Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
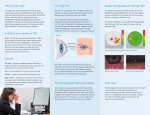
40 j u n e 2 0 1 4 A Quick Guide to Dry Eye j a s o n c a l h o u n , o p h t h a l m i c p h o t o g r a p h e r , d e p a r t m e n t o f o p h t h a l m o l o g y, m ay o c l i n i c j a c k s o n v i l l e Dry eye may not blind your patients, but moderate or severe disease is making some of them miserable. Spot and treat this overlooked condition in its early stages, and make a difference for your patients. A s a cornea fellow some 30 years ago, Robert S. Feder, MD, was shown a cartoon of an elf holding a watering can. “That was the model for treating dry eye disease. Water the cornea,” said Dr. Feder, at Northwestern University in Chicago. Fifteen years later, not much had changed. “Doctors said, ‘Take these tears and go home,” said Giacomina Massaro-Giordano, MD, now at Penn Dry Eye and Ocular Surface Center, Philadelphia. “Dry eye was ignored.” Or, worse, these patients were dismissed as crazy. Indeed, this was the case with Dr. Massaro-Giordano’s mother when she complained about her eyes. But patients who say they have foreign body sensations in their eyes—or burning, dryness, or exquisite sensitivity to wind or air conditioning drafts—suffer from a very real condition. Today doctors better understand dry eye disease (DED), a multifactorial condition associated with ocular surface inflammation and tear film hyperosmolarity. There are even centers, such as Dr. Massaro-Giordano’s, dedicated to its treatment. Growing prevalence. As the population ages, doctors will be diagnosing DED with greater frequency. Though the condition is not associated exclusively with aging, its prevalence increases with every decade of life over 40. It is also associated with contact lens use, cigarette smoking, diabetes, prolonged video display viewing, and low-humidity environments. Twenty percent of the U.S. population is diagnosed with dry eye, said Dr. MassaroGiordano. Still, the disease is very underdiagnosed, Dr. Feder noted. “It is also underappreciated in that you don’t see frank pathology as you do in macular degeneration or cataract, so it may be easy to ignore,” said Penny A. Asbell, MD, FACS, at Icahn School of Medicine in New York. Unhappy patients. The more severe forms of DED have been ranked equivalent to unstable Miriam Karmel, Contributing Writer e y e n e t 41 Causes of Dry Eye The two major types of DED are aqueous tear deficiency (ATD) and evaporative dry eye. In the latter, which is linked to meibomian gland dysfunction, lipid insufficiency may result in increased evaporation and tear film instability, among other sequelae.3 It’s important to try to differentiate between the two underlying causes. In many—but not all—cases, the treatments are the same, said Robert W. Weisenthal, MD, at SUNY Upstate Medical University, Syracuse. Dr. Asbell added that some patients may have a little of both types. “The reality is that it’s pretty hard to tell. There’s no surefire test.” Still, you want to think about findings that point more toward ATD or evaporative DED because that may alter your treatment, she said. 42 j u n e 2 0 1 4 Either way, DED will progInspissated meibomian glands. ress. Chronic inflammation of the lids from meibomian gland dysfunction and evaporative dry eye, coupled with tears that contain inflammatory components, can further damage the meibomian glands, said Dr. Massaro-Giordano. Tear insufficiency dry eye, on the other hand, may point to an underlying autoimmune disorder. “Over time, that can destroy the lacrimal glands,” she said. Consider systemic conditions. A number of inflammatory autoimmune conditions can cause dry eye. One of the most important objectives of the dry eye evaluation is ruling out Sjögren syndrome, said Esen K. Akpek, MD, at Wilmer Eye Institute, Baltimore. One in 10 patients with clinically significant dry eye will have Sjögren’s, which puts the patient at risk for systemic conditions such as lymphoma and major organ involvement, including the lungs, kidneys, and liver, she said. These patients often complain of dry mouth, fatigue, and joint pain. The clinician should always inquire about these symptoms in assessing dry eye patients. Symptoms of concern. Dr. Feder said to beware of potential underlying conditions when dry eye is accompanied by the following symptoms: • Fullness and/or tenderness in the superotemporal eyelid—the area of the lacrimal gland—should trigger consideration of dacryoadenitis, either postviral or associated with inflammatory disorders such as sarcoidosis. If a conjunctival granuloma is present, it can be biopsied. • Proptosis and/or eyelid swelling may indicate thyroid disease. • Subepithelial fibrosis in