Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
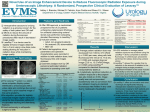
IMAGING & THERAPEUTIC TECHNOLOGY 521 The AAPM/RSNA Physics Tutorial for Residents Digital Fluoroscopy1 Robert A. Pooley, PhD ● J. Mark McKinney, MD ● David A. Miller, MD A digital fluoroscopy system is most commonly configured as a conventional fluoroscopy system (tube, table, image intensifier, video system) in which the analog video signal is converted to and stored as digital data. Other methods of acquiring the digital data (eg, digital or charge-coupled device video and flat-panel detectors) will become more prevalent in the future. Fundamental concepts related to digital imaging in general include binary numbers, pixels, and gray levels. Digital image data allow the convenient use of several image processing techniques including last image hold, gray-scale processing, temporal frame averaging, and edge enhancement. Real-time subtraction of digital fluoroscopic images after injection of contrast material has led to widespread use of digital subtraction angiography (DSA). Additional image processing techniques used with DSA include road mapping, image fade, mask pixel shift, frame summation, and vessel size measurement. Peripheral angiography performed with an automatic moving table allows imaging of the peripheral vasculature with a single contrast material injection. Introduction The digital environment in radiology includes tools that may be used to enhance the clinical examination. This enhancement may take the form of dose savings to the patient and medical personnel, increased imaging efficiency, or improved visualization of anatomic and physiologic processes. To realize these enhancements, it is important to have a fundamental understanding of the imaging technology and practical knowledge of how the digital tools are implemented for clinical use. This statement is true in general and specifically for digital fluoroscopy. Digital fluoroscopy is currently most commonly configured as a conventional fluoroscopy system in which the analog video signal is converted to a digital format with an analog-to-digital converter (ADC). An in-depth discussion of digital detector technologies (eg, flat-panel “direct” detection of x rays and charge-coupled device technology) is beyond the scope of this article. After a review of several fundamental Abbreviations: ADC ⫽ analog-to-digital converter, DSA ⫽ digital subtraction angiography Index terms: Digital subtraction angiography ● Fluoroscopy ● Images, processing ● Physics ● Radiography, digital RadioGraphics 2001; 21:521–534 1From the Department of Radiology, Mayo Clinic, 4500 San Pablo Rd, Jacksonville, FL 32224. From the AAPM/RSNA Physics Tutorial at the 1999 RSNA scientific assembly. Received October 25, 2000; revision requested December 11 and received December 19; accepted December 21. Address correspondence to R.A.P. (e-mail: [email protected]). © RSNA, 2001 522 March-April 2001 RG f Volume 21 ● Number 2 Figure 1. Comparison of the composition of decimal and binary numbers. In both systems, numbers are formed by multiplying a digit by a multiplication factor that is dependent on the position of the digit and the base (eg, 10 or 2) of the numbering system. The resulting products are then added together to form a decimal representation of the number. Figure 2. Effect of pixel size, number of pixels, and field of view on image spatial resolution and proper reproduction of imaged objects. As the number of pixels increases and their size decreases (at a constant field of view), the original object is more faithfully reproduced in the image. digital imaging concepts including binary numbers, pixels, and gray levels, emphasis will be placed on discussions of the digital imaging tools specific to digital fluoroscopy and digital subtraction angiography (DSA). Binary Numbers Although the decimal number system encodes values by using 10 digits (0 –9), the binary number system encodes values by using only two digits (0,1). Recall how a decimal number is built and the similarities in how a binary number is formed (Fig 1). A binary number with three digits (bits) can encode up to eight different values (000 –111 in binary, 0 –7 in decimal). A 4-bit binary number can encode up to 16 (24) different values (0000 –1111 in binary, 0 –15 in decimal), and an 8-bit number can encode up to 256 (28) different values (0 –255 in decimal). Pixels A pixel can be described as the smallest element of a digital image. A digital image is normally composed of a two-dimensional (square) matrix of pixels. A pixel can be characterized by its loca- tion, size, and value. The matrix size of an image is used to