Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
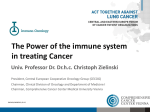
Special Report Temporal Trends in Demographics and Overall Survival of Non–Small-Cell Lung Cancer Patients at Moffitt Cancer Center From 1986 to 2008 Matthew B. Schabath, PhD, Zachary J. Thompson, PhD, and Jhanelle E. Gray, MD Background: An assessment of historical trends in patient survival is important to determine the progress toward patient outcomes and to reveal where advancements must be made. The goal of this study was to assess changes in demographics and overall survival of non–small-cell lung cancer (NSCLC) patients who were seen at Moffitt Cancer Center spanning 22 years. Methods: This analysis included 4,997 NSCLC patients who were treated at our institute over 5 time periods: 1986 to 1988, 1991 to 1993, 1996 to 1998, 2001 to 2003, and 2006 to 2008. Kaplan-Meier survival curves and the log-rank statistic were used to assess changes in 5-year survival rates over the 5 time periods, and multivariable hazard ratios were estimated from Cox proportional hazards models. Results: From 1986 to 2008 we observed statistically significant increases in the percentage of patients over the age of 70 years, women, never-smokers and former smokers, and patients with stage I tumors. Over the same time period the median survival time statistically significantly increased from 1.09 years (95% confidence interval [CI], 0.95–1.34, P < .001) to 2.27 years (95% CI, 2.07–2.46, P < .001), and the overall 5-year survival rate for all patients significantly increased from 14.7% to 31.1% (P < .001). Among stage I patients, the 5-year survival rate increased from 31.7% to 54.0% (P < .001), 13.3% to 36.0% for stage II (P < .001), 10.5% to 21.7% for stage III (P < .001), and 3.4% to 9.6% for stage IV (P < .001). Conclusions: This analysis demonstrated important temporal changes in the demographics and improvements in overall survival of NSCLC patients treated at our institute from 1986 to 2008. The 5-year survival rates and median survival time of patients diagnosed with NSCLC has significantly improved across all stages, including patients with late-stage disease. Introduction In the United States, lung cancer is the second most common cancer in men after prostate cancer and the second most common cancer in women after breast cancer. In 2013 an estimated 228,190 new cases of lung cancer were diagnosed in the United States, accounting for about 14% of all cancer diagnoses.1 The incidence rate has been declining in men over the past 2 decades, but in women the incidence rate has just recently started to decrease. Lung cancer is the leading cause of cancer-related death among both men and women in the United States, and it accounts for more deaths than any other cancer in both sexes. In 2013 approximately 159,480 deaths occurred, or From the Departments of Cancer Epidemiology (MBS) and Biostatistics (ZJT) and the Thoracic Oncology Program (JEG) at the H. Lee Moffitt Cancer Center & Research Institute, Tampa, Florida. Submitted August 26, 2013; accepted August 26, 2013. Address correspondence to Matthew B. Schabath, PhD. Department of Cancer Epidemiology, Moffitt Cancer Center, 12902 Magnolia Drive, MRC-CANCONT, Tampa, FL 33612. E-mail: Matthew. [email protected] No significant relationship exists between the authors and the companies/organizations whose products or services may be referenced in this article. January 2014, Vol. 21, No. 1 about 27% of all cancer deaths. Lung cancer causes more deaths annually than prostate, breast, colon, and pancreatic cancers combined.1 Non–small-cell lung cancer (NSCLC) represents more than 80% of lung cancer diagnoses and has an overall 5-year survival rate of approximately 16%, which decreases precipitously among patients diagnosed