Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychedelic therapy wikipedia , lookup
Drug interaction wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Discovery and development of direct Xa inhibitors wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
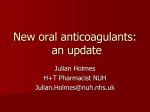
New Anticoagulants For Stroke Prevention in AF Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, BoehringerIngelheim, Bristol Myers Squibb, Otsuka, Forest, Janssen, Daiichi-Sankyo Atrial Fibrillation and Stroke ● Stroke is the most common complication of AF1,2 – Incidence of all-cause stroke in AF patients is 5%1 – Approximately 15% of all strokes in the U.S. are caused by AF1 (75,000 strokes per year) – 90% of strokes in NVAF are ischemic – Elderly ( > 75 y.o.) AF pts (No AC) have a 5.49 increased risk of ischemic stroke vs. < 65 y.o.3 – Annualized stroke rate is 3.2% in paroxysmal and 3.3% in persistent AF ● Ischemic stroke associated with AF is often more severe than stroke from other etiology4 ● Stroke risk persists even in asymptomatic AF5 ● In AF patients <70 years old: 187% greater risk of dementia and 130% increased risk for Alzheimer's6 ) 1) Fuster V, et al. J Am Coll Cardiol. 2006;48:854-906 ; 2. Benjamin EJ, et al. Circulation. 1998;98:946-9523. 3) Friberg L, et al. Eur Heart J 2012; 33:1500-1510; 4) Dulli DA, et al. Neuroepidemiology. 2003;22:118-123; 5) Page RL, et al. Circulation. 2003;107:1141-1145; 6) Bunch. Heart Rhythm Society-. Boston, MA., 2009. Stroke Risk Stratification in AF Annual Risk of Stroke (%) CHADS2 Risk Factor Cardiac failure HTN Age ≥75 years Diabetes Stroke Score 1 1 1 1 2 CHA2DS2-VASc Risk Factor Score Cardiac failure 1 HTN 1 Age ≥75 years 2 Diabetes 1 Stroke 2 Vascular disease (MI, peripheral 1 arterial disease, aortic atherosclerosis) Age 65-74 years 1 Sex category (female) 1 HTN = hypertension; MI = myocardial infarction. Lip GY, et al. Am J Med. 2010;123(6):484-488. 20 18 CHADS2 16 CHA2DS2-VASc 14 12 10 8 6 4 2 0 0 1 2 3 4 5 6 7 8 9 Total Score Camm AJ, et al. Eur Heart J. 2010:31;2369-2429. 1 ACCP 2012 AF Guidelines Antithrombotic therapy recommendations to prevent stroke Risk Category CHADS2 Score Low Risk 0 Moderate Risk 1 High Risk ≥2 Recommended Therapy No therapy If therapy, preferred: Aspirin over OAC* or combination of aspirin and clopidogrel OAC* Preferred: OAC* over aspirin or combination of aspirin and clopidogrel OAC* *Dabigatran 150mg twice daily preferred over a vitamin K antagonist. ACCP = American College of Chest Physicians; OAC = Oral anticoagulant. You JJ, et al. Chest. 2012;141:e531S-75S. ESC Focused AF Guideline Update ● The efficacy of stroke prevention with aspirin is weak, with a potential of harm, since the risk of major bleeding (and ICH) with aspirin is not significantly different to that of OAC, especially in the elderly ● The use of antiplatelet therapy (as aspirin-clopidogrel combination therapy or - less effectively - aspirin monotherapy for those who cannot tolerate aspirinclopidogrel combination therapy) for stroke prevention in AF should be limited to the few patients who refuse any form of OAC ● The CHA2DS2-VASc score is better at identifying “truly low risk” patients with AF and as good as – and possibly better than – scores such as CHADS2 in identifying patients who develop stroke and thromboembolism Camm AJ, et al. Eur Heart J 2012 ESC Focused AF Guideline Update ● The NOACs offer better efficacy, safety, and convenience compared with OACS with VKAs. Thus, where and OAC is recommended, one of the NOACs – either a direct thrombin inhibitor (dabigatran) or an active factor Xa inhibitor (e.g. rivaroxaban, apixaban) – should be considered instead of adjusted-dose VKA ( INR 2-3) for most patients with AF ● There is insufficient evidence to recommend one NOAC over another, although some patient characteristics, drug compliance and tolerability, and cost may be important considerations in the choice of agent Camm AJ, et al. Eur Heart J 2012 2 Mechanism of Action of Warfarin Steps in Coagulation Coagulation Cascade Drug TF/VIIa Initiation X IX VIIIa Va Xa Propagation IXa Warfarin II Thrombin (IIa) Thrombin Activity Fibrinogen Fibrin Adapted with permission from Weitz JI, et al. Chest. 