describe the number of pixels in each row and column of the image. The size of a pixel determines the smallest detail visible in the image, and the number of pixels (of a given size) determines the field of view of the image. As discussed later in this article, the pixel value is assigned to a certain color or gray level for visualization. Pixel size has an effect on object edge definition (Fig 2); the same is true of matrix size at a constant field of view. The imaged object is more faithfully reproduced as matrix size increases and pixel size decreases. In medical imaging, different applications use different matrix sizes depending on the clinical requirements and technology. Although nuclear medicine and functional magnetic resonance (MR) images may have matrix sizes as low as 642, MR and computed tomographic images normally have matrix sizes from 1282 to 5122 pixels, digital fluoroscopy normally uses 5122 to 1,0242 pixels, and digital chest radiography may have more than 1,500 –2,000 pixels on a side. A comparison of the same image reproduced at different matrix sizes demonstrates loss of edge definition and small object detail as matrix size decreases (Fig 3). RG f Volume 21 ● Number 2 Pooley et al Figure 3. Comparison of a clinical image at different matrix sizes: 512 ⫻ 512 (a), 256 ⫻ 256 (b), 128 ⫻ 128 (c), 64 ⫻ 64 (d), 32 ⫻ 32 (e), and 16 ⫻ 16 (f). The images show an endoscope inserted via the mouth and through the stomach into the second portion of the duodenum; the ampulla was cannulated to provide an endoscopic retrograde cholangiopancreatogram. Contrast material is seen in the common bile duct, pancreatic duct, and intrahepatic bile ducts. As matrix size decreases, larger pixels are required to maintain a constant field of view. As the pixel size increases, image spatial resolution decreases; edge definition is lost and smaller objects are not well visualized. 523 524 March-April 2001 Gray Levels As mentioned earlier, an 8-bit binary system can encode up to 256 different values. These 256 values can be assigned to 256 different colors or shades of gray. The assignment of a pixel value to a certain color or gray level is arbitrary. Often, in 8-bit gray-scale medical images, light pixels are given high values and dark pixels are given low values. The number of bits used to encode pixel values in an image is called the bit depth of the image. The displayed image is formed by associating image pixel values with gray levels on the display monitor (Fig 4). A comparison of the same image reproduced at different bit depths demonstrates loss of contrast resolution as bit depth decreases (Fig 5). Digital Fluoroscopy Digital fluoroscopy is most commonly configured as a conventional fluoroscopy system (tube, table, image intensifier, video system) in which the analog video signal has been digitized with an ADC. Alternatively, digitization may be accomplished with a digital video camera (eg, a charge-coupled device) or via direct capture of x rays with a flatpanel detector. For digital fluoroscopy systems in which the analog video signal is digitized with an ADC, the resolution is limited by the resolution of the video camera, which is typically 1–2 line pairs per millimeter. For the typical system, the ADC samples the analog video signal at discrete time points and converts the value of the signal to a binary number for storage. The maximum and minimum RG f Volume 21 ● Number 2 analog video signal values will be scaled to the maximum and minimum digital values according to the bit depth of the ADC. An 8-bit ADC will convert the video signal to a maximum of 256 different values. Improved representation of the analog video signal will occur as the bit depth of the ADC is increased and the sampling frequency of the discrete time points increases. Digital spot film images and photospot images may be acquired by using the same digital fluoroscopy system. Individual frames from a digital fluoroscopy sequence can be stored digitally and can be used instead of conventional spot film and photospot images. Digital photospot images will have the same characteristics (eg, resolution) as digital fluoroscopic images. The digital image data from digital fluoroscopy may be processed by using many useful image processing techniques. These techniques may serve to decrease radiation exposure to the patient and medical imaging staff or improve visualization of anatomy. Processing options include last image hold, gray-scale processing, temporal frame averaging, and edge enhancement. Additional processing is available when digital fluoroscopy data are used to perform DSA. Last Image Hold In conventional fluoroscopy, the patient’s anatomy is