Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
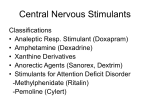
NARCOLEPSY Month of Birth as a Risk Factor for Narcolepsy Yves Dauvilliers, MD1,3; Bertrand Carlander, MD1; Nicolas Molinari, PhD2; Alex Desautels, MSc4; Michele Okun, MA5; Mehdi Tafti, PhD6; Jacques Montplaisir, MD, PhD4; Emmanuel Mignot, MD, PhD5; Michel Billiard, MD1 1Service de Neurologie B, Unité des Troubles du Sommeil, Hôpital Gui-de-Chauliac Montpellier, France; 2Institut Universitaire de Recherche Clinique, Montpellier, France; 3Inserm EMI 9930, Hôpital La Colombière, Montpellier, France; 4Centre d’Etude du Sommeil, Hôpital du Sacré-Cœur, Montréal, Canada; 5Stanford University Center for Narcolepsy, Palo Alto, CA; 6Unité de Biochimie et Neurophysiologie Clinique, Genève, Suisse Study Objectives: A loss of hypocretin neurons has been observed in human narcolepsy; however, the cause of this disorder is still unknown. While family history and genetic factors are important individual risk factors for narcolepsy, environmental factors also contribute to the pathogenesis of the disease. The aim of the study was to find out whether there is a seasonality of month of birth in narcoleptic patients. Design: Diagnosis of narcolepsy with cataplexy was based on International Classification of Sleep Disorders criteria with clinical, standard polysomnographic, and Multiple Sleep Latency Test features Patients and Setting: The birth dates of 886 patients with a clear-cut diagnosis of narcolepsy with cataplexy from 3 large narcolepsy databases (352 from Montpellier-France, 157 from Montreal-Canada, and 377 from Stanford-United States of America) were compared with those of 35,160,522 subjects from the general population. Measurements and Results: Patients with narcolepsy had a significantly different seasonality of month of birth compared to that of the general population. The monthly distribution of birth yielded a peak in March with a maximal odds ratio at 1.45 and a trough in September with a minimal odds ratio at 0.63. No gender or country of origin differences were observed. Conclusions: A birth seasonality in the development of narcolepsy suggests the presence of environmental factors acting in combination with genetic factors during the fetal or perinatal period, in terms of an autoimmune process targeting the hypocretin system. Key Words: Narcolepsy, season of birth, autoimmune, hypocretin Citation: Dauvilliers Y; Carlander B; Molinari N et al. Month of birth as a risk factor for narcolepsy. SLEEP 2003;26(6):663-5. INTRODUCTION and autoimmune disorders such as type 1 diabetes mellitus and Crohn disease.17,18 In narcolepsy, preliminary data based on a small population also suggest a potential difference in the month of birth in comparison with the general population.19 The purpose of the present study is to examine the pattern of annual cyclic variation in month of birth of patients with narcolepsy compared to the general population in 3 large narcolepsy cohorts from Montpellier, Montreal, and Stanford. HUMAN NARCOLEPSY IS A DISORDER CHARACTERIZED BY 2 MAJOR SYMPTOMS: EXCESSIVE DAYTIME SLEEPINESS AND CATAPLEXY. Recent research has significantly advanced understanding of the underlying pathophysiology of narcolepsy; however, the exact etiology of this disorder remains uncertain.1-4 The loss of hypocretincontaining neurons appears to be a consistent feature of the disorder, and it has been hypothesized that this loss may be attributable to an autoimmune mechanism. The close association with the HLA DQB1*06025 and probably tumor necrosis factor-α gene,6 together with the bimodal distribution of age at onset,7 support this hypothesis. Also, the low rate of familial cases and the low concordance in monozygotic twin studies favor the involvement of environmental factors as in many other autoimmune disorders.8,9 Analysis of patterns of birth is a potentially important way to assess the role of early-life environmental factors in the pathophysiology of the disease. Environmental risks, such as infectious agents, could trigger the disease through the induction of an autoimmune process.10-11 Should this occur during the fetal period, it could cause damage to the central nervous system. As infectious disorders commonly show seasonal variation, temporal patterns of month of birth of narcoleptic patients would differ from that of the general