clinical Oncology (ASCO) developed in 2015 a framework (updated in 2016) to support physicians and patients in assessing value of new cancer therapies and to facilitate dialogue between physicians and patients [2,3]. OBJECTIVES • This research aimed to review the ASCO value framework and to identify its contributions and limits for fair decisions toward cancer medicines options. • • Drug acquisition costs and patient out-of-pocket payment are also considered but not included in the NHB. Since ASCO value framework allows to weight cost with clinical benefits and side effects, it has been considered as a potential valuable tool for oncologists and may have a potential to impact a clinical practice [5,9]. However, several limitations of the framework were reported by the authors themselves and by other stakeholders, which could limit it usefulness in providing physicians and patients with properly informed basis for making treatment decisions [Figure 2]. Figure 2. Factors potentially limiting adoption of ASCO framework to the practice Lack of patient-centeredness • Despite the incorporation of QoL into the framework it awards only 10 points for QoL improvement and does not include other factors significant for patients such as work productivity, unmet need, and burden of disease [5,6,7]. METHODS • • This issue is related to the lack of relevant data in clinical trials, and the authors of the framework hope that such endpoints will be included in a larger number of clinical trials in the future [2]. ASCO value framework (initial version and update [2,3]) was reviewed and analysed to identify: Dimensions taken into account to assess the value of cancer drugs, Its contribution for patients and physicians’ shared-decision making in Inability to perform cross-trial comparisons • If two alternative therapies were not compared within a single trial it is not possible to compare them using the framework. It is due to the methodological differences between clinical trials, especially in terms of patient population and comparator used [3,7], since different outcomes can be observed when: treatment options. A drug is compared to placebo or to active treatment, A drug is used in patient populations with different prognosis. A comprehensive literature review was also performed to identify discussions on the practical usability of the framework. Difficult interpretation of outcomes for patients RESULTS • • • • • The interpretation of the value score could be challenging, in particular for patients, mainly because of two reasons: ASCO value framework is built to compare new cancer therapies versus standard of care using data from prospective randomised trials The use of hazard ratio (HR) might be misinterpreted by patients while a favourable HR does not necessarily represent a large absolute gain in OS or PFS (and this should be well explained by the physicians) [3]. The NHB scale length, reaching from -20 to 130 points, suggests that the score in the middle of the scale is not a high score. However it has been shown that mid-range scores should be interpreted as excellent rating and that the entirety of the scale is rarely applied [8]. (single-arm trial data might be accepted if sole available data; response rate should be used in this case). The framework includes 2 sub-frameworks: For advanced cancers, For potentially curative treatments (adjuvant or neoadjuvant therapy). Both of these sub-frameworks include 2 main dimensions computed in net health benefit (NHB): Clinical benefit including overall survival (OS), progression-free survival (PFS), response rate (RR), disease-free survival (DFS) depending on available data, Toxicity. NHB calculation includes clinical benefit score, toxicity score and bonus points (Figure 1): Maximum scoring for clinical benefit is 100 (more important weight on OS versus PFS or RR), while being 20 for toxicity. Bonus points are awarded for tail of the survival curve (20 points); advance disease framework also includes palliation of symptoms (10 points) and/or treatment-free interval (20 points) and/or quality of life (QoL) (10 points). • The need to explain the framework outcomes to a patient during a time-limited visit could discourage physicians from using the framework within their clinical practice [7]. Consideration of drug cost only • The framework does not allow to include other costs than costs of drugs. This is important to consider since [9]: • • • Initially, QoL was deliberately not included in the framework, reflecting the lack of QoL data in many clinical trials. Figure 1. Outcomes included in the Net Health Benefit calculation Advanced disease Median OS HR for death HR for disease progression Median OS Median PFS HR for DFS RR Median DFS OR • OR OR OR OR OR NHB Toxicity Zafar SY et al. Oncologist. 2013;18(4):381-90. Schnipper LE et al. J Clin Oncol. 2015 Aug 10;33(23):2563-77. Schnipper LE et al. J Clin Oncol. 2016 Aug 20;34(24):2925-34. Lederman L. Value Tools at ASCO 2016: Building a Framework fro Prime Time. ZS Associates 2016. (http://www.zsassociates.com/publications/articles/value-tools-atasco-2016-building-a-framework-for-prime-time.aspx) 5. Westrich K. Current Landscape: Value Assessment Frameworks. National Pharmaceutical Council. Mar 2016. • Tail of the curve REFERENCES 1. 2. 3. 4. readily available in clinical trials [2,3], A software application is currently being developed which will facilitate fast access to relevant information and adjustment of selected parameters to fit patient preferences [2,3,6]. Despite being still a conceptual tool, the ASCO value framework is the one most commonly used among other value frameworks, as showed in a survey conducted with 93 oncologists during the ASCO 2016 Annual Meeting [4]. CONCLUSIONS OR Tail of the curve Palliation QoL Treatment-free interval The limitations above should not be treated as permanent barriers for the framework uptake because: The authors foresee an improvement in the future when more data will be Adjuvant setting HR for death Toxicity The cost of a drug is usually only 20-25% of the total cancer care cost, New drugs may generate savings in cost components such as hospitalisation. The authors argue that incorporation of additional cost data into the framework would be problematic because such information is not readily available, nor easily quantifiable [3]. 6. 7. 8. 9. (http://www.npcnow.org/publication/current-landscape-valueassessment-frameworks) Bankhead C. MedPage Today. Feb 2016. (http://www.medpagetoday.com/publichealthpolicy/healthpolicy/582 73) Pratt-Chapman M et al. Value in Oncology. Oct 2015, Vol 6, No 9. Subramanian R, Schorr K. How valuable is a cancer therapy? It depends on who you ask. Simon-Kuchner. Dec 2015. (http://www.simonkucher.com/sites/default/files/how_valuable_is_cancer_therapy.pdf) Okon T. VBCC Perspectives. Jul 2015, Vol 6, No 6. • ISPOR 19th Annual European Congress, Vienna, Austria, OCT 29 – NOV 02, 2016. PRM15. ASCO value framework represents clear improvement in supporting physicians’ and patient’s decisions for cancer therapies but the use of the tool might be complex in daily clinical practice unless all products are already scored for relevant conditions. In general, it reflects more physicians’ perspective: • Clinical benefits are overrated versus toxicity and only 10 bonus points awarded for QoL, which may have more importance for patients • Moreover, as the cost is just a background information not influencing the NHB, the usefulness of the framework for payers is rather marginal. However, this tool is continuously evolving through feedback of various stakeholders with strong willingness to improve patient’s empowerment.