with latestage disease.2,3 An assessment of historical trends in patient survival is an important evaluation to determine the progress toward patient outcomes and reveal where advancements must be made. To date, few studies have evaluated survival trends over time in patients with lung cancer. The goal of this study was to assess changes in demographics and overall survival of NSCLC patients across 5 time periods spanning 22 years who were seen at Moffitt Cancer Center (MCC). Material and Methods Study Population This analysis included 4,997 NSCLC patients who were treated at our institute between 1986 and 2008. The 5 periods that were selected for analysis were 1986 to 1988, 1991 to 1993, 1996 to 1998, 2001 to 2003, Cancer Control 51 and 2006 to 2008. These time period ranges were selected to compare changes in demographics and overall survival within and across decades. Each study period included 3 years of patient data with a 2- to 3-year interval in between. This research was approved by the University of South Florida Institutional Review Board. Cancer Registry Data The primary source of data for this analysis was MCC’s Cancer Registry, which abstracts information from patient electronic medical records on demographics, history of smoking, stage, histology, and treatment. Patients seen for second opinions are not included in the Cancer Registry database because they do not fall under current Table 1. — Demographic and Clinical Characteristics of the NSCLC Patients (N = 4,997) for 5 Time Periods Characteristic Age, n (%) < 50 yrs 50 to 59 yrs 60 to 69 yrs ≥ 70 yrs Sex, n (%) Male Female Smoking Status, n (%) Never Former Current Race, n (%) White Black Other or unknown Ethnicity, n (%) Non-Spanish Spanish Unknown 1986 to 1988 (n = 207) 1991 to 1993 (n = 379) 1996 to 1998 (n = 792) 2001 to 2003 (n = 1,669) 2006 to 2008 (n = 1,950) P Valueb < .001 24 52 90 41 (11.6) (25.1) (43.5) (19.8) 42 66 166 105 (11.1) (17.4) (43.8) (27.7) 74 133 281 304 (9.3) (16.8) (35.5) (38.4) 165 361 556 587 (9.9) (21.6) (33.3) (35.2) 165 376 660 748 (8.5) (19.3) (33.9) (38.4) < .001 133 (64.3) 74 (35.7) 212 (55.9) 167 (44.1) 422 (53.3) 370 (46.7) 896 (53.7) 773 (46.3) 957 (49.1) 993 (50.9) 11 (5.3) 84 (40.6) 99 (47.8) 31 (8.2) 167 (44.1) 172 (45.4) 51 (6.4) 439 (55.4) 292 (36.9) 111 (6.7) 856 (51.3) 586 (35.1) 140 (7.2) 1006 (51.6) 551 (28.3) < .001 .008c 203 (98.1) 4 (1.9) 0 (0) 367 (96.8) 10 (2.6) 2 (0.5) 771 (97.3) 14 (1.8) 7 (0.9) 1605 (96.2) 49 (2.9) 15 (0.9) 1817 (93.2) 81 (4.2) 52 (2.7) .025d 203 (98.1) 4 (1.9) 0 (0) 375 (98.9) 4 (1.1) 0 (0) 776 (98) 15 (1.9) 1 (0.1) 1612 (96.6) 50 (3) 7 (0.4) 1856 (95.2) 68 (3.5) 26 (1.3) Histology, n (%) Adenocarcinoma Squamous cell carcinoma Other NSCLC 89 (43.0) 76 (36.7) 42 (20.3) 167 (44.1) 139 (36.7) 73 (19.3) 382 (48.2) 225 (28.4) 185 (23.4) 697 (41.8) 431 (25.8) 541 (32.4) 751 (38.5) 389 (19.9) 810 (41.5) Stage, n (%) I II III IV N/A 41 15 77 61 13 (19.8) (7.2) (37.2) (29.5) (6.3) 79 40 136 100 24 (20.8) (10.6) (35.9) (26.4) (6.3) 223 56 268 211 34 (28.2) (7.1) (33.8) (26.6) (4.3) 419 161 450 495 144 (25.1) (9.6) (27) (29.7) (8.6) 532 135 446 521 316 (27.3) (6.9) (22.9) (26.7) (16.2) First Course of Treatment, n (%)a Combination Surgery Chemotherapy Radiation None N/A 56 55 12 62 22 0 (27.1) (26.6) (5.8) (30) (10.6) (0) 102 112 30 115 20 0 (26.9) (29.6) (7.9) (30.3) (5.3) (0) 324 241 117 67 42 1 (40.9) (30.4) (14.8) (8.5) (5.3) (0.1) 706 485 207 110 102 59 (42.3) (29.1) (12.4) (6.6) (6.1) (3.5) 691 461 228 129 105 336 (35.4) (23.6) (11.7) (6.6) (5.4) (17.2) < .001 < .001e < .001e N/A = not available. NSCLC = Non–small-cell lung cancer. P values in bold font indicate a statistically significant difference across the 5 time periods. Because of missing data or rounding, percentages may not total 100. a First course of treatment includes all methods of treatment recorded in the treatment plan and administered to the patient before disease progression or recurrence. Combination is treatment with 2 or more of surgery, chemotherapy, of radiation. b P values calculated from Pearson’s chi-square to test for differences across the 5 time periods. c Excludes “Other or unknown” group. d Excludes “Unknown” group. e Excludes “N/A” group. 