Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
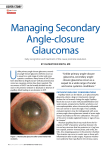
Management of a patient with acute angle closure glaucoma: Part 1 - Assessment and medical/surgical treatment Agnes Lee MPhil, Bsc (Hons), PGCE, DipN, RN, RM, OND ABSTRACT This is a two-part case study that discusses the care and management of a patient with acute angle closure glaucoma. The first part of this article provides the background to the case study. It examines the normal and abnormal anatomy and physiology of acute angle closure glaucoma and takes into account the presenting signs and symptoms. Findings from the slit lamp examination will provide a framework for discussion. An individualised medical plan of care for acute angle closure glaucoma will be discussed based on research evidence. The second part of the article examines the nursing care of the patient. The Roper-Logan-Tierney model of nursing is utilised to provide a framework for the assessment, planning, implementing and evaluation of the patient (Roper et al 1996). The case study will also explore the patient's beliefs about his illness and issues of adherence. The role of the glaucoma nurse in the management of patients with glaucoma will also be discussed. Key words: Acute glaucoma, individualised care management, advanced nursing practice. Journal of ESONT 2006; 1(2): 10-15 © 2006 ESONT Summary of case study Summary Mr J is a 67 year old hypermetropic gentleman who was referred by his GP with a three day history of an acute, painful left eye and blurring of vision. A diagnosis of left acute angle closure glaucoma was made. An individualised medical plan was put into action. Immediate medical treatment of a stat dose of intravenous and oral acetazolamide 500mgs was instigated. He was admitted and commenced on guttae prednisolone forte and pilocarpine 4% four times a day to his left eye. Due to Mr J's asthmatic status, topical betablockers were avoided and guttae Iopidine prescribed instead. The next day, the IOP in his left eye was reduced to 10mmHg. As his left cornea was still oedematous, he underwent an uneventful right YAG peripheral iridotomy before he was discharged. He attended as an outpatient two days later to undergo a left YAG peripheral iridotomy. His discharge topical medications included prednisolone four times a day to both eyes, Iopidine and pilcocarpine three times a day to his left eye only. He was also prescribed acetazolamide tablets 250mgs three times a day for three days. Mr J's nursing care on the ward was based on the RoperLogan-Tierney model for nursing (Roper et al 1996). Since the pivotal concept of the model is described in the Activities of Living, this provides the framework for the assessment, planning, implementing and evaluation of Mr J's care. Mr J was subsequently discharged five months later with no adverse damage to his eyes. 10 Journal of ESONT Volume 1 Issue 2 INTRODUCTION Mr J is a 67 year old hypermetropic gentleman who was referred by his general practitioner (GP) with a three day history of an acute, painful left eye and blurring of vision. A provisional diagnosis of an acute anterior iritis associated with a history of cervical spondylitis was made by his GP. At the hospital, his corrected vision was 6/5 in his right eye and 6/12 in his left eye. Slit lamp examination showed bilateral shallow anterior chambers and his intraocular pressure in his right and left eye was 17mmHg and 65mmHg respectively. His left pupil was dilated and unreactive with a mild anterior chamber reaction. His medical history included angina, hypertension, hypercholestremia, cervical spondylitis and asthma. His medications included verapamil 120mgs, atavastin 10mgs, soluble aspirin 75mgs and Beclaforte and salbutamol inhalers. He was also possibly allergic to tetracycline. When Mr J’s assessment was complete, he was diagnosed with having acute angle closure glaucoma. ANATOMY AND PATHOPHYSIOLOGY OF ACUTE ANGLE CLOSURE GLAUCOMA Angle closure glaucoma is a condition in which the iris is apposed to the trabecular meshwork at the angle of the anterior chamber of the eye. Angle closure may occur via two mechanisms. The iris may be pushed forward into contact with the trabecular meshwork, as in pupillary block or plateau iris, or it may be pulled anteriorly as occurs with other inflammatory conditions such as acute anterior uveitis. Approximately 90% of patients with angle closure glaucoma have relative block as the underlying mechanisms (Ritch 2001). The remaining 10% have another mechanism or combination of mechanisms other than, or in addition to, pupillary block. © 2006 ESONT