population, as has been previously reported in other neurologic diseases.12,13 Several studies have suggested, for example, that season of birth may play a pathogenic role in the development of Parkinson disease, schizophrenia, multiple sclerosis, autism,12-16 PATIENTS AND METHODS Dates of birth of 886 well-defined narcoleptic-cataplectic subjects known to 3 large sleep disorder clinics were obtained: 352 (237 male and 115 female) in the Montpellier Sleep Wake Disorders Center, 157 (87 male and 70 female) in the Montreal Sacré-Cœur Sleep Disorders Center, and 377 (167 male and 210 female) in the Stanford University Sleep Disorders Clinic. Diagnoses were made by sleep-disorder specialists on the basis of the International Classification of Sleep Disorders.20 All patients had a typical clinical history of narcolepsy with recurrent daytime naps or lapses into sleep and clear-cut cataplexy (defined as a sudden bilateral loss of postural muscle tone in association with intense emotion), the hallmark of the disorder. Patients had a standard polysomnographic recording including 1 all-night recording in the sleep laboratory followed by the Multiple Sleep Latency Test performed according to standard methods.21 Most of the narcoleptic patients showed a mean sleep latency of less than 8 minutes and 2 or more sleep-onset rapid eye movement periods (SOREMPs). However, only 1 or no SOREMPs was also documented in 10% to 15% of the patients in each center in spite of well-defined excessive daytime sleepiness and cataplexy (diagnosis in accordance with International Classification of Sleep Disorders criteria19). The birth distribution for the narcoleptic population ranged from 1901 to 1994. The distribution by month and year in the general population was obtained for each country from civil registries. Live-birth data for each decade from 1910 to 1990 were obtained for each center (Table 1). The general population included 6,416,584 persons in France, 793,834 persons in Quebec, and 27,950,104 persons in the United States, giving Disclosure Statement No significant financial interest/other relationship to disclose. Submitted for publication December 2002 Accepted for publication April 2003 Address correspondence to: Dr. Yves Dauvilliers, Service de Neurologie B, Hôpital Gui-de-Chauliac, 80 avenue Augustin Fliche, 34295 Montpellier cedex 5, France; Tel: +33 04 67 33 72 77 ; Fax: +33 04 67 33 72 85 ; E-mail : [email protected] SLEEP, Vol. 26, No. 6, 2003 663 Month of Birth as a Risk Factor for Narcolepsy—Dauvilliers et al a total pooled reference population of 35,160,522 persons (Table 1). The expected number of births of narcoleptic patients, calculated as the proportion of the general population born in each month throughout the study period, was compared to the observed number of births of patients for the pooled population and by center of origin. Results were expressed as odds ratios with the general population as the reference category. The odds ratio was then defined as follows: for each month, we compared the observed number of births of patients to the pooled population against 1 of the 11 other months. Hence, 12 χ2 tests with 1 degree of freedom were performed. A Bonferroni correction was applied to interpret the P-value. We also divided the pooled data into 4 seasonal periods delineated by groups of months (winter: January, February, March; spring: April, May, June; summer: July, August, September; and autumn: October, November, December) and data were analyzed by χ2. In addition, the effect of gender and center of origin on the monthly distribution of birth in narcoleptic patients was evaluated using χ2 distributions. Statistical analysis were performed with S-plus package version 3.4 (Mathsoft). Statistical significance was set at P< 0.05. icant drop in September (χ2 = 10.09, df=1, P=0.0015) were observed (Table 1). The month of March was clearly the month where the number of narcoleptic births was the highest in all cases (11.85% of patients), higher than the value expected in the general population (8.45 %) (Table 1). Figure 1 shows the odds ratio of the month of birth in the pooled narcoleptic population. The maximal calculated odds ratio for the season of birth was 1.45 (95% confidence interval, 1.06-1.98) observed in March. These percentages, derived from the clinical cohorts, are unlikely to be representative of the general