2004;126:265S-286S. Weitz JI, et al. Chest. 2004;126:265S-286S. Hirsh J, et al. Circulation. 2003;107:1692-1711. Efficacy of Warfarin Compared With Control in 5 Studies 62% to 67% RRR with warfarin vs placebo No. of PatientEvents Years AFASAK 27 Risk Reduction, % 811 BAATAF 15 922 CAFA 14 478 SPAF 23 508 SPINAF 29 972 Combined 108 3691 100 50 0 Warfarin Better -50 -100 Warfarin Worse Atrial Fibrillation Investigators. Arch Intern Med. 1994;154(13):1449-1457. Warfarin for Nonvalvular AF Pooled data from AFASAK, SPAF, and BAATAF For every 1000 patients with nonvalvular AF in clinical trials treated with warfarin for 1 year: Benefit Risk 31 fewer thromboembolic events* 1 more intracranial or major bleed* *Compared with control 35 more minor bleeds occurred with warfarin Intention-to-treat analysis Risk of ICH increases with age Adapted from Albers GW et al. Ann Neurol. 1991;30:511-8. 3 Therapeutic Range for Warfarin: Balancing Safety and Efficacy Odds Ratio 15.0 Stroke 10.0 Intracranial Bleeding Therapeutic Range 5.0 1.0 0 1.0 2.0 3.0 5.0 4.0 6.0 7.0 8.0 INR Hylek EM, Singer DE. Ann Intern Med. 1994;120(11):897-902. Hylek EM, et al. N Engl J Med. 2003;349(11):1019-1026. Warfarin Use: Medicare Cohort % Taking Warfarin 60 50 40 30 20 10 0 1992 1994 1996 1998 2000 2002 Year Adapted from Lakshminarayan K, et al. Stroke. 2006;37(8):1969-1974. TTR Was 55% in a Systematic Overview of US Centers Setting TTR (95% CI) Anticoagulation clinic-based warfarin dosing 0.63 (0.58,0.68) Community-based warfarin dosing 0.51 (0.47,0.55) Overall 0.55 (0.51,0.58) 0.2 0.5 1.0 TTR (95% CI) ● Analysis of 8 studies with >41,000 patient years of total follow-up ● Anticoagulation clinic services are associated with improved TTR Abbreviations: TTR = time in therapeutic range; CI = confidence interval. Adapted from Baker W et al. J Manag Care Pharm. 2009;15(3):244-252. 4 INR Control and Outcomes in AF Cumulative Survival ● 486 AF patients with CHADS2 ≥2 on warfarin ● Mean duration of treatment, 986 days; mean of 66 INRs ● Compared with no warfarin, stroke was significantly reduced only in patients with TTR >70% 1.0 TTR 0.9 71–100% 61–70% 51–60% 41–50 % 31–40 % <30% Non-warfarin 0.8 0.7 0.6 0 500 1000 1500 Survival to Stroke (days) TTR, time in therapeutic range. Morgan CL, et al. Thromb Res. 2009;124(1):37-41. The Challenges of Using Warfarin – The intensity of AC achieved through the use of warfarin is affected by a number of genetic, environmental, and patient factors Interacting medication (eg, NSAIDs, ASA) Drug-related Dietary vitamin K intake Herbal supplements Alcohol Inability to adhere to restrictions (dietary, drug, alcohol, etc) Poor compliance with medication Dosing errors Discomfort or inconvenience of frequent venipuncture Age Patient Genetic medical (CYP2C9, VKORC1) characteristics Acute Warfarin management diarrheal illness Renal impairment Hepatic dysfunction Impaired GI absorption Malignancy Patient capabilities or preference ASA=aspirin; CYP2C9=cytochrome P450 2C9; GI=gastrointestinal; NSAIDs=nonsteroidal antiinflammatory drugs; VKORC1=vitamin K epoxide reductase complex, subunit 1. Merli GJ, Tzanis G. J Thromb Thrombolysis. 2009;27(3):293-299. Aspirin Has Minimal Efficacy in Preventing CVA in AF Aspirin vs Placebo Relative Risk Reduction (95% CI) AFASAK I SPAF I EAFT ESPS II LASAF UK-TIA All Trials (N=6) 100% 50% Aspirin Better 0% –50% –100% Aspirin Worse Hart RG, et al. Ann Intern Med. 1999;131(7):492-501. 5 Antiplatelet Therapy in AF ACTIVE-W: 6706 randomized patients; trial stopped ACTIVE-A: 7554 randomized patients; median follow-up of 3.6 years 8 P = .0003 5 4 P = .001 3 P = .53 2 Clopidogrel + ASA ASA 6 5 4 P<.001 3 P<.001 2 1 1 0 P = .01 7 Outcome/Year (%) Outcome/Year (%) 6 Clopidogrel + ASA Warfarin Vascular Event Stroke 0 Major Bleeding Vascular Event Stroke Major Bleeding ACTIVE = AF Clopidogrel Trial with Irbesartan for Prevention of Vascular Events. ACTIVE Investigators. Lancet. 