52 Cancer Control January 2014, Vol. 21, No. 1 Table 2. — Median Survival Time and 5-Year Survival Rate for 5 Time Periods Median survival time, yrs (95% CI)a 1986 to 1988 (N = 207) 1991 to 1993 (N = 379) 1996 to 1998 (N = 791) 2001 to 2003 (N = 1,668) 2006 to 2008 (N= 1,806) P Valueb 1.09 (0.95–1.34) 1.20 (1.07–1.49) 1.71 (1.53–1.93) 1.82 (1.66–2.01) 2.27 (2.07–2.46) < .001 14.7 14.2 21.1 26.5 31.1 < .001 31.7 13.3 10.5 3.4 36.7 22.5 5.5 3.0 48.0 30.4 11.6 3.8 54.3 35.3 15.0 6.3 54.0 36.0 21.7 9.6 < .001 < .001 < .001 < .001 5-year survival rate, % Overall By stage I II III IV CI = confidence interval. P values in bold font indicate a statistically significant difference across the 5 time periods. a Median survival time was calculated from the Kaplan-Meier survival curves. b P values calculated from the log-rank test. reportable state and/or federal guidelines. Follow-up for survival and vital status information occurs annually through passive and active methods. The Cancer Registry defines “first course of treatment” as all methods of treatment recorded in the treatment plan and administered to the patient before disease progression or recurrence or death. For this analysis smoking status was categorized as self-reported current smoker, former smoker, or never-smoker. Where available, pathological TNM staging was utilized, and if these data were missing, we utilized clinical stage information. (P < .001), the percentage of squamous cell carcinoma decreased from 36.7% to 19.9% (P < .001), and the percentage of stage I patients increased 19.8% to 27.3% (P < .001). Although the percentage of surgeries remained relatively constant for the first course of treatment (26.6% to 23.6%), the actual number of surgical patients increased from 55 in the 1986 to 1988 time period to 461 in the 2006 to 2008 time period. Furthermore, combination first course of treatment, which would include surgical patients who received adjuvant chemotherapy, increased significantly (27.1% to 35.4%, P < .001). Complete follow-up data were not available on all patients. The number of patients with complete follow-up data per time period is noted in Table 2 and Fig 1. From 1986 to 2008 among all NSCLC patients, the median survival time statistically significantly increased (P < .001) from 1.09 years (95% CI, 0.95–1.34) to 2.27 years (95% CI, 2.07–2.46), and the overall 5-year survival rate significantly increased January 2014, Vol. 21, No. 1 0.8 0.6 0.4 Survival Probability 0.2 For this analysis, 4,997 NSCLC patients were available across the 5 time periods: 1986 to 1988 (n = 207), 1991 to 1993 (n = 379), 1996 to 1998 (n = 792), 2001 to 2003 (n = 1,669), and 2006 to 2008 (n = 1,950). The demographics and 5-year survival data across the 5 time periods are presented in Table 1. From 1986 to 2008, the percentage of patients who were diagnosed over the age of 70 years increased from 19.8% to 38.4% (P < .001), the percentage of women increased from 35.7% to 50.9% (P < .001), the percentage of current smokers decreased from 47.8% to 28.3% Log Rank P value < .001 1986 to 1988 (N = 207) 1991 to 1993 (N = 379) 1996 to 1998 (N = 791) 2001 to 2003 (N = 1,668) 2006 to 2008 (N = 1,806) 0.0 Results 1.0 Statistical Analysis Pearson’s chi-square was used to test for differences in the patient characteristics across the 5 time groups. Overall survival was right-censored at 5 years, and survival analyses were performed using Kaplan-Meier survival curves and the log-rank statistic. Multivariable Cox proportional hazard regression was utilized to generate hazard ratio (HR) and 95% confidence interval (CI) for each time period. All statistical analyses were performed using R version 2.14 (R Project for Statistical Computing, www.rproject.org). 