displayed on the video monitor only when the x rays are turned on to produce an image on the image intensifier. When the x rays are turned off, display of the patient’s anatomy is also turned off. Last image hold uses the digital information from the last frame (that is stored on the computer) and continuously provides this to the video system so that the display monitor continuously RG f Volume 21 ● Number 2 Pooley et al 525 Figure 4. Formation of a displayed image from a 4 ⫻ 4 matrix of pixel values (stored as a series of binary numbers). A 3-bit binary system is used, which can encode up to eight (23) different values (0 –7 in decimal). The eight values are assigned to eight shades of gray between white and black. The gray level assigned to a pixel value will be displayed at that pixel location in the matrix. Likewise, an 8-bit image may have a maximum of 256 different pixel values and 256 different shades of gray. Figure 5. Comparison of a clinical image at different bit depths (constant 5122 matrix): 256 gray levels (8 bits) (a), 16 gray levels (4 bits) (b), eight gray levels (3 bits) (c), and four gray levels (2 bits) (d). As the number of available gray levels decreases, contrast resolution decreases. Objects with pixel values similar to the surrounding pixel values are assigned the same gray level, making them indistinguishable (eg, the hepatic vessels). High-contrast objects (pixel values significantly different from those of surrounding tissue) are still visualized even at four gray levels (eg, the endoscope). Note that spatial resolution (edge definition) is maintained for the high-contrast objects. 526 March-April 2001 RG f Volume 21 ● Number 2 Figure 6. Last image hold. The last frame acquired before stopping x-ray acquisition is continuously displayed. Fluoro ⫽ fluoroscopic, l.i.h. ⫽ last image hold. Figure 7. Gray-scale processing. The image data have a range of pixel values from 0 to 255. The anatomy of interest may have a range of pixel values of 100 – 150. By setting the window width to 50 and the window level to 125, pixels with values below 100 are assigned to black, pixels with values above 150 are assigned to white, and pixels with values from 100 to 150 are assigned some shade of gray. shows the patient’s anatomy even after the x rays have been turned off (Fig 6). Use of this feature will dramatically decrease the ionizing radiation exposure to the patient and medical imaging staff. If display of the patient’s anatomy required review on a system without last image hold, x rays would continuously be used during this time. With last image hold, the display monitor can be studied with no additional dose to the patient. Gray-Scale Processing The term gray-scale processing generally refers to adjustment of the displayed contrast and brightness of the digital image; this technique is also referred to as adjustment of the window width and level (or center). The goal is to map (associate) pixel values from our image data set to some shade of gray on our display monitor so that visualization of the anatomy of interest is optimized. For example, even though the maximum and minimum pixel values in an image may be 255 and 0, respectively, the anatomy of interest may have pixel values only in the range of 100 –150 (Fig 7). In this case, the window width should be set to 50 and the window level should be set to 125. All objects with pixel values greater than 150 would be assigned to white, and all objects with pixel values less than 100 would be assigned to black. Brighter objects can be viewed by increas- ing the window level, and darker objects can be viewed by decreasing the window level. Objects whose pixel values span a wider range may require an increased window width (Fig 8). Temporal Frame Averaging Temporal frame averaging is used to decrease displayed image noise. The decrease is accomplished by continuously displaying an image that is created by averaging the current frame with one or more previous frames of digital fluoroscopic image data (Fig 9). Averaging more frames together decreases image noise further. Frame averaging may work well for static images, but the increased image lag may be unacceptable for imaging dynamic processes. Edge Enhancement Edge enhancement can be used to increase the conspicuity of boundaries between objects of different pixel values. One method used to produce edge-enhanced images is to subtract a blurred version of the original image from the original image and then add the resulting “edge image” to the original image (Fig 10). The blurred version of the original image is created by averaging a pixel value with surrounding pixel values and placing the new value in the location