Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
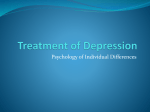
The Mind/Body Connection: Innovative Techniques to Compliment Medical Therapy Alice D. Domar, Ph.D Director, Domar Center for Mind/Body Health, Boston IVF, Beth Israel Deaconess Medical Center Harvard Medical School • Alice D. Domar, Ph.D, does not have a financial interest or affiliation with any of the research being presented What’s a Nurse To Do? • Understand the psychological challenges facing our patients • Be familiar with the most common psychological reactions to infertility • Be aware of the resources available to your patients • Don’t take their distress personally Infertility Treatment as the Cause… • Numerous forms of infertility treatment are associated with the development of depressive symptoms: – 80% of women taking leuprolide acetate scored higher than 20 on the Hamilton Rating Scale* – 75% of women using GnRH agonist medication reported depressive symptoms** – *Warnock et al, Fertil Steril 2000; 74: 984-6 – **Steingold et al, Obstet Gynecol 1987; 69: 403-11 . • In a very large study in Denmark, more than 42,000 women who underwent IVF were assessed for a depression diagnosis*. Of those who were diagnosed: • 34.7% prior to ART • 4.7% during ART • 60.7% after ART • Sejbaek et al Hum Reprod 2013; 28: 1100-9 . • Thus, be aware of the huge psychological toll that treatment takes on our patients • Women who had a depression diagnosis prior to undergoing ART underwent significantly fewer cycles and experienced fewer live births than women who did not have a depression diagnosis prior to ART treatment. • Women who are depressed are significantly more likely to drop out of treatment after one ART cycle than women who are not depressed Prevalence of Depressive Symptoms • Measuring the prevalence of symptoms in this patient population can be challenging. Patients may want to “fake good” so as to ensure entry into treatment and in some cultures, revealing psychological distress is frowned upon*. It is not at all uncommon for a patient to deny any level of depression and actually score 0 on a depression scale. * Lewis et al, Arch Womens Mental health 2013; 16: 87-92 . • Suicide is a real risk in infertile women who are not successful with treatment: – In a study of 51,221 infertile women, the risk of suicide in women who did not conceive was more than two times that of the suicide rate of women who did* – Women with secondary infertility also had an increased risk, but it was not statistically significant *Kjaer et al Hum Reprod 2011 Impact of Depressive Symptoms on Treatment Outcome • The research is unclear as to the impact of depression on treatment outcome. • Most studies indicate that distress prior to or during an IVF cycle is associated with lower pregnancy rates but some studies have not shown a relationship • It is challenging research for several reasons: – Distress is associated with prognosis, so patients with a better prognosis report less distress, and also have higher pregnancy rates, but it might not be cause and effect – Patients may not accurately report their true level of distress Treatment for Distress • Interventions currently offered to patients include: – Individual therapy – Couples therapy – Support groups – Mind/body groups – Medication – Complementary or Alternative Medicine (CAM) • There is little data to support the efficacy of individual or couples therapy in the decrease of distress or the increase in pregnancy rates but there has been minimal research • There is some data on support groups indicating increased pregnancy rates and a decrease in distress • In one study of 31 patients with major depressive disorder randomized to either 12 sessions of interpersonal psychotherapy (IPT) or brief supportive psychotherapy*: – IPT patients had a better response, with >2/3 achieving a >50% reduction in symptoms and improvements persisted six months later *Koszycki et al Arch Womens Ment Health 2012 • Two meta-analyses have been done on the efficacy of psychological interventions with infertility patients: – One concluded that interventions which included skills acquisition training were more effective than those which emphasized emotional expression or support* – The other concluded that programs that were at least six sessions were the most effective** • • *Boivin Soc Sci Med 2003 ** Hammerli et al Human Reprod 2009 Mind/Body Groups for Infertility • Efficacy: – Significant decrease in psychological symptoms such as depression, anxiety, and hostility – Decrease in physical symptoms such as insomnia, headaches, and abdominal pain – Significant increase in pregnancy rates: in an RCT*, the take home baby rate for the m/b subjects was 55%, compared to 20% in the control group. *Domar et al Fertil Steril 2000; 73: 805-11 • In another RCT* on the impact of the mind/body program on pregnancy rates in women undergoing their first IVF cycles, participants in the mind/body group had a 52% pregnancy rates compared to a 20% rate in the control group* *Domar et al Fertil Steril 2011; 95: 2269-73 Mind/body groups • • • • • 10 session group program Buddy system Peer counselors co-lead Partners attend three of the ten sessions Patients have a variety of diagnoses • First half hour is an optional sharing support time • Different relaxation technique taught each week • Hand in weekly diary sheet to group leader • • • • • • Skills include: Numerous relaxation techniques Cognitive strategies Lifestyle modifications How to handle anger/shame/guilt Recommendations about alternative treatments • Group support • A recent study on a similar program, the Mindfulness-Based Program for Infertility* had similar results: – Participants reported a significant decrease in depressive symptoms, shame, entrapment and defeat *Galhardo et al Fertil Steril 2013 Antidepressant Medications In a recent study at Boston IVF*: • 11.1% of the patients self-reported on the patient portal that they were currently taking antidepressant medication • However… • Only 3% reported antidepressant use to the anesthesiologist prior to their oocyte retrieval *Domar et al Fertil Steril 2013 Impact of SSRI Use on IVF – Klock et al 2004: • pregnancy rates: – SSRI users: 46% – Non users: 63% – Friedman et al 2009 • cycle cancellation rates: – SSRI users: 26.8% – non-users: 10% 24 Risks: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Spontaneous