Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
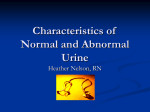
PROTOCOL PEDIATRIC SMALL BOWEL TRANSPLANT DATE: PATIENT NAME: MEDICAL RECORD #: ATTENDINGS/CONSULTING SERVICES PICU: TRANSPLANT: SURGERY: OTHER CONSULTANTS: DR.JOHN (312 –996-9291, BEEPER 3634) ANESTHESIA, PLASTIC SURGERY MONA BOTTKE BEEPER 3632 PEDS and TX PHARM D STAFF DIETARY CONSULT RADIOLOGY PATHOLOGY 1. Draw blood for: Chem 7, PI, Mg, Liver function, CBC, PT, PTT. Type and cross match (per transplant service 2 units). Check transplant service for special labs on donor/recipient). 2. CXR (EKG and ECHO). 3. History and physical exam. Need height, weight, and surface area 4. UA, urine culture, other cultures. (stat) 5. Notify Ramona Bottke, (3632) out patient follow-up, Kathy Lusher for discharge plans, Lucy Ramirez for social issues and transport. 6. Pre-transplant immunosuppressive medications per transplant service; call Transplant PharmD for transplant medication protocol. POST OPERATIVE SMALL BOWEL TRANSPLANT ORDERS VITALS: BP, HR, RR, Q ½ - 1 hour CVP q 1 hour TEMP q 1 – 6 hours Daily weights and urine—specific gravity Strict I & O q ½ - 1 hour FIRST 2-4 DAYS THEN Q 2-4HRS FLUIDS:MAINTENANCE(IWL+STOOL LOSSES+URINE LOSSES+WOUND LOSSES+THIRD SPACE AND OTHER LOSSES) IWL – 400cc – 600cc/M2 (can be given as D5W, 2NS or Hyperal) plus urine replacement cc/cc plus other losses. STOOL REPLACEMENT: CC/CC WITH RINGERS LACTATE URINE REPLACEMENT: OBTAIN UA AND URINE LYTES DAILY DURING FIRST TWO WEEKS THEN AS NEEDED DW5% 0 .45%NS + 20-35MEQ/L OF KCL (ADJUST KCL CONCENTRATION IN IV FLUID BASED ON SERUM K+. Keep Serum K ABOVE 3MEQ/L) + BICARBONATE 30-70 MEQ/L TO KEEP SERUM BICARBONATE AT 21-23 MEQ/L (solution to match urine losses of electrolytes) WOUND AND SKIN LOSSES: REPLACE – WITH 5%ALBUMIN 1 THIRD SPACE FLUID LOSSES: REPLACE WITH 25%ALBUMIN ½-1G/KG OVER 2-4 HRS FOLLOWED BY 1-2MG/KG OF LASIX TO MOBILIZE NORMAL SALINE BOLUS FOR: CVP < 10-12 cms. Urine output less than 2cc/hr/kg BP lower than the parameter (<110/70 – 120/80 mmHg). Inform TRANSPLANT SERVICE IF THERE ARE ANY major changes in stool out put. TRANSFUSION: Avoid unless acutely indicated. Inform Transplant and Renal Services. BLOOD PRESSURE: High BP (parameters to be set by DR.JOHN AND TX SERVICE) give IV medication (Hydralazine or Labetalol), Q 3-6 hours; important not to drop the BP quickly to avoid thrombosis of the graft and/or CNS problems. FEVER: Tylenol Work up for infection (bacterial, viral and fungus), (blood, urine, STOOL, tracheal aspirate and wound). CMV PCR, EBV PCR BACTERIAL; AEROBIC AND ANAEROBIC CULTURE LABS: ELECTROLYTES Serum lytes, BUN, Cr, Ca, Mg ,Pi Q 4-6 hrs X 1-2 days, then q 8 hr, then q 12 hr, and then once a day LIVER FUNCTION STUDIES DAILY OR AS NEEDED (micro blood samples please). URINE: Na, K, Cl, Cr once a day as needed. UA and urine for protein/creatinine ratio to be done daily Ca/P/Mg/LFT’s: Daily or as needed. CBC: Q 8 – 12 hrs then daily as needed. PT/PTT: Q 6 – 12 hrs or as needed CSA /FK506 level: Trough level in a.m. daily to three times a week (keep CSA level at 250-270 & FK 12-20). CHEST: X ray as needed. CULTURES: Blood, line, urine, throat, stool as indicated (bacterial, viral, fungal). Stoma and wound culture as needed. ULTRASOUND, CT SCAN: Abdominal/graft as indicated. 