Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
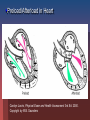
Cardiac Medications Hypertension Learning Objectives Students will be able to: Discuss the major categories of drugs as they relate to the treatment of Cardiac Disease. Describe the major effects of various medications on cardiac function. Discuss major nursing implications when administering above medications. New Zealand Statistics: Maori die almost a decade earlier than non-Maori in New Zealand. Cardiovascular disease is a major contributor to this statistic (NZGG, 2003). Maori should therefore be assessed for risk 10 years earlier than non-Maori. Hypertension Defined as a consistent elevation of the systolic or diastolic blood pressure above 140/90mm Hg On two elevated readings (sitting and supine) on separate office visits Two types hypertension Primary: no known cause Secondary: consequence of underlying disease or condition Goal with hypertension: Two primary regulatory factors: Blood flow (volume) Peripheral Vascular Resistance (PVR) Goal is to optimise these two in order to get pressure below 140/90 mm Hg Primary groups of drugs are used: Diuretics Adrenergic inhibitors (Beta-blockers) Vasodilators ACE inhibitors Calcium antagonists Diuretics: to reduce overall volume of blood Thiazides - block sodium reabsorption in nephron’s distal segment Water is excreted with sodium, producing decreased blood volume Loop diuretics – potent loop diuretic that inhibits sodium and chloride reabsorption at proximal and distal tubules and ascending loop of Henle Indicated for acute pulmonary oedema MedlinePlus Medical Encyclopedia Diuretics Cont’d Nursing Interventions: Monitor K+ routinely (depleted here) Monitor weight daily and intake/output Give in am so avoid nocturia Potassium-sparing diuretics (Aldactone or Spironolactone) Potassium sparing diuretic Antagonises aldosterone in the distal tubules which increases sodium and water excretion Need to watch for hyperkalemia and don’t give potassium supplements Monitor electrolytes and fluid intake/output Monitor blood pressure and daily weights Less potent than thiazide and loop diuretics but useful as an adjunct to other diuretic therapy Vasodilators Hydralazine hycrochloride (Apresoline) Dilate peripheral blood vessels by directly relaxing arteriolar smooth muscle Usually used in combination with other antihypertensives as they increase sodium and fluid retention Calcium Antagonists Felodipine, Nifedipine, Diltiazem Inhibit the influx of calcium into muscle cells; act on vascular smooth muscle (primary arteries) to reduce spasms and promote vasodilatation May enhance serum Digoxin levels Cardiac Medications Coronary Artery Disease New Zealand Statistics Cardiovascular disease is the leading cause of death in New Zealand (NZGG, 2003). 1998 N.Z. had age-standardised mortality rate from CAD of 111/100,000 people CAD death rates for Maori less than 75 yrs old are 2-3X higher than non-Maori and 2X as high for Pacific peoples. So what is the overall goal in managing CAD? To reduce 5-year cardiovascular risk to less than 15% with medications (NZGG, 2003). Ensure individuals with total cholesterol greater than 8mmol/L undergo risk assessment and lipid modifying treatment. Ensure BP less than 170/100 drug treatment Different drug effects: Inotropic: relating to or influencing the force of contraction Chronotropic: influencing the rate; especially the heart beat Dromotropic: affecting the conductivity of cardiac muscle -- used of the influence of cardiac nerves Jarvis, 2000, Figure 17-8. p. 505. Overview of Pulmonary/Systemic Circulation Carolyn Jarvis, Physical Exam and Health Assessment 3rd Ed. 2000. Figure 17-1. p. 498. Copyright by W.B. Saunders So what is the goal of medical management of heart disease? Dissolve clots (save muscle) Maximize blood flow to heart muscle Maximize preload Minimize the afterload Maximize cardiac contractility (inotropic effect) Reduce chances clot formation Reduce overall blood volume if overload Heart rate between 60-80 beats/min to maximize cardiac output and filling pressures Treat arrhythmias Preload/Afterload in Heart Carolyn Jarvis, Physical Exam and Health Assessment 3rd Ed. 2000. Copyright by W.B. Saunders So what drugs help meet these goals? Dissolve existing clots quickly—TPA, Urokinase Maximize preload— I.V. fluids, volume expanders Minimize afterload—Ace inhibitors, IABP Maximize cardiac contractility—Digoxin, Dopamine Decrease preload, increase coronary circulation, and reduce pulmonary congestion—Nitrates Reduce chances clot formation—ASA or other anti-platelet medications Reduce overall fluid volume in overload--diuretics Keep heart rate between 60-80/min (Beta blockers and