the conjunctiva of an elderly patient should be evaluated for ocular mucous membrane pemphigoid, with conjunctival biopsy for immunopathology looking for antibodies to the basement membrane. Diagnose Dry Eye Because dry eye disease is hard to diagnose, “What we need is a metric that says, ‘Yes, you have it. Or don’t,’” Dr. Asbell said. Ideally, that metric also could distinguish severe from mild cases. She compared it with HIV, where a blood test confirms that you either do or don’t have the disease. It can measure viral load robert w. weisenthal, md angina in quality-of-life utility assessments.1 “You may not go blind from it, but it does affect your whole persona,” said Dr. Massaro-Giordano. Dr. Asbell added that patients who have significant dry eye “are not too happy.” It’s a chronic pain syndrome, she said. “These can be challenging patients to care for.” Frustrating for physicians. Dr. Asbell noted that DED can be challenging to diagnose. For instance, when a dry eye patient reads the chart, she may have 20/20 vision because she blinked before reading, yet she still says, “But I don’t see well,” said Dr. Asbell. She likens this to a car with a dirty windshield. Clean it off (or blink) and you can see through it. However, many of these patients are not blinking often enough to maintain good vision throughout the day. A few years ago, Dr. Asbell surveyed ophthalmologists on their perceptions about treatment of dry eye, and they reported being frustrated, saying that patients with moderate to severe DED were difficult to treat. Ophthalmologists wanted more treatment options.2 Multifactorial misery. DED is also challenging to diagnose and manage because it is multifactorial. To better handle patients with DED, the Penn Dry Eye Center, for example, has a team of experts to address the range of conditions that might be associated with DED: a rheumatologist for autoimmune disease; a dermatologist for underlying rosacea; an oculoplastic specialist for malpositioned eyelids, which can affect the tear film; an endocrinologist for the hormonal component; and a contact lens specialist. Most ophthalmologists don’t have the extensive support of a dry eye center to deal with advanced disease. But even mild DED poses challenges. What’s the best management strategy? Yes, watering the eyes with artificial tears may provide symptomatic relief. But before you reach into the sample drawer and say, “Try this tear supplement,” consider what the experts are saying about DED. Diagnostics & Tests Several diagnostic tests for dry eye are available, but expert opinion about their use is mixed. Dr. Feder pointed out that ophthalmologists are still learning about the utility of these products for everyday practice. But, he said, “if the goal of therapy is to reduce symptoms, improve function, and prevent damage, and if you can do that in the vast majority of patients for the cost of a fluorescein or Schirmer strip, you have to ask, ‘Is it worth the extra expense to buy equipment and administer a sophisticated test?’” Dr. Weisenthal noted that even though these tests quantify what you see, they don’t alter his treatment approach. Here are a few devices and tests on the market: Keratograph 5M (Oculus) and Tear Stability Analysis System (Tomey). If the tear film isn’t thick enough or doesn’t last long enough between blinks, holes appear in the tear film, causing irregularity of the surface. “These two devices assess the irregularity or regularity of the surface between blinks,” Dr. Akpek Keratograph 5M said, adding that they’re essentially topographers that can be very useful for dry eye specialists. She recommended their incorporation into LASIK and premium lens implant practices because they are topography-based and give good information on TBUT, in addition to corneal power, which affects refraction. RPS Inflammadry dectector Dr. Asbell called the Keratograph one of the promising newer devices. corneal epithelial barrier function, “That machine has a lot of potential increased corneal desquamation, for putting us in the realm of what and corneal surface irregularity. we want: minimally invasive objecHowever, the device doesn’t distintive metrics.” guish dry eye from other inflammaLipiView Ocular Surface Interfertory disorders, Dr. Akpek said. Still, ometer (TearScience). This device objective MMP measures may guide measures TBUT by taking a photo of treatment decisions. “It tells me the tear film and looking for areas of the surface is not healthy and that desiccation. the patient needs to be aggressively It’s used to diagnose evaporative treated.” The device may correlate to dry eye, Dr. Akpek said. “Whenever fluorescein punctate staining of the we see a dry eye, cornea, she said. we