Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
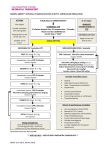
Aultman College of Nursing and Health Sciences Nursing 203 METI Experience: Code Blue – Faculty Goals: Discuss appropriate health history questions. Set priorities for specific presenting symptoms. Interpret the EKG findings throughout the scenario. Implement appropriate interventions for the abnormal assessment data. Perform a variety of roles during a code blue situation. Manage the client’s significant others during a critical situation. Evaluate own performance during the scenario. Plan: 30 minutes 30 minutes 30 minutes Contents of Code Cart Review Code Cart 1. Medications and use – EPI, Atropine, Amio, and Defibrillator Lido, Sodium Bicarb, Narcan, Vasopressin, Adenosine, Magnesium, Calcium Chloride 2. Code Blue Documentation Sheet 3. Intubation Tray (briefly) 4. Defibrillator (safe use), hands free, how to shock 5. AED 6. Pacer 7. Ambu Bag 8. CPR board Review various Cardiac Rhythms cardiac rhythms on 1. NSR, SB, ST, SVT, Afib, Aflutter, VTach simulator (with and without pulse), V fib, PEA, Asystole 2. Students to identify each and explain possible treatment options 4-5 students with Simulation lab has roles of staff nurse, charge nurse, METI MICU/SICU nurse, respiratory, recorder Have extra students observe Clinical instructor can play role of ACLS coordinator/resident doctor Both groups Questions located under debriefing. Allow students to discuss feelings they had during code openly. How will they run the next code more efficiently? 10-15 minutes debrief students on code blue 30 minutes Switch the above another code groups 10/14 LB, 1/07kg 1 Remaining time Medications: Name Epinephrine Vasopressin Allow students to practice skills, retry problem areas, and review sections they have questions about. Dose 1mg IVP bolus q3-5m Magnesium Sulfate 40u IVP bolus, once (in place of 1st/2nd dose of epinephrine) 1mg IVP may repeat q3-5m 1st dose – 6mg IVP 2nd dose – 12 mg IVP 3rd dose – 12 mg IVP Each dose followed by a 20 ml NS flush 1mEq/kg IVP bolus (give after 10 minutes of cardiac arrest for metabolic acidosis) 0.02-0.2mg q2-3min until response obtained (may need to repeat in 1-2h due to half-life) 1st dose - 300 mg IVP 2nd dose – 150 mg IVP Need a maintenance drip if converts rhythm 1-1.5mg/kg IVP q3-5 minutes Need a maintenance drip if converts rhythm 1-2g/100ml D5W over 2m Calcium Chloride 2-4 mg/kg IVP Atropine Adenosine Sodium Bicarbonate Narcan Amiodorone Lidocaine Cardiac Rhythm Treatments: Rhythm Normal Sinus Rhythm (NSR) Sinus Bradycardia (SB) 10/14 LB, 1/07kg Use Asystole, Vfib, pulseless Vtach, PEA (Different dose & Route for anaphylaxis) VF, asystole, PEA, pulseless Vtach Symptomatic bradycardia SVT Metabolic acidosis associated with cardiac arrest Opioid overdose Vfib or pulseless Vtach Vfib or pulseless Vtach VFib or Vtach (torsades de pointes) Treat hypocalcemia or hyperkalemia Treatment No treatment – continue to monitor patient Determine cause – may be normal (runners, bearing down) *If symptomatic – Atropine 1mg IVP Pacer 2 Determine cause and remove – Anxiety, pain, exercise *Betablockers Have patient bear down Adenosine 6mg/12mg/12mg Cardioversion Betablocker, calcium channel blocker, digoxin Cardioversion Need long term anticoagulant to prevent blood clots Amiodorone or Lidocaine Cardioversion Defibrillation, CPR, Amiodarone or Lidocaine, Epinephrine Defibrillation, CPR, Amiodarone or Lidocaine, Epinephrine CPR, epinephrine Determine rhythm does not have pulse CPR, epinephrine Sinus Tachycardia (ST) SupraVentricular Tachycardia (SVT) Atrial Fibrillation (Afib) Atrial Flutter Ventricular Tachycardia (VT) with a pulse Ventricular Tachycardia (VT) pulseless Ventricular Fibrillation (VF) Asystole PEA Scenario Data: Dr. Gerber admitted Fred Boron, a 79-year-old yesterday to Memorial 4 East with the diagnosis of pneumonia. Fred has a history of COPD, MI, HTN and a CABG x2. Fred’s cardiologists is Dr. Friedler and his pulmonologist is Dr. Mills. Home medications include: o Lopressor 25mg twice a day o Lipitor 20mg at bedtime o Baby ASA 81mg once a day o Prednisone 20mg twice a day o Albuterol 2 puffs four times a day and as needed o Ventolin nebulizer every four hours Midnight Nurse report: 4738 has stable vital signs, is breathing okay, has an IV running of NS. He has an antibiotic ordered, but it has not come up from pharmacy (I didn’t have time to check on it.). He has been a PIA… on the light all night. Additional information if the students ask, if not they are on their own: On admission: T – 100.8 F BP 150/92 P – 110 (Sinus tach) R – 24 Most recent vital signs: 10/14 LB, 1/07kg 3 T – 101 F BP – 146/88 