2 ENDOSCOPY/ SMALL INTESTINAL BIOPSY Q WEEKLY OR AS NEEDED TO R/O REJECTION; PER TRANSPLANT SERVICE AND SURGERY SERVICE. DURING NPO GIVE IV SOLUTION WITH ELECROLYTES TO REPLACE URINE AND INSENSIBLE LOSSES MEDICATIONS: Immunosuppression medications per Transplant Service KEEP IN TOUCH WITH TRANSPLANT SERVICE REGARDING IMMUNOSUPPRESSION MEDS CHANGES Need to change CSA, FK506 (TACROLIMUS) daily, Imuran, TG/OKT3, based on WBC, GI FUNCTION, LIVER FUNCTION AND REJECTION, and infection status. ANTIBIOTICS; ADJUST FOR LIVER AND RENAL FUNCTION Pre-medicate patient with Tylenol and Benadryl prior to ATG/TG/OKT3 immune suppressant medications. PHYSIOTHERAPY OT AS SOON AS POSSIBLE TO AVOID MUSCLE WASTING AND OTHER COMPLICATIONS PAIN CONTROL/AND ITS COMPLICATIONS; PICU/PAINMANAGEMENT TEAM SPECIAL TESTS; FAT ABSORPTION TEST: 72 HRS STOOL COLLECTION.* DIETICIAN TO MEASURE DIETARY FAT CONTENT DURINGTHIS PERIOD (72HRS) Fecal Fat Protocol Name Fat, Quantitative, Stool CPT 82710 Synonyms Fat Quantitative; Fat, Quantitative, 72-Hour Stool Collection; Lipids, Total, Quantitative, Stool; Quantitative Fecal Fat, 72-Hour Collection Laboratory Core Laboratory Referral to Referred Request Form Computer Order or Test Request Form 1095 Phone Results and specimen information: 6-4440; technical/clinical information: 6-3972 Availability Daily, 24 hours Turnaround Time 1 week Special Instructions Requisition must state date and time collection started and date and time collection finished. Specimen 72-hour stool collection Volume Entire collection Minimum Volume 20 g or 80 mL Container Wide mouth container Patient Preparation Adult patients should be on a standard diet containing 100 g fat per day for at least 3 days before test is started and during the test. Causes for Rejection Improper container, foreign matter other than feces inside container, patient not on special diet, not 72-hour collection Reference Range 0-6 g/24 hours Use Diagnose the presence of steatorrhea, supporting a diagnosis of one of the malabsorption syndromes, including nontropical sprue, Crohn's disease, chronic pancreatitis, cystic fibrosis, Whipple's disease Limitations Fecal fat collection does not provide a diagnostic explanation for the presence of steatorrhea. Contraindications: Patient taking mineral oil. Patient having barium enema within previous week Additional Information: The three major causes of steatorrhea, which is a pathological increase in fecal fat, are impairment of intestinal absorption, deficiency of pancreatic digestive enzymes, and deficiency of bile. Fecal fat quantitation measures total fatty acids in stool; not only dietary triglycerides (neutral fats) and lipolytic byproducts (split fats) but also fatty acids 3 of phospholipids and cholesterol esters. Identification of types of stool fat (eg, free fatty acids, triglycerides, neutral fats, phospholipids) is of little value. Fecal fat excretion >6 g/day is abnormal but nonspecific. XYLOSE ABSORPTION;* 145G/M2 IV NPO 4-6HRS Protocol for Xylose Test D-XYLOSE TEST (per Johns Hopkins: The Harriet Lane Handbook: A Manual for Pediatric House Officers, 16th ed., Copyright © 2002 Mosby, Inc.) Purpose: To screen for small bowel malabsorption by measuring the amount of D-xylose absorbed after an oral load. Unreliable in patients with edema, renal disease, delayed gastric emptying, severe diarrhea, rapid transit time, or small bowel bacterial overgrowth. Method: Have infants fast for 4 to 6 hours, older children for 8 hours. Give a 14.5 g/m2 (maximum 25 g) oral load of D-xylose as a 10% water solution. Ensure adequate urine output using supplementary oral or intravenous (IV) fluid, collect all urine for 5 hours, and send for quantitation. Alternatively, send serum specimens for D-xylose concentration before the load and 30, 60, 90, and 120 minutes after the load. (PATIENT WAS GIVEN 6 GRAMS OF XYLOSE) Interpretation (urine) Children >6 months old 5 hours urinary excretion of <15% of the oral load suggests malabsorption. 