apply gentle Sjö (Nicox). This in-office findigital pressure ger-stick blood test, which is sent on the lid margins out to Immco labs, is designed to to get meibum check for novel antisecretion out bodies that may be of the glands. positive earlier than LIPIVIEW We look at its the traditional antiappearance. An experienced ophbody tests. Because thalmologist can distinguish good Sjö is very new, it is quality from bad quality. Although not clear whether all LipiView does not evaluate the insurance companies SJö quality of meibum, it gives good will cover it, said Dr. information about whether there Massaro-Giordano. are adequate amounts of meibum in TearLab Osmolarity System (Tearthe tear film,” she said. Lab). This device measures tear RPS InflammaDry Detector (Rapid osmolarity, which if too high may Pathogen Screening). In 10 minutes, damage the cornea and conjunctithis device delivers a reading on va. Dr. Akpek said the osmolarity levels of MMP-9 (matrix metalloprosystem would be a good addition to teinase-9), an inflammathe armamentarium. tory marker shown to be “It’s quicker and less elevated in the tears of invasive than SchirmDED patients. Increased er testing. It can be MMP-9 activity may done by a technician. contribute to deranged It is reimbursed.” tearlab over time. “There’s no equivalent for dry eye disease,” she said. But there are ways to make a diagnosis. Listen. You can get a pretty good idea by listening to the patient and taking a careful history, Dr. Asbell said. Dr. Massaro-Giordano added, “What sets some people off doesn’t set off others. It takes a lot of chair time with patients trying to figure out what makes their eyes feel better.” Dr. Weisenthal suggests that physicians ask the following questions: • Is your dry eye worst upon awakening? Or does it get worse as the day goes on? The former suggests aqueous tear deficiency; the latter, meibomian gland dysfunction. • What activities make it better or worse? • Are you using diuretics or antihistamines? (These exacerbate symptoms of dry eye and are known to make dry eye worse, said Dr. Massaro-Giordano.) e y e n e t 43 functioning. It is the first-line stain to use in evaluating the ocular surface. • Lissamine green or rose bengal staining to reveal devitalized epithelium. Use these stains to evaluate the ocular surface, not just the cornea, Dr. Weisenthal said. “If fluorescein doesn’t confirm my suspicion, I do one of these.” Dr. Akpek said you won’t see much staining in early stages of DED. By the time these stains highlight unhealthy areas of the cornea or the conjunctiva, the disease is moderate to advanced. 44 j u n e 2 0 1 4 Treatment Treatment for both mild evaporative and aqueous deficient dry eye is relatively straightforward, but it’s worth keeping a few things in mind. For evaporative dry eye, the experts recommend the following. • Warm compresses. Warm compresses and eyelid hygiene improve meibomian gland function. Moist compresses are better than dry heat, Dr. Massaro- Giordano said. Hygiene entails removing any makeup, then gently scrubbing eyelashes and eyelids with a commercially available premoistened pad. (Diluted baby shampoo or gentle face wash also works.) Apply mild pressure along the rims of the eyelids in order to express some “oil” Preservative-free glaucoma drops are from the meibomian glands. advised for dry eye Then rinse off and pat dry, she patients. said. • Manage the environment. “Recognition of the environment as a cause of dry eye can make a huge difference for the patient,” Dr. Feder said. Prolonged visual effort—reading, watching TV, computer work—reduces the blink rate, causing desiccation of the ocular surface. Other environmental causes of drying are fans, car vents, circulating airplane air, and drafts from air conditioners. Patients may improve in summer and get worse in winter. “Desktop humidifiers are becoming increasingly popular,” said Dr. Feder. He added that if the patient can’t change the environment, eye protection such as moisture chamber glasses—which have side shields to keep the eyes’ moisture in—may be helpful. • Beware of eyedrops. Preservatives in glaucoma medications can destabilize the tear film. Dr. Massaro-Giordano advises working with the glaucoma specialist for a preservative-free option. If that’s not possible, she suggests considering surgery that cour tesy of giacomina massaro-giordano, md; american academy of ophthalmology Dr. Massaro• Do you have dry mouth? Gum disease? These symptoms Giordano squeezes may be associated with system- a patient’s meibomian glands. ic disease like Sjögren’s. Look. Though tests will confirm the diagnosis, Dr. Weisenthal said he often knows the results before doing them. “You can tell by looking at