abortion (miscarriage) Birth defects Preterm birth Preeclampsia Smaller fetal head size Decreased fetal growth Newborn behavioral syndrome (seizures) Persistent pulmonary hypertension of the newborn (PPHN) Neonatal EKG changes Death within the first year of life Long-term neurobehavioral effects (? Autism ? Language?) Long-term health effects (Pulmonary, GI, Sexual) 25 “Never before in human history have we artificially changed the architecture of brain development.” ---- Feng Zhou, Ph.D. Indiana University School of Medicine 26 AD Work AD Don’t Work 27 Alternatives to Medications for the Treatment of Depressive Symptoms • • • • • • Psychotherapy Exercise Relaxation training Yoga Acupuncture Nutritional supplements Psychotherapy • The majority of research on non-pharmacological treatment of depression is on the efficacy of psychotherapy, specifically cognitive-behavioral therapy (CBT). • CBT is short-term, typically 4-10 sessions • Patients recognize and challenge distorted automatic beliefs CBT • Huge amount of evidence that CBT is equivalent to antidepressant medication in the treatment of mild to moderate symptoms • Recent research shows it is effective in the treatment of severe symptoms as well • Psychiatric research concludes that CBT is the optimal first line treatment for depression CBT vs SSRIs • Relapse rates are lower for CBT than for medication • CBT is more costThoughts effective than medication Behaviors Emotions SSRI vs CBT • 89 infertile women with depressive symptoms* • Randomized to receive CBT, fluoxetine (20 mg for 90 days) or placebo. • CBT patients had 79% decrease in symptoms compared to 50% in fluoxetine patients and 10% in placebo patients • *Faramarzi et al, J Affec Dis 2008; 108: 159-64 Exercise • Randomized controlled trials comparing SSRIs vs exercise have indicated that exercise is equivalent in the treatment of depressive symptoms • It can be difficult however to motivate depressed patients to institute an exercise routine and vigorous exercise might be contraindicated in some infertility patients Relaxation training • Requires less time and training than CBT • More effective than no treatment, but less effective than CBT Yoga • There is limited research on the impact of yoga on depressive symptoms, although some small studies have shown significant results • Since yoga has no side effects, it is worth considering in patients with mild to moderate symptoms Acupuncture • There is recent research which supports the efficacy of acupuncture to treat symptoms of depression and anxiety in infertile women*, including at least one RCT in women with PCOS** *Anderson et al Altern Ther Health Med 2007, **Stener-Victorin et al BMC Complement Altern Med 2013 • There are numerous studies which support the efficacy of acupuncture to treat symptoms of depression and anxiety during pregnancy* **. • The response rates are equivalent or better than the response rates to antidepressant medication *Da Silva, Acupunc Med 2007 **Manber et al, Obs Gyn 2010 Nutritional Supplements • There is recent research which indicates that omega-3 fatty acids and myo-inositol may have some antidepressant effects*. • Since the data is still limited, they are considered to be adjunctive treatment options. • *Domar et al Human Reprod 2013;28:160-71 Treatments for Depression (Khan, Faucett, Lichtenberg, Kirsch, & Brown, 2012) Summary: The Mind/Body Connection and Infertility • Depression is a common symptom in infertile women and may well be exacerbated by treatment • Psychological interventions, including mind/body groups and CBT, as well as acupuncture should be considered as a first line treatment for distress Summary • Exercise has many physical and psychological advantages and should be considered as an initial option for motivated patients • Yoga, relaxation training, and nutritional supplements should be considered as additional options, but not stand-alone treatments, unless new research supports their efficacy The Domar Center for Mind/Body Health at Boston IVF • Services include: – Acupuncture – Psychotherapy: CBT, individual, couples – Nutritional counseling – The mind/body program – Yoga Patient Support • Acupuncture is available 7 days/week, 365 days/year • Any Boston IVF patient in crisis can be seen within the hour by one of the psychologists • Any patient who has bad results from a prenatal ultrasound has the option of being seen for 5-10 minutes within the hour and a regular appointment within 24 hours • Every Boston IVF patient who has an unsuccessful treatment cycle is offered a free 30 minute consultation with a psychologist to process the negative results and plan support for the next treatment cycle Employee Support • Employees receive one free acupuncture visit and 25% off all future visits • “Stress lunches” are offered periodically throughout the year to all employees • Crisis interventions are provided to employees when needed, free of charge Self Care • Working with this patient population can be challenging for a variety of reasons: – Patients are highly distressed yet often assertive – Patients seek out potentially erroneous information from the internet – Nurses may be put in the situation of being the gatekeeper from the physician • It is vital to recognize symptoms of stress: – physical: insomnia, headaches, neck and/or back pain, gastrointestinal distress, shortness of breath, chest pain, fatigue – emotional: anxiety, sadness, tearfulness, irritability, anger, hopelessness – behavioral: decreased motivation to exercise, more sweet or salty cravings, more alcohol intake, increased gum chewing, increased smoking Most Effective Stress Reduction Strategies • Physical: relaxation techniques such as meditation or yoga, mini relaxation techniques, appropriate nutrition, exercise • Emotional: cognitive restructuring, social support, journaling, self-nurturance Summary • Infertility patients experience significant distress but there are treatment modalities which can effectively lower that distress • It is vital that the nurses who take care of infertility patients feel comfortable discussing the emotional impact of infertility as well as ways to minimize it • It is equally vital that nurses understand the impact of these patients on their own mental health, recognize stress-warning signs, and take steps to remain physically and emotionally healthy