Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
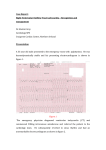
Nodal‐like cells exist in the right ventricular outflow tract O Monfredi1, RH Anderson2, MR Boyett1, H Dobrzynski1 1 Cardiovascular Research Group, The University of Manchester, United Kingdom; 2Cardiac Unit, Institute of Child Health, University College, London, United Kingdom Introduction • • • • • • The right ventricular outflow tract (RVOT), anatomically connecting the right ventricular working myocardium to the pulmonary artery via the pulmonary valve, remains one of the more scientifically neglected ‘Cinderella’ regions of the heart Despite this, the region is responsible for a significant amount of cardiac morbidity and mortality, especially associated with dysrhythmias Dysrhythmias arising from the RVOT may be associated with macroscopic anatomical abnormalities (such as those arising in the context of arrhythmogenic right ventricular dysplaisia ‐ ARVD, tetralogy of Fallot or catecholaminergic polymorphic ventricular tachycardia ‐ CPVT), or there may be a complete absence of anatomical abnormality, as seen in the RVOT subtype of idiopathic ventricular tachycardia (RVOT‐VT) The RVOT is recognised to have a unique embryological origin, maturing late and being mainly comprised of cells from the secondary heart field and some cardiac neural crest cells It has previously been suggested that the underlying cause of the RVOT’s propensity towards dysrhythmia could be the persistence of embryonic type tissue with pacemaking ability in the region surrounding the pulmonary valve (Christoffels et al (2009), Circ Arrhythm Electrophysiol 2:195‐207) We hypothesised that cells with characteristic features of pacemaker cells would be present in the region of the RVOT upon detailed anatomical and immunohistochemical examination Methods Results – histology Results – immunohistochemistry, continued A population of cells was apparent in the RVOT that was distinct from either those making up the working myocardium of the right ventricle and those making up the pulmonary valve and artery. This distinct population was smaller, more spindle‐shaped and substantially more loosely packed, mirroring many of the characteristics of pacemaker tissues. Fig 3 (left): Enlarged, high power (x63) microscope view of the region within the RVOT that contains the novel cells of interest. It can be clearly seen that compared to the inferiorly lying cells of the working right ventricular myocardium, the cells discovered within the RVOT are smaller, more spindle shaped and more loosely packed. Fig 6: Comparative immunohistochemistry from the RVOT and working right ventricular myocardium for important ion channels. Cx40 (first column) demonstrated absence in the right ventricular working myocardial cells, whilst in RVOT cells at high power, there appeared to be significant though low level cytoplasmic labelling for this gap junction protein that is typically localised to the Purkinje fibres in healthy individuals. The fast sodium channel, Nav1.5 (second column), was immunohistochemically below detectable levels in RVOT cells, whilst demonstrating strong membranous labelling in the ventricle. This may suggest that cells from the RVOT have a slow upstroke to their action potential, similar to pacemaking cells. The inwardly rectifying potassium channel, Kir2.1, was also below detectable levels in the RVOT cells, but demonstrated strong membranous labelling in the cells of the working right ventricular myocardium. This may suggest that the RVOT cells have an unstable resting membrane potential, similar to pacemaking cells. Fig 4 (above 2 panels): high‐power (x63) views of cells from the RVOT (leftward panel) and the working myocardium of the right ventricle (rightward panel), to emphasise the differences in size, morphology and overall cell‐cell relationship between the 2 populations Results – immunohistochemistry Substantial differences were found to exist between the novel cells of the RVOT and the working myocardium of the right ventricle. These are outlined below. Fig 1 (left): Schematic view of complete open‐book dissection of RVOT. The RVOT is removed from its position (yellow box, top diagram) and is pinned out face up (bottom diagram) and sectioned sagittally Fig 2 (right): low power microscope photograph of sagittally sectioned RVOT with luminal surfaces being present to the right side of the tissue section. The pulmonary valve is in the open position, apposed to the connective tissue comprising the pulmonary artery. Fig 5: High power (x63) view of the RVOT region, oriented as shown in Fig 3 above. Tissue is labelled for Cx43 (red) and caveolin3 (green). As one moves inferior to superior, the intensity of labelling for Cx43 markedly decreases, and is noticably sparse in the RVOT cells of interest. Labelling for caveolin3 is identical in both RVOT cells and the cells of the working myocardium, suggesting that the cells of interest are indeed cardiac myocytes, rather than a distinct population of ‘foreign’ cells. Fig 7: Comparative immunohistochemistry from the RVOT and working right ventricular myocardium for important ion channels and Ca2+‐handling proteins. The L‐type Ca2+ channel, Cav1.3, and the T‐type Ca2+ channel, Cav3.1, were below detectable levels in the working right ventricular myocardium. In the RVOT, however, Cav1.3 fluorescence was present with a membranous distribution. Similarly, fluorescence for Cav3.1 in the RVOT appeared positive. Cav1.3 and 3.1 are typically found in the pacemaker tissue of the heart, and the finding of their positive immunohistochemical labelling in cells from the RVOT further suggests that the cells may have a pacemaker phenotype or origin. Ryanodine receptor (RyR2) fluorescence was present in both cell types, though the distribution was markedly different. In the working myocardium, the classical labelling for RyR2 was present, with strong trabeculated intracellular fluorescence. However, in the RVOT cells, intracellular labelling was absent, with fluorescence being confined to the region close to the cell membrane, reminiscent of previous studies of SAN cell RyR2 immunohistochemistry. SERCA2A labelling was also strong, reproducible and close to the cell membrane in the RVOT, whilst in the working myocardium labelling did not appear to be associated with any discreet intracellular structure. These 2 findings may suggest that if indeed the RVOT cells are of pacemaker type, that the ‘Ca2+ clock’ mechanism of pacemaking is of predominant importance rather than the ‘membrane clock’. Notably, labelling for HCN4 was below detectable limits in both RVOT and myocardium. The same was true for labelling with NCX. Conclusions 1. The right ventricular outflow tract contains a previously undescribed population of cells that are histologically and immunohistochemically distinct from the cells of the surrounding working right ventricular myocardium 2. Many of the novel features of these cells suggest that they would behave in a similar manner to pacemaking cells of the cardiac conduction axis of the heart 3. Certain features of the cells suggest that if they were indeed able to generate spontaneous pacemaking activity, that they would depend on the ‘Ca2+ clock’ mechanism of pacemaking preferentially over the ‘membrane clock’ • • This may help to explain why the RVOT is a ‘hot‐bed’ of cardiac arrhythmias Further immunohistochemical characterisation of these cells is underway, and we also plan to attempt functional studies of these cells following their isolation, in terms of perforated patch clamping