2006;367:1903-1912. ACTIVE Investigators. N Engl J Med. 2009;360(20):2066-2078. Sites of Action for the New Anticoagulants Intrinsic XII Extrinsic XI TF IX VII VIII X V Thrombin IIa Fibrinogen Xa Inhibitors – Apixaban – Edoxaban* – Rivaroxaban Direct Thrombin Inhibitor – Dabigatran Fibrin Clot *Not currently FDA approved. Weitz JI, et al. Chest 2001;119:95S-107S. Gulseth MP, et al. Am J Health Syst Pharm 2008;65:1520-1529. New Oral Anticoagulants Drug Dabigatran Rivaroxaban Apixaban Edoxaban Mechanism of Thrombin inhibitor action FXa inhibitor FXa inhibitor FXa inhibitor Half-life 14-17 h 6-9 h 12 h 6-12 h Regimen BID QD, BID BID QD Peak to trough ~7x 12x (QD) 3-5x ~3x Renal excretion ~80% 36-45% 25-30% 35% CYP3A4 substrate and Pglycoprotein inhibitor CYP3A4 substrate(min) P-glycoprotein inhibitor Potential drug P-glycoprotein inhibitor interactions CYP3A4 substrate and Pglycoprotein inhibitor Usman MH, et al. Curr Treat Cardiovasc Med. 2008;10(5):388-397. Piccini JP, et al. Curr Opin Cardiol. 2010;25(4):312-320. 6 Heidbuchel H, et al. Europace 2013;15:625-651 Restricted Use of Dabigatran, Rivaroxaban and Apixaban ● Renal impairment ● Pregnancy Category C: No adequate and wellcontrolled studies ● Labor and delivery ● Nursing mothers ● Pediatric use ● Prosthetic Heart Valves RE-ALIGN trial stopped due to more thromboembolic and bleeding events with dabigatran in bi-leaflet mechanical prosthetic heart valves Dabigatran ● ● ● ● ● ● ● ● ● Potent, competitive, reversible inhibitor of thrombin Binds clot-bound and free thrombin (high affinity/ specificity) Bioavailability 6.5%; low protein binding No known food or CYP450 drug interactions – Decreased absorption with H2 blockers/PPIs Decreased levels with PGP inducers (rifampin) and increased levels with PGP inhibitors (verapamil, amiodarone, dronedarone) Dyspepsia most common subjective adverse effect No need for INR monitoring Half-life: 8 hours after single dose and 14-17 hours after multiple doses with BID dosing 80% renal excreted 7 RE-LY® – PROBE Study Design Non-valvular atrial fibrillation at moderate to high risk of stroke or systemic embolism (at least one additional risk factor) (N=18,113) R Warfarin 1 mg, 3 mg, 5 mg (INR 2.0-3.0) N=6022 ● ● ● ● Dabigatran Etexilate 110 mg bid N=6015 Mean CHADS2 = 2.1 Median TTR = 67% Dabigatran Etexilate 150 mg bid N=6076 Primary objective: Non-inferiority to warfarin Minimum 1 year follow-up, maximum of 3 years; mean 2 years Primary end point: Stroke + systemic embolism Primary safety outcome: Incidence of major bleeds Connolly SJ, et al. N Engl J Med. 2009;361(12):1139-1151 NOAC Trials: Key Exclusion Criteria ● RELY – Mechanical prosthetic valve or hemodynamically significant valve disease – CrCl < 30 ml/min ● ROCKET AF – Hemodynamically significant MS or any valve prosthesis – CrCl < 30 ml/min ● ARISTOTLE – Moderate or severe MS or prosthetic valve – Cr >2.5 or CrCl <25 ml/min ● ENGAGE AF (TIMI 48) – Moderate or severe mitral stenosis, unresected atrial myxoma, or a mechanical heart valve – CrCl < 30 ml/min All patients had to be candidates for warfarin and low dose ASA allowed in all trials RE-LY Trial Dabigatran vs. Warfarin 18,113 patients with nonvalvular AF randomized to warfarin (goal INR 2-3), dabigatran (150 mg BID), or dabigatran (110 mg BID) for a median of 2 years P=0.051 4.0 P=0.32 3.5 Warfarin INR 2.03.0 Percent/Year 3.0 2.5 2.0 1.5 Dabigatran 150 mg twice daily TTR=67% Superiority P<0.001 Noninferiority P<0.001 P<0.001 P=0.03 P<0.001 1.0 P<0.001 0.5 0.0 Stroke or Ischemic HemorrhagicAll Cause Stroke Systemic Mortality Stroke Embolism Major Intracranial Major GI Bleed Hemorrhage Bleed P-values are for superiority. The 110 mg twice daily is not presented as this dose was not approved by the FDA. AF = Atrial fibrillation; FDA = US Food and Drug Administration; GI = Gastrointestinal; MI = Myocardial infarction; TTR = Time in therapeutic range. Connolly SJ, et al. N Engl J Med 2009;361:1139-1151. Connolly SJ, et al. N Engl J Med 2010;363:1875-1876. 