population due to recruitment bias. However, no differences in the distribution of month of birth in narcoleptic patients was observed among centers of origin (χ2 = 22.18, df = 22, P=0.45). Moreover, they do show similar tendencies across the 3 sites (Table 1). A second lower peak in August is also evident in Figure 1, though this was significant only in the French population (Table 1; χ2 = 7.17, df = 1, P=0.007). September was the month where the narcoleptic births were the lowest (5.64% of patients), and lower than the value expected in the general population (8.71%) (Table 1). Accordingly, September was the month of birth associated with the minimal relative risk (odds ratio at 0.63; 95% confidence interval, 0.43-0.91), which corresponds to a 37% reduction in the risk for narcolepsy. Analysis of seasonal periods displayed one peak in winter (January to March) in the narcoleptic patient group when compared to the general population (χ2=7.98, df=3, P=0.04). However, most of this result was explained by an excess number of narcoleptic subjects born in March. Finally, there was no significant difference in the seasonality trend of birth between the sexes (491 male, 395 female) (χ2=6.3 df=11, P=0.85). There was no clear change in the monthly distribution of births over the century in either the general population or in the narcoleptic group. RESULTS Monthly distribution of births among narcoleptic patients differed significantly from that expected on the basis of the general population (χ2= 26.81, df = 11, P=0.004) (Table 1). A significant excess of narcolepsy among persons born in March (χ2= 12.85, df=1, P=0.0003) and a signif- DISCUSSION This is the first large study of birth seasonality in narcoleptic patients including 3 sleep disorders centers. The results demonstrate that the number of narcoleptic subjects born in March significantly exceeds that expected, with no differences based on gender, recruitment center, or decade of birth. There was no clear variation in seasonal birth rate in the general population. The risk of narcolepsy was at its maximum in March and at its minimum in September (Table 1, Figure 1). Preliminary results on the narcoleptic Stanford population included in this study were partially reported in a previous work.19 Although an excess of births in the month of March had been noticed, statistical analysis had not revealed a significant difference between narcoleptics and the general population in the United States. Our results are also comparable to those obtained for several other central nervous system diseases such as schizophrenia14,22 and Parkinson disease12 and for autoimmune diseases such as diabetes Figure 1—Odds ratios of narcolepsy according to month of birth. The data points and verand Crohn disease,17,18 all showing a birth excess during winter. tical bars show the relative risks and 95% confidence intervals, respectively, with month of The effect of season of birth is a potentially important way to assess birth analyzed as a categorical variable. the role of early-life environmental factors in a disease. The Table 1—Month of birth in narcolepsy (3 cohorts of narcoleptic subjects) compared with rates expected from the finding of a seasonal birth patgeneral population (pooled general population data from France, Canada, and the Unites States of America). tern for a specific disease that significantly differs from the Month France Quebec USA Total Total General observed expected population birth pattern of the general % % % % % % population suggests that the Observed Expected Observed Expected Observed Expected N % N % N origins of the disease date very January 10,51 8,56 6,37 7,99 7,43 8,19 75 8,47 73,11 8,25 2,901,381 early in life. These data may February 8,81 8,19 7,64 7,60 7,69 7,72 72 8,13 69,10 7,80 2,742,148 March 11,93 8,91 12,74 8,85 11,41 8,33 105 11,85 74,82 8,45 2,969,392 provide clues for the disease April 6,53 8,60 5,10 8,78 10,34 7,74 70 7,90 70,16 7,92 2,784,217 etiology; however, a preferenMay 7,95 8,76 11,46 9,04 7,16 8,02 73 8,24 72,46 8,18 2,875,494 tial season of birth does not June 6,25 8,27 8,92 8,69 7,43 8,13 64 7,22 72,36 8,17 2,871,448 July 6,82 8,57 10,83 8,79 7,69 8,85 70 7,90 77,94 8,80 3,092,990 reveal specifically when the August 12,50 8,40 9,55 8,45 9,02 9,04 93 10,50 78,92 8,91 3,131,895 environmental factor occurred. September 5,68 8,10 5,10 8,49 5,84 8,85 