Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
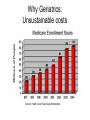
Precise Evaluation of the Geriatric Patient Adult in the ED: An interactive case series Kevin Biese MD, MAT Kristen Barrio MD Nikki Waller, MD Ellen Roberts PhD, MPH Jan Busby-Whitehead, MD With Support from The Donald W. Reynolds Foundation, John A. Hartford Foundation & American Geriatrics Society © The University of North Carolina at Chapel Hill, Center for Aging and Health The Overview • Overview Geriatric Emergency Medicine (GEM) • The Precise Evaluation game • Frequent GEM pitfalls – Trauma, delirium, triage, care transition, abdominal pain • Wrap up with key GEM take home points • Discussion Why Geriatrics: Phenomenal growth Why Geriatrics: Unsustainable costs Precise Evaluation: The game Kevin Biese MD, MAT Kristen Barrio MD Nikki Waller, MD Ellen Roberts PhD, MPH Jan Busby-Whitehead, MD Center for Aging and Health With Support from The Donald W. Reynolds Foundation, John A. Hartford Foundation & American Geriatrics Society © The University of North Carolina at Chapel Hill, Center for Aging and Health Precise Evaluation: The answers Kevin Biese MD, MAT Kristen Barrio MD Nikki Waller, MD Ellen Roberts PhD, MPH Jan Busby-Whitehead, MD Center for Aging and Health With Support from The Donald W. Reynolds Foundation, John A. Hartford Foundation & American Geriatrics Society © The University of North Carolina at Chapel Hill, Center for Aging and Health Acute Abdominal Pain in the Elderly: Significant Mortality and Morbidity • ≥65 years old (yo) and come to the ED with acute abdominal pain – 50% admission – 33% surgery – Mortality 10% (similar to ST elevation myocardial infarction) Kizer KW, Am J Emerg Med 1998; 16: 357-62. Geriatric Abdominal Pain: Different Causes Final Diagnosis Biliary Tract Nonspecific Age <50 6% 40% Age > 50 21% 16% Appendicitis Bowel Obstruction Pancreatitis 32% 2% 2% 15% 12% 7% Diverticular Cancer Hernia Vascular <.1% <.1% <.1% <.1% 6% 4% 3% 2% Gyn Other 4% 13% <.1% 13% Tintinalli J, et al. Emergency Medicine: A Comprehensive Study Guide. 6th ed. New York: McGraw-Hill; 2000. Case 1 Ultrasound Case 1: Cholecystitis • #1 abdominal surgical emergency in elderly • Incidence increases with age • Often only epigastric pain (foregut innervation is visceral) • LFTS often not helpful • Ultrasound is study of choice Cholecystitis: Are LFTs Helpful? Trowbridge RL. JAMA. 2003; 289(1): 80-86. Case 2 Insert picture of CT scan with mesenteric ischemia Case 2 Insert picture of CT scan with mesenteric ischemia Case 2: Mesenteric Ischemia • Classically pain out of proportion to exam • Risks include atrial fibrillation, hypercoagulable, low-flow, increasing age • Arterial (usually) or venous • Embolus or thrombosis • Sometimes “intestinal angina” • Usually superior mesenteric artery • Multi-detector CT scan 77-90% sensitive • Elevated lactate is a late finding (check >1 time) Newman TS. AmSurg. 1998; 64: 611-16. Horton KM. Radiographics. 2002: 22; 161. Emedicine 2006 Case 3: GI Bleed - Syncope • DO A RECTAL EXAM Case 4: Fall/Pain Management • Pain related complaints are common among elderly patients – Approximately 7 million US ED visits/year are due to acute pain in patients >65 • Persistent pain has been associated with functional decline, falls, death Platts-Mills TF, Esserman DA, Brown DL, Bortsov AV, McLean SA. Ann Emerg Med. 2012 Aug;60(2):199206. Case 4: Fall/Pain Management • Studies have reported that pain is undertreated in elderly patients – One recent analysis showed >1/2 of all patients >75, 1/3rd with severe pain that presented with a pain related complaint were not given analgesic – Patients >75 approx 19% less likely to receive pain meds than pts aged 35-54 years Platts-Mills TF, Esserman DA, Brown DL, Bortsov AV, McLean SA. Ann Emerg Med. 2012 Aug;60(2):199-206. Case 4: Fall/Pain Management • Strategies for treating pain – Involve patient and the family in treatment options – Consider non-pharmacologic approaches – Scheduled acetaminophen – Start low and titrate slow with opioids and avoid preparations with acetaminophen – Anticipate side effects ( especially constipation, nausea, tiredness) if going to prescribe opioids – Ensure close follow-up Kapo JM. Persistent Pain. In: Pacala JT, Sullivan GM, eds. Geriatrics Review Syllabus. 