the patient.” He advises checking for the following: • Rosacea in the face and eyelids. Rosacea is associated with meibomianitis and evaporative dry eye. • Look at the lids. Are they floppy? Floppy eyelid syndrome can cause symptoms of dry eye. • Red lid margins. This suggests meibomian gland dysfunction. Press on the lids. If there’s a toothpaste-like secretion or no secretion, the glands are blocked. • Watch how often the patient blinks. The norm is 12 blinks per minute. The patient who doesn’t blink for 30 seconds has a problem. • Is there an incomplete blink? This is often seen after blepharoplasty. • Malpositioned lids. Eyelids that are turned in or out may evert the lacrimal punctum. • Swelling of the conjunctiva. This may indicate conjunctivochalasis. Test. Dr. Feder said that by performing the following, “you would miss very few cases of dry eye.” • Slit-lamp exam to evaluate the tear film. “A tear meniscus on the inferior lid should be a certain thickness and the fluid should be clear. Some patients have cellular debris or mucus within that tear film that just is not healthy,” Dr. Weisenthal said. • Schirmer test with anesthetic to measure basal tear production. • Fluorescein staining to Schirmer’s test. test for tear film breakup time (TBUT), which is defined as the interval between the last complete blink and the first appearance of a dry spot or disruption in the tear film. Once in the tear film, fluorescein should stay intact for at least 10 seconds. This test provides evidence of tear film stability, which suggests how well the meibomian glands are reduces the need for glaucoma medications. • Recognize systemic medication effects. Anticholinergics, antidepressants, or oral allergy and decongestant medications designed to dry up mucous membranes all can dry the surface of the eye, Dr. Feder said. Dr. Massaro-Giordano noted that a lot of patients have itchy lids resulting from advanced anterior blepharitis. “They get an over-the-counter allergy drug, which in turn dries them out further.” For aqueous tear deficiency, the experts recommend the following. • Artificial tears. For mild cases, Dr. Weisenthal gives patients two or three samples to try. “People seem to have their favorite.” The experts agreed that anyone using tear supplements more than four times a day should use preservative-free varieties. • Anti-inflammatory agents. For moderate to severe cases of dry eye, a mild topical steroid may help. Dr. Weisenthal starts with steroids four times a day for two weeks and tapers to twice a day for two weeks. No more than two to four weeks of treatment is recommended, Dr. Weisenthal warned. Topical cyclosporine (Restasis) has anti-inflammatory properties without the side effects associated with steroids. But it can take time for increased tear production to kick in. For immediate relief, Dr. Weisenthal prescribes a steroid (as above) for four weeks. By then the cyclosporine kicks in, and he stops the steroids. Restasis benefits many, but not all, patients. “It’s not particularly helpful for evaporative dry eye,” Dr. Feder said. “Its greatest utility is for patients with connective tissue disease who have inflammation of the lacrimal glands.” • Punctal plugs. For moderate to severe cases of dry eye, Dr. Feder prefers punctal plugs to cautery because they’re reversible. But in cases of severe dry eye associated with a chronic systemic disease, such as rheumatoid arthritis, he’ll consider cautery. “If you’re going to use punctal plugs, put in the largest plug possible because it’s more likely to stay in.” Dr. Weisenthal considers plugs as an alternative to long-term Restasis for patients with ATD. He warned that using plugs in cases of meibomian gland dysfunction will sometimes make the condition worse. • Omega-3. When she heard reports that omega-3 Silicone punctal plug. “works great” for dry eye disease, Dr. Asbell went to the literature. The data were limited to a few small trials, all using different types and amounts of omega-3s and different endpoints, she said. “We needed a real trial.” That trial is now under way. DREAM (Dry Eye Evaluation and Management) is the first clinical trial for dry eye funded by the NEI. Six hundred patients at 21 sites across the United States will be randomized into two groups to determine whether oral supplementation with omega-3s is an effective treatment for dry eye disease compared with placebo. DREAM will also assess potential biomarkers for inflammation. When to refer. All of the experts agreed that some cases require specialized care. Dr. Massaro-Giordano recommended referral to an academic center with an interest in DED or to a doctor who deals in surface rober t w. weisenthal, md PEARLS from the experts Academy