15% to 24% is indeterminate. >25% is normal. Infants <6 months old: 5 hours urinary excretion <10% suggests malabsorption. Interpretation (serum): Failure of the serum level to exceed 25 mg/dl in any of the postabsorptive specimens suggests malabsorption e.g.; Based on Zachary's last known height and weight, 14.3kg and 94.5cm, his BSA = sqrt (14.3 x 94.5 / 3600) = 0.61 D-Xylose and Tacrolimus Kinetics Xylose levels are collected in a grey top tube. Please place this form when completed in the bedside chart. Please page Kelly 4985 with questions. 1. Around 6am, draw baseline xylose level and tacrolimus trough. Record time ____________. 2. Give tacrolimus and then mix d-xylose powder in 50-100mL water and administer through G-tube. Record time ____________. 3. Draw a xylose level at 30min, 1 hr, and 2 hrs. Draw tacrolimus at 1 hr, 2hr, 4hr, and a trough before the 2pm dose. Xylose 30min (6:30) _________ Tacrolimus 1hr (7am) _____________ 1hr (7:00am) _________ 2hr (8am) _____________ 2hr (8:00 am) _________ 4hr (10am) _____________ 8hr trough (2pm) _________ 4 FK506;* KINETICS AND AREA UNDER THE CURVE SERUM B12, CARNITINE, VITAMIN D METABOLITES, AND AMINOACIDS AS NEEDED STOOL ELECTROLYTES; WEEKLY OR AS NEEDEED OTHER SPECIAL CARE; STOMA CARE; LINE CARE CHEST TUBE CARE; SKIN GRAFT CARE; DISCHARGE PLANS; TRANSPLANT PHARM D TO EDUCATE PARENTS REGARDING IMMUNESUPPRESSIVE MEDICATIONS PEDS PHARM D; GET THE MED LIST READY AND REINFORCE ABOUT MEDICATION DOSAGE AND ITS COMPLICATIONS KATHY LUSHER TO ORGANIZE FOR HOME SUPPLIES AND OTHER NEEDED ARRANGEMENTS AS WELL AS INSURANCE ISSUES LUCY RAMIREZ; TO ARRANGE FOR TRANSPORTATION AND CONFIRM ABOUT INSURANCE MONA BOTTKE; TRANSPLANT NURSE TO ARRANGE FOR OUT PATIENT CLINIC FOLLOW UP DR.HOLTERMAN AND HIS STAFF TO ARRANGE FOR WEEKLY BIOPSY AND SEDATION DISCHARGE SUPPLIES; DRESSING IV FLUIDS IV SET WIGHING MACHINE BP MACHINE UA DIPSTICK I/OLOG SHEETS WEIGHING SCALE IV MEDICATIONS PAIN MEDS VISITING NURSE 5 Cumulative Volume Status 5000 4000 Volume (cc) 3000 2000 1000 0 -1000 -2000 Cumulative -3000 10 / 26 10 /02 /2 8 10 /02 /3 0/ 11 02 /1 / 11 02 /3 / 11 02 /5 / 11 02 /7 / 11 02 /9 11 / 02 /1 1 11 /02 /1 3 11 /02 /1 5 11 /02 /1 7 11 /02 /1 9 11 /02 /2 1 11 /02 /2 3 11 /02 /2 5 11 /02 /2 7 11 /02 /2 9/ 12 02 /1 / 12 02 /3 /0 12 2 /5 / 12 02 /7 / 12 02 /9 /0 2 -4000 Time FLUID BALANCE CHART FOR TRANSPLANT SERVICE Special labs (to send) 1. EBV PCR Quantification Contact person : Dr. Kadkol, Shrihari. Director, Molecular pathology, MC 847. Pathology Rm. 446 CMW phone: 312-996-7312 Specimen : Blood 2 cc in green top and label to send for EBV DNA quantification real time PCR code 10186 and write as discuss and approve with Dr. Kadkol to be send out Note : Please contact Dr. Kadkol before send specimen 2. Citrulline level Contact person : Biochemical Genetic Lab (6-5326). Specimen: Approximately 0.8 cc in a green top bullet tube to the Biochemical Genetic Lab (65326). 6