of the original pixel (eg, averaging the nine pixels in a 3 ⫻ 3 box and placing the averaged value at the center location). RG f Volume 21 ● Number 2 Pooley et al Figure 8. Comparison of a clinical image at different gray-scale settings. (a) A wide range of pixel values is mapped to white and black, giving a low-contrast appearance. (b) A narrow range of pixel values is mapped to white and black, giving a high-contrast appearance. The window level is set for optimized viewing of dark objects (eg, the endoscope). (c) Same window width as in b, but the window level is decreased for optimized viewing of objects with an intermediate pixel value (eg, the hepatic bile ducts). (d) Same window level as in c but with a window width intermediate between that in a and that in c. This may be the optimum setting for viewing all objects simultaneously in this image. Figure 9. Temporal frame averaging. Averaging five frames together may decrease image noise by up to 44%. As more frames are averaged together, display lag (persistence of displayed objects that have shifted position in the field of view) will increase. 527 528 March-April 2001 RG f Volume 21 ● Number 2 Figure 10. Edge enhancement. A blurred version (b) of the original image (a) is subtracted from the original image; the resulting edge image (c) is added to the original image to produce an edge-enhanced image (d). (Edge-enhanced image ⫽ [original image ⫺ blurred version] ⫹ original image.) The result is increased conspicuity of small objects and object edges. Digital Subtraction Angiography The acquisition of digital fluoroscopic images can be combined with injection of contrast material and real-time subtraction of pre- and postcontrast images to perform examinations that are generally referred to as digital subtraction angiography (Fig 11). Although the subtraction process increases image noise, perception of low-contrast vessels is increased due to the removal of distracting background tissue. With a properly calibrated system, quantitative data (eg, degree of stenosis) may also be measured. Recall that the image is formed by detection of x rays that have been attenuated exponentially in the body. Subtraction of pre- and postcontrast images must take this exponential attenuation into account in the form of a logarithmic subtraction. If logarithmic subtraction is not done, the brightness of the objects in the subtracted angiographic image (ie, the vessels with contrast material) will vary according to the brightness of the underlying tissue in the nonsubtracted images. Because the x-ray beam is not monoenergetic, the logarithmic subtraction is not perfect; there is still slight variation of vessel brightness that is dependent on the attenuation of the underlying tissue. DSA is used clinically for diagnostic and therapeutic applications of vessel visualization throughout the entire body (Figs 12–14). Comparison of precontrast, postcontrast, and subtracted images demonstrates increased perception of vessels with subtraction. RG f Volume 21 ● Number 2 Pooley et al 529 Figure 11. DSA. A precontrast mask image (which shows a distracting background structure and the tip of a catheter) is subtracted from a postcontrast image obtained at the same location (which shows contrast material–filled vessels). The result is an image of only the contrast material–filled vessels. During the actual imaging sequence, the subtraction process may begin slightly prior to contrast material injection, with each frame capturing a different phase of the injection. The sequence of subtracted frames can then be reviewed in cine mode or as still frames. The unsubtracted original digital fluoroscopic images are generally not reviewed. Figure 12. DSA. Cerebral arteriogram (oblique transorbital view) shows an aneurysm of the anterior communicating artery (junction of the A1 and A2 segments of the anterior cerebral artery). (a) Unsubtracted original digital fluoroscopic image obtained midway through the contrast material injection. (b– d) Subtracted DSA images obtained at three progressive time points during contrast material injection. 