8 Dabigatran: Recommended Dosing Creatinine Clearance >30 mL/min 15-30 mL/min <15 mL/min or dialysis Dabigatran Dose 150 mg twice daily 75 mg twice daily contraindicated • Avoid use with PgP inducers (rifampin) • If CrCl 30-50 and dronedarone – consider 75 mg bid ROCKET AF Enrolled Patients With Nonvalvular AF at Moderate to High Risk of Stroke Nonvalvular AF Mean CHADS2 score = 3.5 Randomized double-blind/ double-dummy (N=14,264)2 CHADS2 Risk Factors • Prior stroke, TIA, or non-CNS systemic embolus – OR – • CHF or LVEF ≤35% At least 2 • Hypertension required • Age ≥75 years • Diabetes Warfarin Rivaroxaban 20 mg/d (15 mg/d for CrCl 30 to <50 mL/min)1,2 INR target: 2.0 to 3.0 inclusive Monthly assessments* Warfarin management was determined by clinician1,2 Mean CHADS2 = 3.5 Median TTR for the warfarin arm was 58% Patel MR et al. N Engl J Med. 2011;365(10):883-891. ROCKET AF Study Investigators. Am Heart J. 2010;159(3):340-347. Rivaroxaban: Pharmacologic Profile ● Oral, once-daily dosing ● Predictable pharmacokinetics and pharmacodynamics1,2 ● Rapid onset – 1/3 Unmetabolized Direct Renal Excretion 2/3 Metabolized in Liver Cmax of 2 to 4 hours – Maximum inhibition of Factor Xa activity at 1-4 hours after administration3* ● Dual mode of clearance1 – 1/3 direct renal excretion – 2/3 metabolized in the liver ● T1/2 of 5 to 9 hours in healthy individuals aged 20 to 45 years – T1/2 11 to 13 hours in the elderly 1/2 excreted via the bile 1/2 excreted via renal elimination ● No requirement for routine coagulation monitoring4,5 Abbreviations: T1/2 = half-life. *Phase I randomized single-blind dose escalation study in 108 healthy white males aged 19 to 45 years. Single doses of rivaroxaban 1.25, 5, 10, 15, 20, 30, 40, 60, and 80 mg tablets were tested. 1. Perzborn E et al. Nat Rev Drug Discov. 2011;10(1):61-75. 2. Mueck W et al. Int J Clin Pharmacol Ther. 2007;45(6):335-344. 3. Kubitza D et al. Clin Pharmacol Ther. 2005;78(4):412-421. 4. Mueck W et al. Clin Pharmacokinet. 2008;47(3):203-216. 5. Patel MR 27 et al. N Engl J Med. 2011;365(10):883-891. 9 Inhibition of Factor Xa (%) Rivaroxaban: Inhibition of Factor Xa Activity over 24 hour Period Anti-Factor Xa Activity 70 60 Rivaroxaban Rivaroxaban Rivaroxaban Rivaroxaban 50 40 5 mg (n=6) 10 mg (n=8) 20 mg (n=7) 40 mg (n=8) Placebo (n=25) 30 20 10 0 -10 0 2 4 6 8 10 12 14 16 18 20 22 24 Time (hours) ● ● Results from a randomized, single-blinded, placebo-controlled, dose-escalation study demonstrated that once-daily dosing regimens of rivaroxaban tablets above 5 mg resulted in Factor Xa inhibition through 24 hours* Results provided foundation for once-daily dosing regimens for evaluation in phase 3 programs *Pharmacokinetics/pharmacodynamics do not imply clinical effectiveness. Kubitza D et al. Clin Pharmacol Ther. 2005;78(4):412-421. Rivaroxaban Clinical Development Program (>60,000 Patients) Indications Randomized Patients; vs Comparator DVT prophylaxis after knee or hip surgery 9011 patients; vs enoxaparin Approved Stroke/systemic embolism in patients with nonvalvular AF1 14,264 patients noninferiority; vs warfarin Approved ACS secondary prevention2 >15,000 patients in addition to standard therapy Investigational VTE primary prevention in medically ill patients3 ~8000 patients; vs enoxaparin Investigational VTE treatment and secondary prevention4,5 >9000 patients; vs enoxaparin and warfarin/acenocoumarol Approved Study Program Status Abbreviations: ACS = acute coronary syndrome; AF = atrial fibrillation; DVT = deep vein thrombosis. 1. Patel MR et al. N Engl J Med. 2011;365(10):883-991. 2. Gibson CM et al. Am Heart J. 2011;161(5):815-821. 3. ClinicalTrials.gov. http://clinicaltrials.gov/ct2/show/NCT00809965. Accessed September 14, 2011. 3. Cohen AT et al. LBCT IV Session 3015. ACC 60th Annual Scientific Sessions. New Orleans; LA; April 2-5, 2011. 