7th ed. New York: American Geriatrics Society; 2010 Geriatric Trauma: Mechanisms • Falls - most common – Balance, strength, vision – Often worse than they seem • MVC – most fatal – Judgment, vision, reaction times – Crash fatality rates are much higher • Burns- 1/5 of all burn unit admissions – Mortality estimate = age + % burn Geriatric Trauma: Complicating Factors • Past medical history – Cardiac and pulmonary disease limit physiological response to stressors – Vital signs are difficult to interpret • Medications – Anticoagulant use – Beta blockers • Cause of the event – MI, syncope, stroke, hypoglycemia, suicide attempt Geriatric Trauma: Triage • Geriatric trauma patients are under-triaged pre-hospital, in violation of paramedic protocols • Improved outcomes with lower threshold for trauma activation for geriatric trauma • Focus on trauma triage! Ma, J Trauma, 1999 Demetriades, 2002 Rib Fractures If >65 with 3 or more rib fractures, admit; if >6 rib fractures, ICU Bergeron, J Trauma 2003 Case 4 • What would have compelled you to obtain a head CT? Insert picture of CT scan with subdural hematoma Warfarin and Elderly ICH • Blunt head trauma on warfarin no symptoms, 7-14% with ICH • Beware DASH (Delayed Acute Subdural Hematoma) – consider observation even if negative head CT (especially INR >4) • Patients frequently supra-therapeutic INR – 11% with INR >5 =Check INR • Risk of spontaneous ICH on warfarin 0.35.4% • Frequent medication interactions – (>700 interactions including fluoroquinolones) Callaway, Emerg Med 2007 Aggressive Warfarin protocol 82 patients/ 19 with ICH Initiation of reversal from 4.3 to 1.9 hours Mortality from 48% to 10% Ivascu, J Trauma 2005 Case 5:Delirium 2° ASA Toxicity • Delirium: – Acute onset with fluctuating course – Need to know the baseline • Call the referring facility – Vital sign of older adults Case 5: CAM http://jajsamos.files.wordpress.com/2011/03/cam-delirium-flow-chart.jpg Mini - Cog Rapid assessment cognitive impairment Less subject to language and education Detects mild impairment www2f.biglobe.ne.jp Benzodiazepines for Acute Agitation • Avoid entirely if possible – see Beers Criteria Table 2 – Appropriate if being used to treat alcohol withdrawal • May cause a paradoxical reaction in the elderly – Increasing agitation and anxiety – May lead to prescribing cascade (ie. antipsychotic use) • Long-acting – Prolonged half-life in older adults (days) • Benzodiazepines are lipophilic – Sedation, aspiration, delirium – Increased risk of falls and fractures Beers criteria Table 2: JAGS 2012 Apr;60(4):616-31 Case 5: Treating agitation Consider non-pharmacologic treatment first Rule out delirium Avoid physical restraints Use oral route if possible Use lowest effective dose and repeat if needed (60 min) Benzodiazepines within 1-2 hours of IM olanzapine are contraindicated Avoid benzodiazepines unless seizures or withdrawal Cardiac history required with IM ziprasidone Increased risk of QT prolongation with haloperidol given IV Reorientation Modify environment Attend to basic needs Risperidone ≤ 1 mg PO Olanzapine 2.5-5 mg PO/IM (NO BZDs with IM) Quetiapine ≤ 50 mg PO Haloperidol 1-2.5 mg PO/IM Ziprasidone 10-20 mg IM Haloperidol 0.25-1 mg IV Lorazepam 0.5-1 mg (PO, IM, IV) Tintinalli J, et al. Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York: McGraw-Hill; 2014 Case 5: ASA Toxicity • Tinnitus, N/V, confusion, pulmonary edema • Mixed metabolic acidosis and respiratory alkalosis • Chronic toxicity more common in elderly and often missed • Possible etiology of delirium Take Home Points • GEM is its own subspecialty with unique and evolving knowledge base and skills • To avoid pitfalls – Be wary - don’t under triage (particularly trauma and always “blood thinners”) – Acute abdominal pain is often life threatening – Utilize Mini Cog and ICU CAM – Delirium means something is wrong – Treat pain, intelligently – Treat agitation, gently – Prepare for care transitions • You can be an excellent physician by taking extraordinary care of your older patients