530 March-April 2001 RG f Volume 21 ● Number 2 Figure 13. DSA. Lateral view of the knee shows postsurgical changes from a total knee arthroplasty. (a) Precontrast digital fluoroscopic image. (b) Postcontrast digital fluoroscopic image shows the popliteal artery directly behind the knee joint. (c) Subtracted image. Note the increased perception of small vessels in the subtracted image due to removal of background tissue and the bright prosthesis. Also note the disappearance of small vessels overlying the prosthesis due to a low number of detected photons. Figure 14. DSA. Oblique view of the pelvis shows a pigtail catheter in the distal abdominal aorta and a metallic stent that extends through the right common and external iliac arteries. (a) Precontrast image. (b) Postcontrast image shows contrast material predominantly in the right common and external iliac arteries. (c) Subtracted image demonstrates improved vessel visualization. RG f Volume 21 ● Number 2 Pooley et al 531 Figure 15. Road mapping. First, DSA of the vascular structure is performed. The postcontrast frame associated with maximum vessel opacification becomes the road map mask; subsequent digital fluoroscopic (Fluoro) images are subtracted from the road map mask. The result is live fluoroscopic images of the inserted catheter or wire overlaid on a static image of the vasculature (with distracting underlying tissue removed). Figure 16. Use of road mapping with clinical images. (a) DSA image of a wire obtained without road mapping. It is more difficult to maneuver the wire through the vessels when the path of the vessels cannot be visualized. (b) Image of the wire obtained with road mapping. Real-time images of movement of the wire overlaid on a static image of the vessels facilitate guiding the wire through vessel turns. Road Mapping Road mapping is useful for the placement of catheters and wires in complex and small vasculature. A DSA sequence is performed, and the frame with maximum vessel opacification is identified; this frame becomes the road map mask. The road map mask is subtracted from subsequent live fluoroscopic images to produce real-time subtracted fluoroscopic images overlaid on a static image of the vasculature (Fig 15). When fluoroscopy alone is used, a small wire may not be visualized in the distracting underlying tissue. When subtraction fluoroscopy is used, the wire is well visualized but steering the wire through the vascu- lature is difficult, with no cues indicating the path of the vessels; road mapping provides these cues and facilitates maneuvering through the vasculature (Fig 16). Clinical use of DSA with road mapping serves as a powerful tool during complex interventional procedures (Fig 17). It is also possible to combine the road mapping feature with a feature called image fade, which allows the user to manually adjust the brightness of the static vessel road map overlay. 532 March-April 2001 RG f Volume 21 ● Number 2 Figure 17. Filling of distal arteries on control angiograms subsequent to packing of an aneurysm with coils (same patient as in Fig 12). The road mapping technique was used to guide the coils to the aneurysm; DSA was used to verify distal filling. (a) Image shows one coil in the aneurysm. (b) Image shows three coils in the aneurysm. The aneurysm is excluded from the circulation, and there is good filling of the A2 segments bilaterally. Figure 18. Peripheral angiography. Use of a stepping table (or stepping gantry) allows imaging of the peripheral vasculature with a single contrast material injection. As in DSA, pre- and postcontrast images are acquired at each position and subtracted. Peripheral Angiography Imaging of the entire peripheral vasculature can be accomplished with a single contrast material injection by using the stepping table or stepping gantry DSA technique (Fig 18). In the stepping table technique, the imaging gantry remains fixed while the patient table moves the anatomy of in- terest into the field of view. In the stepping gantry technique, the patient table remains fixed while the imaging gantry moves the field of view over the anatomy of interest. In both cases, timing of image acquisition with the moving contrast material bolus is critical. At each table or gantry position, images are acquired prior to contrast material injection. After contrast material injection, images are acquired at the exact same locations. The precontrast images are then subtracted from RG f Volume 21 ● Number 2 Pooley et al 533 Figure 19. Peripheral angiography with acquisitions at four positions (“knitted” together). The upper thigh demonstrates bilateral superficial femoral artery occlusions. The lower thigh and upper portion of the knee demonstrate reconstitution of severely diseased popliteal arteries bilaterally. Profunda femoris collateral vessels provide these reconstituted vessels with contrast material. The left posterior tibial artery is incomplete in the distal left lower leg. Figure 20. Mask pixel shift (same patient as in Fig 19). When patient motion occurs, pre- and postcontrast images can be reregistered for subtraction. (a) Original subtracted image. (b) Subtracted image with the subtraction mask shifted several pixels. Note the improved registration at the lower left knee