guidelines. “Review the Academy’s Dry Eye Syndrome Preferred Practice Patterns. The evidence-based information has been carefully reviewed by a panel of experts. It’s a great resource. It’s easily accessible. And it’s free.” —Dr. Feder Find the guidelines at www.aao.org/ppp and scroll to Dry Eye Syndrome PPP - 2013. Artificial tears. “Not all artificial tears are the same. They have different consistencies. Although there can be some trial and error, it’s worth taking a look at some of the newer artificial tears. Some drops are geared more toward lipid abnormality, others toward mild lubrication. And some are more long-lasting.” —Dr. Asbell Examining the eyelids. “Look at those lids! Put pressure up against the eyelid with a fingertip or cotton swab. See what’s coming out. Is it granular? Opaque? If it’s tough to get out, you know you have a problem.” —Dr. Massaro-Giordano Patient expectations. “Dry eye is not something you can treat for two months and it will go away. It can be controlled, but it’s not something that disappears. So it’s important to set up expectations so the patient understands this is something they need to pay attention to and will have to continue to manage.” —Dr. Weisenthal Sjögren syndrome. “One main objective in seeing any dry eye patient is to ask: Is this the 1 in 10 that has Sjögren’s? Dry eye doesn’t kill anyone, but Sjögren’s can.” —Dr. Akpek e y e n e t 45 disease. Because of the multifactorial nature of the disease, a team approach can be very helpful. Bottom line. Our understanding of DED has advanced since the days of the watering can. Now it’s up to the ophthalmologist to apply what’s been learned. Success with these patients, said Dr. Feder, “really starts with your curiosity, a careful evaluation, and then going beyond treating all dry eye symptoms the same way.” n 1 Schiffman RM et al. Ophthalmology. 2003;110(7):1412-1419. 2 Asbell PA, Spiegel S. Eye Contact Lens. 2010;36(1):33-38. 3 Nichols KK et al. Invest Ophthalmol Vis Sci. 2011;52(4):19221929. MEET THE EXPERTS Esen K. Akpek, MD Professor of ophthalmology and rheumatology and director of the Ocular Surface and Dry Eye Disease Clinic, Wilmer Eye Institute, Baltimore. Financial disclosure: Consults for Nicox and has an institutional research grant from Allergan. Penny A. Asbell, MD, FACS, MBA Professor of ophthalmology and director of the cornea service and refractive surgery center at Icahn School of Medicine at Mount Sinai Hospital, New York. Financial disclosure: Conducts research with Alcon and Rtech Laboratories and is funded by the NEI for the DREAM study. Robert S. Feder, MD, MBA Professor of ophthalmology and chief of cornea/external disease service at North- Comprehensive Ophthalmologist Chicago’s Northern Suburbs NorthShore University HealthSystem (NorthShore), the principal academic affiliate of the University of Chicago Pritzker School of Medicine, seeks an exceptional Comprehensive Ophthalmologist. The successful candidate for this position will be BC/BE by the ABO and have completed an Ophthalmology residency. Take advantage of this unique opportunity to: •Workinoneofthelargestmulti-specialtyophthalmology groups on the NorthShore! •Becomeamemberofan870plusphysician,multispecialty group practice that includes more than 125 office locations with over2,100affiliatedphysicians. •BepartoftheMayoClinicCareNetwork;Mayo’sonly collaboration of its kind in the Chicago region. •Enjoythefullrangeoflifestylesthatareuniquelyavailableinthe Chicagoland area. •AcademicappointmenttoTheUniversityofChicagoPritzker School of Medicine is available to qualified candidates. Qualified candidates should submit their CV to: Marian Macsai, MD, Division Head, Division of Ophthalmology by contacting: Sandra Chavez Physician Recruiter [email protected] • (847) 663-8649 www.northshore.org/physicianrecruitment western University, Feinberg School of Medicine, Chicago. Financial disclosure: None. Giacomina Massaro-Giordano, MD Associate clinical professor of ophthalmology at University of Pennsylvania Scheie Eye Institute and codirector of the Penn Dry Eye and Ocular Surface Center, Philadelphia. Financial disclosure: Commercial interest in Physicians Recommended Nutriceuticals. Robert W. Weisenthal, MD Clinical professor of ophthalmology, SUNY Upstate Medical University, Syracuse, N.Y. Financial disclosure: None. The 13th Annual Downeast Ophthalmology Symposium SEPTEMBER 19-21, 2014 Bar Harbor, Maine For further information, contact: Shirley Goggin Maine Society of Eye Physicians and Surgeons P.O. Box 190 Manchester, ME 04351 207-445-2260 [email protected] EOE: Race/Color/Religion/Sex/National Origin/Protected Veteran/Disability, VEVRRA Federal Contractor www.maineeyemds.com 46 j u n e 2 0 1 4