4. EINSTEIN Investigators. N Engl J Med. 2010;363(26): 2499-2510; 29 5. ClinicalTrials.gov. http://clinicaltrials.gov/ct2/show/NCT00439777. Accessed September 26, 2011. Events Occurring on Treatment and After Early Discontinuation Were Counted in ROCKET AF* Median follow-up=707 days1 Last dose +2 days Rivaroxaban R A N D O M I Z E Early discontinuation (23.7%)1 Open-label therapy1 Last dose +2 days Events counted (N=575)1 Open-label therapy1 Early discontinuation (22.2%)1 Warfarin Day 0 Last dose +2 days Last dose +2 days End-of-study site notification Open-label therapy included VKA, aspirin, or no therapy, per discretion of treating physician2 *Included all randomized subjects followed for events during treatment or after premature discontinuation until end-of-study site notification (N=14,171).2 1. Patel MR et al. N Engl J Med. 2011;365(10):883-891. 2. 2. ROCKET AF Study Investigators. Am Heart J. 2010;159(3):340-347. 10 ROCKET AF Trial Rivaroxaban vs. Warfarin 14,264 patients with nonvalvular AF randomized to warfarin (goal INR 2-3) or rivaroxaban (15-20 mg daily) for a median of 1.6 years 4.0 3.5 Percent/Year 3.0 Rivaroxaban 15 or 20 mg BID Hazard ratio 0.88 (95% CI 0.75 -1.03) Non inferiority P<.001 Superiority P=0.12 P<.001* Warfarin TTR=55% P=0.07 2.5 2.0 P=0.58 P=0.58 1.5 P=.02* 1.0 *P=.024 0.5 0.0 Stroke or Ischemic Hemorrhagic All Cause Systemic Stroke Stroke Mortality Embolism Major Intracranial Major GI Bleed Hemorrhage Bleed GI = Gastrointestinal, MI = Myocardial infarction; TTR = Time in therapeutic range. Patel MR, et al. NEJM 2011;365:883-891. The Importance of Adequate Anticoagulation After Discontinuation of Rivaroxaban Similar data for apixaban in ARISTOTLE 21 5 No. of Strokes ● Anticoagulation after discontinuation was not stipulated in ROCKET AF ● Warfarin patients who completed the study were generally maintained on warfarin ● Rivaroxaban patients were generally switched to warfarin – There was no co-administration of warfarin and rivaroxaban – This resulted in inadequate anticoagulation after stopping rivaroxaban until attaining a therapeutic INR Rivaroxaban (n=4637) Median time to INR 2.0-3.0 Warfarin (n=4691) 13 days 3 days Patel MR et al. N Engl J Med. 2011;365(10):883-991. Results in ROCKET AF Across Renal Functions Studied Favors Rivaroxaban n/N (%) Rivaroxaban Favors Warfarin Warfarin Stroke/non–CNS embolism1 Overall 269/7081 (3.8) 306/7090 (4.3) CrCl (mL/min) <50 50-80 77/1490 (5.2) 86/1459 (5.9) 126/3298 (3.8) 151/3400 (4.4) >80 65/2285 (2.8) 68/2222 (3.1) Major and nonmajor clinically relevant bleeding2 Overall 1475/7111 (14.91) 1449/7125 (14.52) CrCl (mL/min) <50 336/1502 (17.84) 342/1476 (18.28) 50-80 725/3313 (15.74) 719/3410 (15.30) >80 412/2288 (12.15) 388/2230 (11.42) 0.1 0.2 Patel MR et al. N Engl J Med. 2011;365(10):883-991. 0.5 1.0 2.0 5.0 10 HR 11 Rivaroxaban: Dosing CrCl (mL/min) Recommended once-daily dose of Rivaroxaban >50 20 mg 15 to 50 15 mg* <15 Avoid use ♦ Should be taken once daily with the evening meal ♦ If a dose of is not taken at the scheduled time, administer the dose as soon as possible on the same day – Do not administer 2 doses on the same day 34 dose for patients with CrCl of 15 to <30 Ml/min is based on exposure matching. *The 15-mg Apixaban ● Oral, reversible, and selective active site inhibitor of Factor Xa ● Bioavailability: 50% (no food effect) ● Maximum concentration 3-4 hours after dose ● Half-life: 12 hours ● Renal excretion: 27% ● Linear pharmacokinetics (if doses 25 mg or more – dissolution limited absorption and bioavailability) ● Plasma Protein Binding: 87% ● Metabolized mainly via CYP3A4; no active metabolites ● Apixaban is a substrate for P-gp transporter The AVERROES (Apixaban Versus ASA To Reduce the Risk Of Stroke) Trial unsuitable for warfarin therapy N= 5,598 E ASA (N=2791) (81–324 mg daily; up to 36 months/end of study) Mean duration of exposure = 59 weeks R Double-blind Apixaban (N=2807) (5 mg twice daily; 2.5 mg in selected patients*; up to 36 months/end of study) *At least two of: age 80 y; weight 60 kg; or serum Cr 1.5 mg/dl Is apixaban more effective than ASA in preventing stroke and systemic embolism in moderate to high-risk (stroke; at least one risk factor) AF patients? 