Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
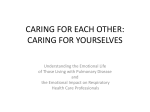
Mental Health Predictors of Pain and Function in Patients with Chronic Low Back Pain ® Olivia D. Lara, K. Ashok Kumar MD FRCS Sandra Burge, PhD The University of Texas Health Science Center at San Antonio Introduction Results Chronic low back pain is one of the most frequent reasons for visits to a physician. Between 1992 and 2006 the prevalence of chronic low back pain has risen from 3.9% to 10.2%. While the proportion of individuals who sought care at a health care provider increased to 84% in 2009 (1). Individuals with chronic low back pain place a large, costly demand on the health care system, and also account for major disability and absence from work (2). Past researchers have shown significant correlations between chronic back pain and mental health factors such as depression and anxiety (3). However few studies have investigated the impact that such mental health factors have on other aspects of health in chronic pain patients, such as physical functioning, role functioning, and general health. This study will evaluate the relationship between self-reported depression and anxiety, opioid use, pain severity, physical functioning while controlling for the causes of back pain. Materials and Methods The sample included 367 patients with an average age of 53 years. Participants were 71.9 % female, and 27.5 % were male. The most common causes of low back pain were degenerative disk (35.1%) and mechanical back pain (12.3%), with 28.9% having no diagnosis on record. Of the total participants 56.4% reported feeling depressed, 32.3% reported feeling generalized anxiety and 39.8% reported panic attacks in the previous two weeks. Based on chi-squared analysis, depression, anxiety and panic attacks were strongly associated with opioid use (Figure 1). Furthermore, mental illness symptoms were associated with physical function, role function, and general health score (p<.074, Figure 2). The specific cause of the back pain had little to do with pain or functioning outcomes. We discovered that having versus not having a diagnosis on record distinguished patients; those with a diagnosis had significantly worse pain, physical function, and role function (p<.05) Mean Scores Subjects. Student research assistants enrolled 367 adult patients from 9 outpatient clinics across Texas. Patients Linear regression analyses examined mental health were eligible if they had low back pain for 3 months or and pain diagnosis as predictors of pain, physical longer, and were excluded if they were pregnant or had function, role function, and health score. In each a diagnosis of cancer. model, mental health issues contributed significantly to pain and function outcomes. Table Procedure and Measurement. Students gathered data 1 illustrates the model addressing role function and from patient surveys and medical records. A 6-page its association with depression, anxiety and patient survey addressed demographic characteristics, diagnosis. This model shows only one outcome, pain duration, frequency and severity, physical role function, there are three other models. functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. Patients reported pain severity using a 10-point scale. To Figure 2. Association between Depression and assess depression and anxiety, investigators used 4 brief Anxiety and Functional Outcomes screening questions from PRIME-MD. Two items 3.5 Physical Function addressed depression (loss of interest and Physical Role feeling down), one addressed general anxiety, and one Health Score 3 addressed panic within the past 2 weeks. From participants’ medical records, students gathered 2.5 information about causes of low back pain, treatments for pain (including medications, procedures, and 2 surgeries), comorbidities, and Body Mass Index (BMI). Figure 1. Association between Depression and Anxiety and Opioid Use 160 No Opioid use Opioid use 140 1 0.5 0 120 Number of Subjects 1.5 Dep - 100 Dep + Anx - Anx + High score is indicator of good function, good health; low score is very limited function, poor health. 80 60 40 Conclusions 20 0 Dep - Dep + Anx - Anx + Depression X2=20.886, p=.000; Anxiety X2=6.674, p=.010 •Depression, anxiety and panic attacks were very strong predictors of opioid use in patients. These results are consistent with past studies which found that patients with depression report higher pain and take more opioids (4). •Patients who reported mental health symptoms also had worse pain, physical function, role functioning and health scores. Table 1. Linear Regression Outcome= Role Function Predictors Beta p-value Depression -.186 .002 Anxiety -.112 .064 Diagnosis -.154 .003 Predictors also entered included panic attacks. Acknowledgements This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Dean’s Office, School of Medicine, UTHSCSA; the Texas Academy of Family Physicians; the South Texas Area Health Education Center; the National Center for Research Resources (Award # UL 1RR025767); and the Health Resources and Services Administration (Award # D54HP16444). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources of the National Institutes of Health. •Because depression and anxiety are so highly prevalent in patients with chronic low back pain, screening for depression and anxiety can help physicians in their treatment of back pain. It is possible that treating depression or anxiety could decrease the need for opioids, and increase a patient’s physical functioning. References 1) Freburger JK, Holmes GM. The rising prevalence of chronic low back pain. Arch Intern Med 2009; 169: 251-8. (2) Anderson JA. Epidemiological aspects of back pain. Journal of the Society of Occupational Medicine 1986;36:90-4. (3) Currie SR, Wang J. Chronic back pain and major depression in the Canadian population. Pain 2004;107:54–60. (4) Bair MJ, Robinson RL. Depression and Pain Comorbidity. Arch Intern Med 2003;163: 2433-2445.