0 1 2 3 4 5 Years Fig 1. — Kaplan-Meier survival curves for overall survival of non–small-cell lung cancer patients by time period. Cancer Control 53 Log Rank P value < .001 0.2 0.4 0.6 0.8 1986 to 1988 (N = 56) 1991 to 1993 (N = 119) 1996 to 1998 (N = 279) 2001 to 2003 (N = 580) 2006 to 2008 (N = 667) 0.0 Survival Probability 1.0 (P < .001) from 14.7% to 31.1% (Table 2). Although there was no substantial difference in the overall 5-year rate for the first 2 time periods (14.7% for 1986 to 1988 vs 14.2% for 1991 to 1993), the 5-year Kaplan-Meier survival curves (Fig 1) demonstrated statistically significantly improved survival across the 5 time periods (P < .001). When the data were strati- 0 1 2 A 3 4 1.0 Log Rank P value < .001 0.4 0.6 0.8 1986 to 1988 (N = 77) 1991 to 1993 (N = 136) 1996 to 1998 (N = 268) 2001 to 2003 (N = 449) 2006 to 2008 (N = 446) 0.2 Survival Probability 5 Years fied by stage, we observed increases in the 5-year survival rates for each stage. The 5-year survival rate increased from 31.7% to 54.0% for stage I patients (P < .001), 13.3% to 36.0% for stage II (P < .001), 10.5% to 21.7% for stage III (P < .001), and 3.4% to 9.6% for stage IV (P < .001). The 5-year survival rates for the 2 most recent time periods were nearly the same for stage I (54.3% for 2001 to 2003 vs 54.0% for 2006 to 2008) and stage II patients (35.3% for 2001 to 2003 vs 36.0% for 2006 to 2008). As noted in Fig 2A, when stage I and II patients were combined, the 5-year survival curves demonstrated statistically significantly improved survival across the 5 time periods (P < .001). Similarly, 5-year survival curves demonstrated statistically significantly improved survival across the 5 time periods for stage III (Fig 2B, P < .001) and stage IV (Fig 2C, P < .001) patients. Table 3 presents the multivariable hazard ratio (mHR) models for all covariates for each time period. Across the 5 time periods, an increased risk of death was generally observed for patients older than 70 years of age, men, and current smokers. Patients treated with radiation were generally associated with an elevated risk of death across the 5 time periods, and increasing stage for each of the time periods was associated with an incremental increased risk of death. For example, in the 2006 to 2008 time period, the mHR was 1.81 (95% CI, 1.36–2.41) for stage II patients, 2.72 (95% CI, 2.19–3.38) for stage III patients, and 5.17 (95% CI, 4.15–6.45) for stage IV patients. 0.0 Discussion 0 1 2 B 3 5 1.0 0.2 0.4 0.6 0.8 Log Rank P value < .001 1986 to 1988 (N = 61) 1991 to 1993 (N = 100) 1996 to 1998 (N = 210) 2001 to 2003 (N = 495) 2006 to 2008 (N = 521) 0.0 Survival Probability 4 Years 0 C 1 2 3 4 5 Years Fig 2A-C. — Stage-specific Kaplan-Meier survival curves for overall survival of non–small-cell lung cancer patients by time period: (A) Kaplan-Meier survival curve for stages I and II lung cancer, (B) Kaplan-Meier survival curve for stage III lung cancer, and (C) Kaplan-Meier survival curve for stage IV lung cancer. 