10 efficacy endpoint: confirmed ischemic or haemorrhagic stroke or systemic embolism 20 study endpoints: as above, including MI or vascular death 10 safety endpoint: major bleeding Study period: until 226 primary outcome events have been observed; estimated 1o completion May 2010 In June 2010, BMS- Pfizer announced that the study had been stopped early because a predefined interim analysis revealed clear evidence of a clinically important reduction in stroke and systemic embolism. Eikelboom, et al. Am Heart J 2010;159:348-353; ClinicalTrials.gov identifier: NCT00496769; Connolly SJ, et al. N Engl J Med 2011;364:806-817 12 AVERROES: Stroke or Systemic Embolic Event RR=0.45 95% CI, 0.32-0.62 P<0.001 Cumulative Risk 0.05 ASA 0.03 Apixaban 0.01 0.0 0 3 6 9 12 18 21 Months Connolly SJ, et al. N Engl J Med 2011; 364:806-817 AVERROES: Primary Outcome Events Apixaban ASA Apixaban vs. ASA Annual Annual events events RR rate rate Outcome 95% CI P Stroke or SEE 52 1.6 112 3.6 0.46 0.33-0.64 <0.001 Stroke 50 1.5 103 3.3 0.48 0.34-0.68 <0.001 Ischemic 35 1.1 92 2.9 0.38 0.26-0.56 <0.001 Hemorrhagic 8 0.2 8 0.2 1.01 0.38-2.68 0.99 Type not determined 8 0.2 4 0.1 1.99 0.60-6.62 0.26 2 <0.1 13 0.4 0.15 0.03-0.69 0.01 SEE 38 30 Connolly SJ, et al. N Engl J Med 2011; 364: 806-817 AVERROES: Major Bleeding RR=1.13 95% CI, 0.74-1.75 P=.56 0.020 Apixaban Cumulative Risk 0.015 ASA 0.010 0.005 0.0 0 3 6 9 12 18 21 Months Connolly SJ, et al. N Engl J Med 2011; 364:806-817 13 The ARISTOTLE Trial: Apixaban ClinicalTrials.gov identifier: NCT00412984 Warfarin INR 2.0–3.0 (N=9081) AF or atrial flutter 18,201 randomized E Mean duration of exposure = 89 weeks R Double-blind *At least two of: age 80 years; weight 60 kg; or serum Cr 1.5 mg/dL Apixaban (N=9120) (5 mg twice daily; 2.5 mg twice daily in selected patients*) Is apixaban non-inferior to standard therapy (warfarin) in preventing stroke and systemic embolism in moderate to high-risk (stroke; at least one risk factor) AF patients? 10 efficacy endpoint: confirmed ischemic or hemorrhagic stroke, or systemic embolism 20 efficacy endpoints: composite of confirmed ischemic or haemorrhagic stroke, systemic embolism and all-cause death 10 safety endpoint: time to first occurrence of confirmed major bleeding Mean CHADS2 = 2.1 Median TTR = 66% Lopes, et al. Am Heart J 2010;159:331–339; Granger CB, et al. N Engl J Med. 2011; 365:981-992. ARISTOTLE Trial Apixaban vs. Warfarin 18,201 patients with AF+ ≥1: TIA/CVA/embolism, ≥75 years, History CHF or LVEF ≤40, HTN, DM P=0.047 4.0 Apixaban = 9120 3.5 P<0.001 Warfarin = 9081 Percent/Year 3.0 2.5 2.0 1.5 1.0 Non inferiority P<0.001 Superiority P<0.01 TTR = 66% P=0.42 P=0.37 P<0.001 P=0.001 0.5 0.0 Stroke or Ischemic HemorrhagicAll Cause Systemic Stroke Stroke Mortality Embolism Major Intracranial Major GI Bleed Hemorrhage Bleed GI = Gastrointestinal, MI = Myocardial infarction; TTR = Time in therapeutic range. Granger CB, et al. N Engl J Med. 2011;365(11):981-992. Apixaban: Dosing • Dosing: 5 mg bid with or without food • Recommended dose is 2.5 mg bid in patients with any 2 of the following characteristics: • age ≥ 80 years • body weight ≤60 kg • serum creatinine ≥1.5 mg/dL • When apixaban is co-administered with strong dual inhibitors of cytochrome P450 3A4 (CYP3A4) and P-glycoprotein (P-gp) (increases blood levels of apixaban), the recommended dose is 2.5 mg twice daily. • If already on 2.5 mg dose – avoid or do not use apixaban • Avoid concomitant use of apixaban with drugs that are strong dual inducers of cytochrome P450 3A4 (CYP3A4) and P-glycoprotein (P-gp) (decreases blood levels of apixaban) 14 ENGAGE AF TIMI 48: Edoxaban Warfarin INR 2.0–3.0 AF >20,000 pts 3 treatment arms E R Double-blind Edoxaban (60 mg vs. 30 mg qd) Is edoxaban non-inferior to standard therapy (warfarin) in preventing stroke and systemic embolism in moderate to high-risk (CHADS2 score > 2) AF patients? 