P – 120 (ST) R – 24-26 Code Status: Not addressed – no advanced directive on chart Oxygen: 2L/NC – pulse ox 89 – 90% Assessment: alert & oriented, restless Skin pink, diaphoretic Breath sounds clear but diminished Productive cough – coughs sputum into tissue Foley catheter drained 200ml dark amber IV of NS at 50ml/hr – infiltrated and didn’t restart it (didn’t have time) Tequin 400mg every 8 hours – needs initiated Last breathing treatment 0400 Activity is up but gets SOB when walking Has BMP and ABG’s ordered this AM but not back yet Yesterdays labs in the chart Sequence of Events: #1 Baseline Assessment Patient Status Desired Actions o Ask pertinent health history questions o Head to toe assessment o Start IV o Initiate antibiotic after checking for allergies o Assess pulse ox o Assess oxygen for correct dosage o Look for AM labs (not back yet) Truck Driver with Code blue Pulseless VT Overlay 10/14 LB, 1/07kg 4 Transition Vital signs: T – 101F P – 124 R – 28 O2 sat. – 85% Monitor – sinus tach (Monitor leads pulled off can the students reapply correctly) Lung sounds – wheezes SOB noted while at rest and talking C/O being tired Cough persists with productive sputum of greenish yellow Oxygen @ 2L/NC (If the students would like to increase the oxygen did they consider the patient has a history o Notify the physician as needed o Assess monitor for vital signs and EKG rhythm o Assess respers o O2 Sat o Focused assessment o AM labs back – compare the with previous labs o call the physician to relay assessment data and labs #2 Rhythm change 10/14 LB, 1/07kg 5 of COPD) - Note how long it takes for the student to see the rhythm change - Vital signs BP – 149/108 P – 123 R – 27 T – 101.2F - Pulse ox – 86% - Skin slightly cyanotic - should note the potassium level is 3.3 - Notify the physician for orders MD. orders: 1. Routine emergency treat orders 2. Give an additional breathing treatment now 3. Tylenol 650mg po now and every 6 hours for temp > 101F 4. Lidocaine 75mg IV push stat 5. Add 20mEq KCL to current IV fluid (need to know if have enough fluid left in bag to add this amount of KCL – what are the KCL rules) 6. BMP in A.M. Telephone order read back should be used Allow students to complete 2 ,4 ,5 before starting into the code section o Note the - Student should note patient is not pulseless VT responding - Call code blue o Assess (know number or monitor push the blue button) screen (VT) - Retrieve the code o Start CPR cart o Call the - Start CPR and code attach the AED while o Initiate waiting for the code ACLS team to arrive. (Who protocol comes – RN from 4 o Handle east, RN MICU, family Respiratory therapy, members if Medical resident as present assigned, Unit or Division Director, RN/LPN caring for the patient, Anesthesia as needed) - Follow ACLS protocol 1. Give oxygen & Attach AED 2. determine if a shockable ryhthm #3 Pulseless VTach 10/14 LB, 1/07kg 6 3. If (VT or VF) 4. Give one shock biphasic 120 – 200j Immediately Resume CPR – 5 cycles (don’t stop CPR only for shock) 5. check rhythm – if shockable them give one more shock 6. Resume CPR (5 cycles) Epinephine 1mg IV every 3-5 minutes throughout Code OR Vasopressin 40units IV to replace the first 2 doses of epi 7. check rhythm 8.if shockable Shock Resume CPR . Consider Antiarrhythmics – amiodarone 300mg IV x1, then an additional 150mg x1 OR lidocaine 1 – 1.5mg/kg x1 then 0.5mg - .75mg 3doses max or (3mg/kg) Consider Magnesium loading dose 1-2g IV for torsades de pointes After 5 cycles of CPR return to number 5 #4 Course V – Fib 10/14 LB, 1/07kg o Assess monitor and note change o Continue ACLS protocol 7 - monitor changes to V-Fib - Same protocol as above o Assess Physician orders: monitor & 1. Lidocaine @ note changes 2mg/min o Initiate MD 2. If patient orders allergic to o Call for bed Lidocaine in CCU give o Prepare for Bretylium Transport 3. Transfer to CCU - Read back orders - Set up lidocaine - move to the CCU #5 ST with 25% PVC’s Debriefing: 1. If unable to insert IV lines what are your options? a. central line insert b. medication via endotracheal tube 2. When would atropine be given? a. for symptomatic bradycardia ONLY 3. When would bicarbonate be given? a. If metabolic acidosis 4. How would you transport patient to ICU? What do you need? 5. What were your thoughts or feelings during the CODE? (anxious, nervous, comfortable with interventions etc.)? 6. Did the group work as a team to support one another and enable best outcome for patient? Was communication clear and professional? 7. What symptoms did the patient present that alerted you to a possible code situation? Is there any actions the nurse could have taken to prevent the code? 10/14 LB, 1/07kg 8