54 Cancer Control This analysis of Cancer Registry data from 5 time periods of lung cancer patients at our institute demonstrates statistically significant changes in demographics and survival of NSCLC patients over the past 22 years. Most importantly, from 1986 to 2008, the overall median survival time and overall 5-year survival rate have both more than doubled. Additionally, we observed statistically significant increases in stage-specific 5-year survival rates over the 5 time periods. The most recent Surveillance, Epidemiology, and End Results (SEER) monograph on lung cancer, published in 2007, reported overall and stagespecific survival rates based on patients diagnosed between 1998 to 2001 from 12 SEER areas.4 Since none of the 5 time periods in our study completely overlapped with the time period in the SEER study, we explored the 1998 to 2001 time period in our data so we could make comparisons. The overall 5-year survival for SEER was 15.5% vs 25.0% in our data, and the stage-specific rates in the SEER study vs our study were 56.9% vs 52.4% for stage I, January 2014, Vol. 21, No. 1 33.7% vs 33.6% for stage II, 9.4% vs 14.9% for stage III, and 9.4% vs 3.9% for stage IV. Thus, the SEER results are comparable with the rates found in our analysis, especially among stage I, II, and III patients. Other studies have also analyzed the temporal changes in lung cancer survival, but our study is by far the largest from a single institution. An analysis performed at the University of Texas MD Anderson Cancer Center5 over 3 study periods (1985 to 1989, 1993 to 1997, and 2000 to 2004) found that the overall median survival duration increased from 12.0 months in 1985 to 1989 to 17.5 months in 2000 to 2004. Additionally, that study reported that the probability of survival of patients who were alive at 2 years after diagnosis increased from 26.5% in 1985 to 1989 to 40.8% in 2000 to 2004. A Japanese study6 compared the survival of lung cancer patients who were detected by screening conducted between 1976 and 1984 with patients who were detected by screening between 1989 and 1997 and reported an increase in both median survival time of 27.8 months to 49.8 months and an increase in 5-year survival from 34.8% to 47.8% (P < .01). Two studies in Canada used national databases to assess temporal changes in cancer survival rates. A recent study by Kachuri et al7 assessed temporal changes across 4 time periods (1992 to 1994, 1996 to 1998, 2000 to 2002, and 2005 to 2007) and Table 3. — Multivariable Cox Proportional Hazard Models for 5 Time Periods 1986 to 1988 mHR (95% CI) 1991 to 1993 mHR (95% CI) 1996 to 1998 mHR (95% CI) 2001 to 2003 mHR (95% CI) 2006 to 2008 mHR (95% CI) Age (yrs) < 50 50 to 59 60 to 69 ≥ 70 1.00 (referent) 0.83 (0.47–1.47) 1.06 (0.62–1.80) 1.74 (0.94–3.24) 1.00 (referent) 1.24 (0.75–2.03) 1.28 (0.84–1.96) 1.85 (1.17–2.91) 1.00 (referent) 1.29 (0.92–1.83) 1.34 (0.97–1.84) 1.73 (1.25–2.41) 1.00 (referent) 1.00 (0.79–1.25) 0.95 (0.77–1.19) 1.28 (1.02–1.60) 1.00 (referent) 0.93 (0.72–1.20) 1.03 (0.81–1.32) 1.16 (0.90–1.48) Sex Female Male 1.00 (referent) 1.21 (0.84–1.73) 1.00 (referent) 1.58 (1.23– 2.03) 1.00 (referent) 1.42 (1.19–1.68) 1.00 (referent) 1.39 (1.23–1.58) 1.00 (referent) 1.24 (1.09–1.41) Smoking Status Never Former Current 1.00 (referent) 1.04 (0.47–2.31) 0.96 (0.44–2.10) 1.00 (referent) 1.10 (0.69–1.74) 1.16 (0.74–1.83) 1.00 (referent) 1.03 (0.72–1.47) 1.38 (0.96–1.98) 1.00 (referent) 1.14 (0.89–1.47) 1.34 (1.03–1.74) 1.00 (referent) 1.39 (1.08–1.79) 1.72 (1.32–2.25) Race White Black Other or unknown 1.00 (referent) 2.92 (0.85–9.97) N/A 1.00 (referent) 2.41 (1.20–4.88) 2.87 (0.67–12.31) 1.00 (referent) 0.60 (0.29–1.24) 1.51 (0.69–3.28) 1.00 (referent) 1.21 (0.83–1.76) 1.87 (0.99–3.53) 1.00 (referent) 1.52 (1.14–2.02) 0.76 (0.48–1.19) Ethnicity Non-Spanish Spanish Unknown 1.00 (referent) 0.33 (.07–1.56) N/A 1.00 (referent) 1.58 (0.48–5.17) N/A 1.00 (referent) 0.84 (0.45–1.59) 0.88 (0.12–6.56) 1.00 (referent) 0.90 (0.64–1.25) 1.41 (0.58–3.43) 1.00 (referent) 1.19 (0.86–1.65) 2.14 (1.14–4.04) Histology Adenocarcinoma Squamous cell carcinoma Other NSCLC 1.00 (referent) 0.79 (0.54–1.17) 0.98 (0.62–1.57) 1.00 (referent) 0.85 (0.63–1.13) 1.01 (0.73–1.40) 1.00 (referent) 0.93 (0.76–1.14) 0.96 (0.77–1.20) 1.00 (referent) 0.92 (0.79–1.08) 0.88 (0.77–1.02) 1.00 (referent) 1.10 (0.92–1.31) 0.92 (0.80–1.07) First Course of Treatmenta Combination Surgery Chemotherapy Radiation 1.00 (referent) 0.37 (0.19–0.72) 0.71 (0.34–1.47) 1.37 (0.90–2.09) 1.00 (referent) 0.86 (0.57–1.29) 1.30 (0.82–2.05) 1.51 (1.10–2.06) 1.00 (referent) 0.88 (0.67–1.17) 1.41 (1.09–1.82) 2.45 (1.82–3.31) 1.00 (referent) 0.70 (0.57–0.85) 1.40 (1.17–1.67) 2.52 (1.98–3.20) 1.00 (referent) 0.86 (0.70–1.07) 1.19 (0.99–1.42) 2.59 (2.03–3.29) Stage I II III IV 1.00 (referent) 1.06 (0.48–2.34) 1.01 (0.52–1.95) 1.87 (0.96–3.64) 1.00 (referent) 1.40 (0.86–2.26) 2.76 (1.79–4.24) 5.40 (3.28–8.89) 1.00 (referent) 1.55 (1.04–2.33) 3.33 (2.49–4.46) 5.26 (3.83–7.23) 1.00 (referent) 1.40 (1.08–1.82) 2.38 (1.92–2.96) 4.30 (3.46–5.36) 1.00 (referent) 1.81 (1.36–2.41) 2.72 (2.19–3.38) 5.17 (4.15–6.45) CI = confidence interval, N/A = not available, NSCLC = non–small-cell lung cancer, mHR = multivariable hazard ratio. Bold font indicates a statistically significant hazard ratio. a First course of treatment includes all methods of treatment recorded in the treatment plan and administered to the patient before disease progression or recurrence. January 2014, Vol. 21, No. 1 Cancer Control 55 found only a 2.6% absolute difference in the 5-year age-standardized relative survival ratios for all lung cancers combined. An earlier study conducted in Canada8 analyzed survival trends across 5 time periods (1969 to 1973, 1974 to 1978, 1979 to 1983, 1984 to 1988, and 1989 to 1991) and found no significant differences across the study periods. Unfortunately, neither Canadian study presented stage-specific results and combined all lung cancers together rather than focusing on specific histological subtypes. The multivariable models in the present analysis revealed that older patients, men, current smokers, and late-stage patients were associated with an increased risk of death. The findings for age, sex, and smoking status have been reported in previous studies,3-5 and tumor stage is a well-documented prognostic and predictive factor for NSCLC.9-11 First course of treatment with radiation was also associated with an increased risk of death. Kachroo et al8 reported a similar finding for radiation therapy where patients treated with radiation only were associated with a 3.9-fold (95% CI, 1.12–13.33) increased risk of death. Lung cancer patients who receive radiotherapy typically have more advanced disease (eg, postoperative stage IIIA, unresectable stage IIIA/B, stage IV). Additionally, some early-stage lung cancer patients are also referred for radiotherapy if they have poor performance status and are not surgical candidates. Thus, the increased risk of death among patients who receive radiotherapy likely reflects the poor performance status and inherent poor prognosis of the patients rather than the treatment itself. We also observed that surgery-only patients were generally associated with a reduced risk of death. This finding is not unexpected since surgery is the typical treatment for early-stage NSCLC patients with good performance status. A few limitations must be acknowledged about this study. First, we acknowledge the possible lack of generalizability of our study population because the lung cancer patients in this analysis were derived from a single cancer care center and were composed of mostly non–Hispanic whites. Hence, the results may not be generalizable to community practices or even to other cancer centers. However, we must consider that lung cancer patients at a tertiary cancer center like MCC could represent more complex cases, and thus our 5-year survival rates could be conservative. This is speculation since we do not have demographic and 5-year survival data for regional practices. Additionally, our analysis was limited to Cancer Registry data, which does not include a comprehensive and systematic assessment of lung cancer risk factors such as detailed smoking history, family history of cancer, occupational exposures, and medical history. The data abstracted by Cancer Registry are limited to information that is available in patient medical records. 