50 5,64 77,16 8,71 3,062,135 Environmental factors may October 9,38 8,01 8,92 8,05 8,22 8,63 78 8,80 75,35 8,50 2,990,325 have occurred during the pregNovember 5,40 7,65 7,64 7,56 9,28 8,10 66 7,45 70,94 8,01 2,815,160 December 8,24 8,00 5,73 7,73 8,49 8,41 70 7,90 73,68 8,32 2,923,937 nancy in the first (summer), Total 352 100,00 157 100,00 377 100,00 886 100 886 100 35,160,522 the second (autumn) or the SLEEP, Vol. 26, No. 6, 2003 664 Month of Birth as a Risk Factor for Narcolepsy—Dauvilliers et al third trimester (winter) or in the first few months following the birth (spring) when the brain undergoes a rapid development. Moreover, seasonal factors may differ among different geographic areas such as in France, in Quebec, and in the United States. However, a significantly excess number of narcoleptic subjects born in March was observed in those 3 different narcoleptic populations. Several known factors could be involved, such as infectious agents, nutrition effects, temperature, or fluctuations of neurotransmitter systems. If the seasonal birth factor is etiologic, one explanation for this effect is infectious agents, since many of them vary seasonally. In addition, the involvement of infectious agents has been reported in other central nervous system diseases such as the poliovirus in Parkinson disease12 and the influenza virus in schizophrenia,13 and also in autoimmune disease such as coxsackie in type 1 diabetes mellitus.23 Two studies have reported that narcoleptics have elevated antibodies to streptococcal antigens,24,25 although this was not confirmed by a later study.26 In addition, secondary narcolepsy after encephalitis, although rare, has been described.27 A seasonal predominance of birth in narcolepsy could provide clues for such an event (infectious agents) having occurred early in life, causing some form of neuronal injury within the sleep structures. Degeneration of hypocretin neurons is clearly implicated in human narcolepsy, although the cause of the degeneration is still unknown, but an autoimmune process remains the most likely candidate.3,4 The transient nature of such a process, together with the low number and focal localization of hypocretin neurons in the brain, could explain the absence of direct evidence of autoimmunity. The pronounced seasonal variation of date of birth in narcoleptic subjects may suggest that environmental factors may be harmful to the developing hypocretin cells. The hypothesis of an autoimmune process against hypocretin neurons starting in the fetal or perinatal period during annual viral epidemics deserves further considerations. In addition, we may hypothesize that the low relative risk for children born in September to develop narcolepsy may be due to protective immune factors. Based on differential genetic susceptibility, only a minority of subjects may experience sufficient initial damage to ultimately develop narcolepsy. The close association with the HLA DQB1*06025 and probably with the tumor necrosis factor-α gene6 together with monthly variations in environmental factors may interact to cause a damage to the hypocretin system that will result in narcolepsy. We therefore hypothesize that genetically susceptible individuals exposed to specific, but yet undetermined, environmental factors might develop narcolepsy through a neurodegenerative process that targets hypocretin neurons. Finally, the seasonal variation of date of birth could be linked to seasonal fluctuations in the hypocretin metabolism, as has already been reported for other neurotransmitter systems such as the serotonergic and dopaminergic systems.28-30 If seasonal fluctuation in the hypocretin system is further demonstrated, the season of birth could be implicated as a pathogenic factor in narcolepsy. More specifically, if a low hypothalamic hypocretin-neuron activity were observed for subjects born in winter, that may constitute a predisposing factor to hypocretin deficiency. In summary, this study suggests that narcoleptic subjects have an excess of births in March and a decrease in September. The fetal or perinatal period could be a vulnerable time for the action of an etiologic agent, which may cause damage to the hypocretin system. Additional research is needed to further elucidate the interaction between environment and genetic-vulnerability factors in narcolepsy and to explore the nature of putative agents. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. Thannickal TC, Moore RY, Nienhuis R, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000;27:469-74. Mignot E, Lin L, Rogers W, et al. Complex HLA-DR and -DQ interactions confer risk of narcolepsy-cataplexy in three ethnic groups. Am J Hum Genet 2000;68:686-99. Hohjoh H, Nakayama T, Ohashi J, et al. Significant association of a single nucleotide polymorphism in the tumor necrosis factor-alpha (TNF-alpha) gene promoter with human narcolepsy. Tissue Antigens 1999;54:138-45. Dauvilliers Y, Montplaisir J, Molinari N, et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001;57:2029-33. Mignot E. Genetic and familial aspects of narcolepsy. Neurology 1998;50:S16-22. Montplaisir J, Poirier G. Narcolepsy in monozygotic twins. Neurology 1987;37:1089. Mignot E, Tafti M, Dement WC, Grumet FC. Narcolepsy and immunity. Adv Neuroimmunol 1995;5:23-37. Carlander B, Eliaou JF, Billiard M. Autoimmune hypothesis in narcolepsy. Neurophysiol Clin 1993;23:15-22. Mattock C, Marmot M, Stern G. Could Parkinson's disease follow intra-uterine influenza?: a speculative hypothesis. J Neurol Neurosurg Psychiatry 1988;51:753-6. Barr CE, Mednick SA, Munk-Jorgensen P. Exposure to influenza epidemics during gestation and adult schizophrenia. A 40-year study. Arch Gen Psychiatry 1990;47:869-74. Mortensen PB, Pedersen CB, Westergaard T, et al. Effects of family history and place and season of birth on the risk of schizophrenia. N Engl J Med 1999;340:603-8. Templer DI, Trent NH, Spencer DA et al. Season of birth in multiple sclerosis. Acta Neurol Scand 1992;85:107-9. Stevens MC, Fein DH, Waterhouse LH. Season of birth effects in autism. J Clin Exp Neuropsychol 2000;22:399-407. Ursic-Bratina N, Battelino T, Krzisnik C, Laron-Kenet T, Ashkenazi I, Laron Z. Seasonality of birth in children (0-14 years) with type 1 diabetes mellitus in Slovenia. J Pediatr Endocrinol Metab 2001;14:47-52. Ekbom A, Wakefield AJ, Zack M, Adami HO. Perinatal measles infection and subsequent Crohn's disease. Lancet 1994;344:508-10. Okun ML, Lin L, Pelin Z, Hong S, Mignot E. Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;25:27-35. International classification of sleep disorders, revised: diagnostic and coding manual. Rochester, MN: American Sleep Disorders Association; 1997. Carskadon MA, Dement WC, Mitler MM, Roth T, Westbrook PR, Keenan S. Guidelines for the Multiple Sleep Latency test (MSLT): a standard measure of sleepiness. Sleep 1986;9:519-24. Fuller Torrey E, Yolken RH. Familial and genetic mechanisms in schizophrenia. Brain Res Brain Res Rev 2000;31:113-7. Mikulecky M, Michalkova D, Petrovicova A. Coxsackie infection and births of future diabetic children: year, seasonality and secularity. J Pediatr Endocrinol Metab 2000;13:523-7. Billiard M, Laberti MF, Reygrobellet C, Seignalet J, Brissaud L, Besset A. Elevated antibodies to streptococcal antigens in narcoleptic subjects. Sleep Res 1989;18:201. Montplaisir J, Poirier G, Lapierre O, Montplaisir S. Streptococcal antibodies in narcolepsy and idiopathic hypersomnia. Sleep Res 1989;18:271. Mueller-Eckhardt G, Meier-Ewart K, Schiefer HG. Is there an infectious origin of narcolepsy? Lancet 1990;335:424. Adie WJ. Idiopathic narcolepsy: a disease sui generis; with remarks on the mechanisms of sleep. Brain 1926;49:257-306. Carlsson A, Svennerholm L, Winblad B. Seasonal and circadian monoamine variations in human brains examined post mortem. Acta Psychiatr Scand 1980;280:75-85. D'Hondt P, Maes M, Leysen JE, et al. Seasonal variation in platelet [3H]paroxetine binding in healthy volunteers. Relationship to climatic variables. Neuropsychopharmacology 1996;15:187-98. Roy-Byrne PP, Uhde TW, Sack DA, Linnoila M, Post RM. Plasma HVA and anxiety in patients with panic disorder. Biol Psychiatry 1986;21:849-53. REFERENCES 1. 2. 3. Nishino S, Ripley B, Overeem S, Lammers GL, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000;355:39-40. Nishino S, Ripley B, Overeem S, et al. Low cerebrospinal fluid hypocretin (orexin) and altered energy homeostasis in human narcolepsy. Ann Neurol 2001;50:381-8. Peyron C, Faraco J, Rogers W, et al. A mutation in a case of early onset narcolepsy and a generalized absence of hypocretin peptides in human narcoleptic brains. Nat Med 2000;6:991-7. SLEEP, Vol. 26, No. 6, 2003 665 Month of Birth as a Risk Factor for Narcolepsy—Dauvilliers et al