Calcium-channel blockers) Arrhythmias—Atropine, Lidocaine, etc. Fibrolytic Drugs TPA-tissue plasminogen activators Streptokinase Image from site http://www.americanheart.org/presenter.jhtml?identifier=4751 Nitrates GTN Cause vasodilatation reducing the amount of blood returning to the heart from the venous system, thus decreasing preload. This decreases the work of the heart and the demand of the myocardium for oxygen. Also dilate the peripheral arteries, decreasing the resistance against which the left ventricle must pump (decreases afterload). Increases coronary vasodilation ACE Inhibitors (pril) Used to treat both hypertension and ACS Inhibit the conversion of angiotension I to angiotension II, thus blocking the release of aldosterone, thereby reducing sodium and water retention Potassium-sparing so watch for hyperkalemia Reduce afterload of heart Inotropes Digitalis Inhibits the sodium-potassium pump, causing an increase in intracellular sodium levels Increased sodium levels force sodium out of the cell in exchange for calcium Higher intracellular calcium levels increase the force of contraction, increasing cardiac output Digoxin also blocks the slow calcium channels of the AV nodes, slowing the HR Antiplatelet Agents Low dose Aspirin Aspirin blocks the formation of thromboxane A2 , inhibiting platelet aggregation A single daily dose of around 80mg can effectively sustain the desired antiplatelet effect Anticoagulants Heparin (Clexane) Binds to anti-thrombin, inactivating coagulation factors and thrombin, thereby blocking the conversion of fibrinogen to fibrin Side Effects: Anticoagulants, Fibrolytics and Antiplatelets Bleeding What symptoms would you see? INR Beta-blockers Block beta-adrenergic receptors of CNS Blockage of beta-1 receptors causes a decrease in the force of contraction, a slowing heart rate, and a slowing of impulse of conduction (negative inotrope, chonotrope, dromotrope) These 3 mechanisms of action combine to decrease myocardial oxygen demand Calcium-channel blockers Action: thought to inhibit calcium ion influx across cardiac and smooth muscles, decreasing contractility and oxygen demand. May also dilate coronary arteries. Nursing implication: monitor for rapid drop in BP (especially if given intravenously). Cholesterol Lowering Agents: hypolipidaemic drugs Statins Reduce plasma lipids and lipoproteins Block the production of LDLs and increase receptor activity that removes LDLs Take other drugs 1 hour before or 4-6 hours after Questran to avoid blockage of absorption Cardiogenic shock: Inability of the impaired ventricle to perfuse and oxygenate body tissues Common in MI that damages 40% or more of the left ventricle. Signs: Systolic BP less than 90 mmHg Anxiety, restlessness, confusion, coma Cool, moist, clammy skin Rales in lungs, decreased (<30ml/hour) urine output S3 and S4 heart sounds Coma and death Cardiac Medications Congestive Heart Failure Congestive Heart Failure Table 17-10. p. 548. What can cause CHF? CAD multiple heart attacks High BP Faulty heart valves Cardiomyopathy Myocarditis Congenital heart defects Cardiac arrhythmias Aims of treatment CHF: Relieve symptoms Improve quality of life Prevent readmission to hospital, and/or recurrent ischaemic events Reduce mortality (Lonn & McKelvie, 2000) Drugs used to treat CHF ACE Inhibitors Beta Blockers Diuretics Vasodilators Inotropes (e.g. Dopamine) Digitalis Inotropes Digitalis Inhibits the sodium-potassium pump, causing an increase in intracellular sodium levels Increased sodium levels force sodium out of the cell in exchange for calcium Higher intracellular calcium levels increase the force of contraction, increasing cardiac output Digoxin also blocks the slow calcium channels of the AV nodes, slowing the HR Dopamine Stimulates dopamine receptors in the renal vessels, increasing renal blood flow, increasing diuresis Net result is an increase in cardiac output Increase in systemic arterial pressure Anti-arrhythmic Drugs Ventricular arrhythmias Amiodarone Treatment of tachyarrhythmias – supraventricular nodal and ventricular tachycardias, atrial flutter and fibrillation. Lignocaine Decreased the depolarisation and excitability in the ventricles. Potassium Chloride Intracellular ion Transmission of nerve impulses Contraction of cardiac muscles Levels 4.0-4.5 Hypokalaemia=potassium deficit Nursing implications CHF: Daily weights Strict intake/output records May be on fluid restriction (1500ml/24hrs) Teaching regarding medications Elevate feet to avoid stasis ulcers Oxygen on at all times Monitor BP, heart rate, respiratory rate, pulse oximetry frequently (every 2-4 hours) Monitor labs (electrolytes, troponin-T) Auscultate lung fields to assess for change every 4 hours!