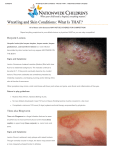
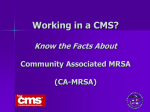
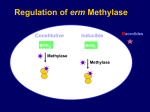
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Case Studies in Sports Dermatology Kent Scheff MD University of Michigan Primary Care Sports Medicine Fellow Disclosures • None Objectives • Be able diagnose common infections encountered in the training room. • Choose appropriate therapy for the above infections • Be able to propose an appropriate time for athletes to return to competition following infection • Propose methods for reducing further infection and recurrence. Case #1 Too Close for Comfort Case #1 • 19 y.o. Wrestler • 2 day history of rash on face • Initially started with tingling/burning sensation • Vesicular rash appeared on day 2, some lesions have started to scab/crust • Presents for evaluation • Holiday Tournament scheduled in 3 days Case #1 Herpes Gladiatorum • Caused by Herpes Simplex Virus 1 • Prominent among wrestlers and in other sports with skin to skin contact • Accounts for 39% of skin infections in the NCAA injury surveillance of wrestlers • Incubation is 2-20 days however, most lesions appear after 3-5 days of exposure Herpes Gladiatorum • Initial presentation is seen on head, neck, face (right side) ears, torso or upper extremities • Primary infections may present with constitutional symptoms along with burning, tingling or stinging at the site • Vesicles then form on an erythematous base • Vesicles ulcers plaques Herpes Gladiatorum vesicles Herpes Gladiatorum ulcers Herpes Gladiatorum Crust Diagnostic Methods • Gold standard is Viral Culture remembering that maximum sensitivity is achieved in 2-7 days. • Sample base of a disrupted vesicle during active lesion • HSV PCR test is more sensitive and faster though more expensive • Serology IgM 20-25 days, IgG 6-8 weeks after exposure Treatment • Early treatment is key; virus exponentially replicates within the first 48 hours • Acyclovir 400 mg TID • Valacyclovir 1 gm BID 7-10 days • Famciclovir 500 mg Bid • Recurrence: identical dosing for 5 days Return to Play • Free of systemic symptoms • No new lesions for 72 hours • All lesions must be dry with a firm adherent crust • Appropriate treatment with a systemic antiviral for 120 hours prior to competition • Active lesions are not to be covered to allow competition Prevention • Early diagnosis and quarantine of affected athletes • Athlete education “no sharing” of towels • Disinfection of commonly used items, mats, exercise equipment • Antiviral prophylaxis has been shown to decrease acquisition and spread of Herpes Gladiatorum in wrestlers • Valacyclovir 500 mg to 1 gm daily Case #2 Training Room Challenge Case #2 • 20 y.o. football player presents with a “spider bite” on his leg that has been present for 4 days. • It is progressing in size and is uncomfortable • Treated over the weekend in urgent care with Keflex with no improvement. Community Acquired MRSA • Most S.aureus are beta-lactamase producing, resistant to penicillin, but susceptible to cephalosporins and the penicillinase-resistant penicillins (nafcillin, oxacillin, dicloxicillin), or Blactam-B-lactamase inhibitor combinations (e.g., amoxicillinclavulanate) CA-MRSA • Increased prevalence of S.aureus that have the mecA gene that produces the penicillin-binding protein PBP2a • Confers resistance to all currently FDAapproved B-lactams CA-MRSA • Study of University affiliated ERs found that 76% of skin/soft tissue infections caused by S. aureus – 59% of total due to MRSA – 77.8% of S. aureus were MRSA – 99% of MRSA were CA-MRSA CA-MRSA • Median age of HA-MRSA: 68 yrs • Median age of CA-MRSA: 23 yrs • 2006 survey of Texas Athletic Trainers found that 32% had treated MRSA infections in their athletes CA-MRSA • Typical presentation is a pustular lesion with central necrosis • Pain is often out of proportion to the size and appearance of the lesion • Patients often c/o of a “spider bite” CA-MRSA CA-MRSA • Class 1 infection –Lesion nonfluctuant –Patient afebrile, otherwise healthy CA-MRSA • Class 2 infection –Lesion fluctuant or pustular –Lesion < 5 cm in diameter –Patient afebrile, otherwise healthy CA-MRSA • Class 3 infection – Lesion > 5 cm in diameter – Patient toxic appearing or at least one unstable comorbidity or limb-threatening infection CA-MRSA • Class 4 infection – Sepsis syndrome of life-threatening infection (necrotizing fasciitis) CA-MRSA CA-MRSA • Incision and drainage alone without antibiotics has 90% cure rate • Use 11 blade to create a wide opening • Explore wound for loculations and pack • Frequent follow-up for approximately 2 weeks Rajendran et al. Antimicrob Agents Chemotherapy 2007;51:4044-48 CA-MRSA treatment • Class 1 infection –If no drainable abscess, prescribe first or second generation cephalosporin, semi-synthetic penicillin, macrolide, or clindamycin –Follow-up in 1-2 days to ensure response CA-MRSA • Class 2 infection – I&D the lesion – Frequent follow-up – If not healing within 7 days, empirically treat with TMP-SMX DS 2 tabs BID – Clindamycin and tetracycline are alternatives, but have slightly less efficacy CA-MRSA treatment • Class 3 and 4 infections –Admit to hospital –Consult surgery for aggressive debridement –Start vancomycin IV –Consult infectious disease specialist CA-MRSA Return to Play • Bacterial infections –Treatment for minimum 72 hrs –No new lesions within 48 hrs –No draining or “wet” lesions CA-MRSA Prevention • Washing/Showering with soap and warm water as soon as possible after competition/practice • Not Sharing soap bars, towels, razors or clothing • Prompt treatment of abrasions, cuts Case #3 Moisture is the Enemy Case #3 • 19 y.o. Baseball player presents with a lacy rash in his inguinal region • He describes it as “itchy” and it exacerbates when he sweats Tinea Infections • Dermatophytes survive on keratin in the stratum corneum layer of the skin • Warm, moist environments promote fungal growth • Tinea corpora in athletes is primarily spread by skin-to-skin contact • Skin scales containing fungal spores can live outside the host on inanimate surfaces Tinea Corporis and Pedis Tinea Diagnosis • Diagnosis can often be made by inspection • Scraping the edge of the lesion and examining with heated KOH prep heated under microscopy yields hyphae Tinea Treatment • Allylamines – Terbinafine – Naftifine – May have shorter treatment periods than imidazoles – Fungicidal Decreased liver toxicity • Imidazoles – Clotrimazole – Ketoconazole – Miconazole – Effective for most fungal infections, but may employ a longer treatment period – Fungistatic Tinea Treatment • Oral anti-fungals for widespread lesions, multiple recurrences –Fluconazole 150 mg q wk for 3 weeks –Itraconazole 200 mg qD for 2 weeks –Terbinafine 250 mg qD for 2 weeks Tinea Return to Play • NCAA and NFHS guidelines – Minimum of 72 hours of topical therapy needed for non-scalp infections – Minimum of 2 weeks of systemic antifungal for scalp infection before participation is allowed. – Lesions should be washed with selenium sulfide or ketoconazole shampoo, coated with naftifine or terbinafine cream then covered with pre-wrap and tape prior to competition Tinea Prevention • Similar to CA-MRSA recommendations – Athlete cleanliness – No sharing equipment such as helmets or towels – Reduce time practicing in hot/damp environments – Cleaning Mats helps, but major risk is skin to skin contact Case #4 My Achin’ Feet! Case #4 • 51 y.o. backpacker • Presents with a blister on his foot • Hiked in rough terrain for 7 miles with a 50 pound pack • Wore wool socks • A recreational runner, but not accustomed to Weight/terrain, etc Friction Blister Friction Blisters • Results from friction forces that separate epidermal cells at the level of the stratum spinosum • Potential space fills with fluid and/or blood Friction Blisters • Factors promoting blister formation – Moisture increases frictional forces – Heat – Poorly fitting shoes – New activities – Cotton socks Friction Blisters • Treatment – Decompress large blisters with a sterile needle. – Leave blister roof intact – “Second Skin” or petrolatum, donut pad, should be applied to minimize further friction at the site. – Prevention: acrylic or polyester socks Friction Blister Case #5 Case #5 • 20 y.o. soccer player presents with a pruritic rash for 2 days between the fingers and in beltline. • 21 y.o. football player presented later that day with similar symptoms and rash distribution • Yet another 21 y.o. soccer player presented with similar rash in the beltline. • What’s going on? Case #5 Scabies • Caused by mite Sarcoptes scabiei (0.4 mm) • Female mite attracted to warmth (intertriginous, beltline, groin, axillary regions) Scabies • Female mite makes a burrow, lays eggs 1-3 daily • Produces secretions that cause allergic rxn. • Larvae hatch from eggs travel to skin surface and also produce secretions. Scabies Treatment • Topical application of Permethrin (Elimite cream) from neck to toes at night. • Wash all bedclothing and suspected contaminated clothing in hot water. • Avoid sleeping on roomate’s couch that is infested. Summary • Reviewed examples of infections and blisters encountered in athletes • Reviewed Diagnosis and treatment • Plans for return to play • Reviewed suggested methods of prevention of infection and re-infection Bibliography • Pecci M, Comeau D, Chawla V. Skin conditions in the athlete. Am J Sports Med 2009;37:406-17. • McBride D. Managing community-acquired MRSA lesions: What works? OBG Management 2008;20:2833. • Cohen P. The skin in the gym. Clinics Derm 2008;26:1626. • http://www.cdc.gov/ncidod/dhqp/ar_mrsa.html • http://epa.gov/oppad001/chemregindex.htm • http://nfhs.org • http://www.mhsaa.com