10 efficacy endpoint: composite primary endpoint of stroke and systemic embolic events 20 efficacy endpoints: composite clinical outcome of stroke, systemic embolic events, and allcause mortality; also major bleeding events. 50% dose reductions occurred for one or more of the following: CrCl 30-50 mL/min; Body weight ≤60 kg; Concomitant strong P-gp inhibitors Treatment period: up to 2 years; results expected 2013 Ruff et al. Am Heart J 2010;160:635-641 ClinicalTrials.gov identifier: NCT00412984. Dabigatran as P-glycoprotein Substrate P-glycoprotein Dabigatran Efflux transporter X Dabigatran etexilate Dabigatran etexilate Dabigatran etexilate Rivaroxaban, Apixaban, Edoxaban also PgP substrates • P-gp inducers (rifampin, St. John’s Wort) – Reduce exposure to NOACS by – 33-65% and should be avoided absorption Bloodstream Intestinal lumen Gut wall X amiodarone, dronedarone, verapamil blockade of P-gp Drug – Drug Interactions ● Apixaban: Metabolized by CYP 3A4 and substrate of Pglycoprotein – Decrease dose to 2.5 mg twice daily in patients taking strong dual inhibitors of CYP 3A4 and P-glycoprotein (e.g., ketoconazole, itraconazole, ritonavir, clarithromycin) – Avoid coadministration of strong dual inhibitors of CYP 3A4 and P-glycoprotein in patients already taking 2.5 mg twice daily – Avoid coadministration with strong dual inducers of CYP3A4 and P-gp (e.g., rifampin, carbamazepine, phenytoin, St. John’s wort: will decrease apixaban exposure). Food and Drug Administration. Drugs@FDA – Apixaban. Available at: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm 15 Drug – Drug Interactions Continued ● Dabigatran: Metabolized by P-glycoprotein – Decrease the dose to 75 mg twice daily if coadministered with a Pglycoprotein inhibitor (e.g., dronedarone, ketoconazole) and the CrCl is 30-50 ml/min – Avoid if coadministered with a P-glycoprotein inhibitor (e.g., dronedarone, systemic ketoconazole) and the CrCl is <30 ml/min – Avoid in conjunction with P-glycoprotein inducers (e.g., rifampin) ● Rivaroxaban: Metabolized by P-glycoprotein and CYP3A4 – Avoid in conjunction with P-glycoprotein and strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, ritonavir, etc.) – Avoid in conjunction with P-glycoprotein and strong CYP3A4 inducers (e.g., carbamazepine, phenytoin, rifampin, St. John’s wort) Food and Drug Administration. Drugs@FDA – Dabigatran or Rivaroxaban. Available at: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm 20 Dabigatran plasma concentration ECT ratio INR aPTT ratio 150 4 TT ratio 3 100 2 50 1 0 0 4 8 12 16 20 16 12 8 TT (ratio) 200 INR and aPTT, ECT (ratio) Dabigatran Plasma Concentration (ng/mL) Dabigatran Plasma Concentrations Parallel Its Anticoagulant Effect 4 0 24 Time (h) aPTT= activated partial thromboplastin time, ECT= ecarin clotting time, INR= international normalized ratio, TT= thrombin time. Stangier J et al. Br J Clin Pharmacol. 2007;64:292-303. Monitoring Anticoagulation ● Normally there is NO indication for anticoagulation monitoring of new agents ● Agents can prolong various clotting tests – DO NOT provide a reliable and accurate prediction of a patient’s coagulation status ● Apixaban: – Prolongs clotting tests: prothrombin time (PT), INR and activated partial thromboplastin time (aPTT) – Not recommended to monitor anticoagulation effect of apixaban – Rotachrom FXa assay is a test where the activity correlates well with drug levels of apixaban. aPTT = Activated partial thromboplastin time; INR = International Normalization Ratio. Food and Drug Administration. Drugs@FDA - Apixaban. Available at: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm Barrett Y, et al. Thrombosis and Haemostasis. 2010;104(6):1263–1271. 