and the increased misregistration artifact at the right knee. the postcontrast images, resulting in a clear depiction of the peripheral vasculature (Fig 19). Mask Pixel Shift When a digital subtraction technique is used, patient motion that occurs between acquisition of the precontrast images and acquisition of the postcontrast images will result in artifacts due to misregistration of the two images. If these artifacts are observed, it is possible to reregister the pre- and postcontrast images by shifting the subtraction mask (precontrast image) with respect to the postcontrast image and resubtracting the two images (Fig 20). Image Summation Image summation is used to combine two or more frames of a DSA imaging sequence into one image. An injection of contrast material may be made to visualize certain vessels, but the imaging frames may occur so rapidly that an individual frame captures only part of the vessel track (eg, the early phase of the contrast material injection). A complete single image of the vessels may be obtained by summing the frames that demonstrate the vessel segments (Fig 21). 534 March-April 2001 RG f Volume 21 ● Number 2 Figure 21. Image summation. Individual DSA frames can be combined to form a complete picture of vessel anatomy (eg, to include frames of early and late phases of contrast material injection). (a) Early-phase image from abdominal aortography. (b) Image obtained with image summation of early- and late-phase images shows single bilateral renal arteries and external iliac arteries. Vessel Size Measurement Digital distance measurements of imaged anatomy (eg, vessel diameter) can be accomplished with proper calibration of image pixel size. A reference object of known dimension can be placed in the imaging field of view. This known dimension can then be used to determine a calibration factor with units of millimeters per pixel. Distance measurements are then made by multiplying the number of pixels that span the anatomy by the calibration factor, a calculation that can be done automatically by the imaging system. The user should be aware of any errors due to differences in magnification of the reference standard and the anatomy of interest (Fig 22). Summary A digital fluoroscopy system is composed of a conventional fluoroscopy system plus hardware for the digitization, processing, and storage of images. The digital data may be processed in real time or during later review by means of many image processing techniques. These techniques can be used to decrease radiation exposure to the patient and medical staff or enhance the visualization of anatomy by adjustment of displayed contrast and brightness, edge enhancement, image noise reduction, or subtraction techniques. Suggested Readings Hoffmann KR, Hackworth CA, Chen Y. Digital techniques to assist in evaluation of the vasculature. In: Balter S, Shope TB, eds. Syllabus: a categorical course in physics—physical and technical aspects of angiography and interventional radiology. Oak Brook, Ill: Radiological Society of North America, 1995; 143–152. Kruger RA, Mistretta CA, Houk TL, et al. Computerized fluoroscopy in real time for noninvasive visualization of the cardiovascular system: preliminary studies. Radiology 1979; 130:49 –57. Figure 22. Distance measurements of vessel dimensions by means of proper system calibration. Washers of known diameter were placed on the skull in the field of view near the anatomy of interest. The number of pixels across the image of the washer is associated with the actual dimension of the washer in millimeters. Subsequent measurement of an aneurysm provides an estimate of the aneurysm diameter in millimeters (which is used to determine the loop diameter of packing coils). There will be some error in this method due to differences in magnification; the aneurysm and washers are at different distances from the image intensifier. Seibert JA. Digital image processing basics. In: Balter S, Shope TB, eds. Syllabus: a categorical course in physics—physical and technical aspects of angiography and interventional radiology. Oak Brook, Ill: Radiological Society of North America, 1995; 121–142. Sprawls P. Digital imaging concepts and applications. In: Frey GD, Sprawls P, eds. The expanding role of medical physics in diagnostic imaging: 1997 summer school proceedings. Madison, Wis: Advanced Medical Publishing, 1997; 18 –36. Verhoeven L. Design considerations of digital fluoroscopy/fluorography equipment. In: Seibert JA, Barnes GT, Gould RG, eds. Specification, acceptance testing and quality control of diagnostic x-ray imaging equipment: 1991 summer school proceedings. Woodbury, NY: American Institute of Physics, 1994; 651– 707.