56 Cancer Control Conclusions This analysis demonstrated important temporal changes in the demographics and improvements in overall survival of non–small-cell lung cancer patients treated at Moffitt Cancer Center from 1986 to 2008. The 5-year survival rates and median survival times of patients diagnosed with non–small-cell lung cancer have significantly improved across all stages, including late-stage disease. The observed improvement in lung cancer survival over the last 22 years is likely attributed to several factors including advancements in surgery, chemotherapy regimens, management of comorbidities, and a slightly higher percentage of early-stage patients who are more amendable to treatment. Further study is required to assess potential temporal changes in targeted molecular-based therapies, advancements in surgical procedures, and patients enrolled into chemotherapy trials. This work was supported was by a National Institutes of Health/National Cancer Institutive (NIH/NCI) Specialized Program of Research Excellence (SPORE) Grant (P50 CA119997) and an NIH/NCI American Recovery and Reinvestment Act (ARRA) Grant (5 UC2 CA 148322-02). For contributions in data collection, curation, management, and access, appreciation is expressed to the Moffitt Cancer Registry (Director: Karen A. Coyne), Edward T. Chwieseni, Research Information Technology (IT), and the Data Management and Integration Technology (DMIT) group. References 1. American Cancer Society. Cancer Facts & Figures 2013. Atlanta, GA: American Cancer Society; 2013. 2. McErlean A, Ginsberg MS. Epidemiology of lung cancer. Semin Roentgenol. 2011;46(3):173-177. 3. Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32(4):605-644. 4. Ries LAG, Young JL, Keel GE, et al, eds. SEER Survival Monograph: Cancer Survival Among Adults. US SEER Program, 1988-2001, Patient and Tumor Characteristics. Bethesda, MD: National Cancer Institute, SEER Program; 2007. NIH Pub. No. 07-6215. 5. Kachroo S, Tong L, Spitz MR, et al. Trends in prevalence of prognostic factors and survival in lung cancer patients from 1985 to 2004 at a tertiary care center. Cancer Detect Prev. 2008;32(2):101-108. 6. Kitajima T, Nishii K, Ueoka H, et al. Recent improvement in lung cancer screening: a comparison of the results carried out in two different time periods. Acta Med Okayama. 2006;60(3):173-179. 7. Kachuri L, De P, Ellison LF, et al. Cancer incidence, mortality and survival trends in Canada, 1970-2007. Chronic Dis Inj Can. 2013;33(2):69-80. 8. Ugnat AM, Xie L, Semenciw R, et al. Survival patterns for the top four cancers in Canada: the effects of age, region and period. Eur J Cancer Prev. 2005;14(2):91-100. 9. Mirsadraee S, Oswal D, Alizadeh Y, et al. The 7th lung cancer TNM classification and staging system: review of the changes and implications. World J Radiol. 2012;4(4):128-134. 10. Chansky K, Sculier JP, Crowley JJ, et al. The International Association for the Study of Lung Cancer Staging Project: prognostic factors and pathologic TNM stage in surgically managed non-small cell lung cancer. J Thorac Oncol. 2009;4(7):792-801. 11. Bergman P, Brodin D, Lewensohn R, et al. Validation of the 7th TNM classification for non-small cell lung cancer: a retrospective analysis on prognostic implications for operated node-negative cases. Acta Oncol. 2013;52(6):1189-1194. January 2014, Vol. 21, No. 1