16 Monitoring Anticoagulation Continued ● Dabigatran: – Coagulation status can be assessed using the aPTT, ECT, and TT – INR cannot be interpreted in the same way as with warfarin – aPTT is the most widely available test with a level of 40 seconds corresponding to the lowest 10th percentile in the RE-LY trial ● Rivaroxaban: – Coagulation status can be assessed using the PT/INR, aPTT, HepTest, and Anti-factor Xa activity – Among the more widely available tests, the PT/INR is more sensitive than the aPTT aPTT = Activated partial thromboplastin time; ECT = Ecarin clotting time; TT = Thrombin time. Food and Drug Administration. Drugs@FDA – Dabigatran or Rivaroxaban Available at: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm Switching Patients From Warfarin to NOACs ● Dabigatran – stop warfarin and start dabigatran when INR < 2.0 ● Rivaroxaban – stop warfarin and start rivaroxaban when INR < 3.0 ● Apixaban – stop warfarin and start apixaban when INR < 2.0 To switch from one NOAC to another consider just substituting new drug at next dose Periprocedural Management of New Anticoagulants ● Apixaban: – Stop ≥ 48-hrs before elective surgery or invasive procedures with moderate or high risk of significant bleeding – Stop ≥ 24 hrs before elective surgery or procedures with low bleeding risk ● Dabigatran: – Stop 1-2 days (CrCl ≥ 50 mL/min) or 3-5 days (CrCl < 50 mL/min) before elective surgery or invasive procedures ● Rivaroxaban: – Stop ≥ 24 hours before elective surgery or invasive procedures – Bridging therapy not usually required – Consider longer discontinuation times (≥5-7 days) in patients undergoing major surgery, spinal puncture, or placement of a spinal or epidural catheter or port, in whom complete hemostasis may be required Food and Drug Administration. Drugs@FDA – Apixaban or Dabigatran or Rivaroxaban. Available at: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm 17 NOACs: Reversing Anticoagulation Effects There is no established way to reverse the anticoagulant effect of NOACs; some of the anticoagulant effect can be expected to persist for 24-48 hours after the last dose (relevant for bridging for procedures) Specific antidote for NOACs not available Dabigatran is dialyzable, because of high plasma protein binding, apixaban and rivaroxaban are not dialyzable Protamine sulfate and vitamin K, hemostatics or antifibrinolytic agents would not be expected to affect the anticoagulant activity of NOACs Use of procoagulant reversal agents such as prothrombin complex concentrate, activated prothrombin complex concentrate, or recombinant factor VIIa may be considered but has not been evaluated carefully in clinical studies Activated oral charcoal reduces absorption apixaban, thereby lowering plasma concentrations. This approach may be useful with dabigatran and rivaroxaban NOACs: DC Cardioversion N (Patients/CV) CVA/SEE Dabigatran 110 mg 409/647 5 (0.8%) Dabigatran 150 mg 415/672 2 (0.3%) Warfarin 431/664 4 (0.6%) Apixaban Warfarin /338 /419 0 (0%) 0 (0%) 143 143 3 (2.1%) 3 (2.1%) Rivaroxaban* Warfarin Nagarakanti R, et al. Circulation 2011;123:131-136 Flaker G, et al. ESC 2012 Piccini JP, et al. AHA 2012. *ARC study in progress SPAF: Novel Anticoagulants “Unanswered Questions” ● Best dose of dabigatran if CrCl 30-49 ml/min ● Safety and best protocol for all drugs peri- AF ablation – VENTURE-AF (Rivaroxaban) in progress ● Best measures of therapeutic anticoagulation ● Reversal agents ● Except for rivaroxaban – FDA approved doses for other indications not well established ● Use in mechanical prosthetic valves – proper dose?? ● Reasons for higher GI bleed and lower ICH 18 Summary: Novel Anticoagulants in AF ● Based on efficacy, safety, ease of use, new oral direct thrombin inhibitors and factor Xa inhibitor drugs will replace warfarin for many/most patients with AF ● Novel anticoagulants have a lower rate of ICH compared to warfarin ● Dose adjustments need to be made based on renal function ● Role in DC Cardioversion: Limited data – no data for any of compounds that is concerning ● Safety/efficacy of novel anticoagulants for AF ablation procedures still under study ● Need for antidote 19