Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
H. HOSSEINI MD
Airway anatomy differences
Airway anatomy differences
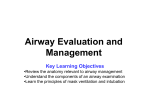
Airway Shape
Adapted from
Walls et al.
Manual of
Emergency
Airway Management.
2nd Ed. 2004.
2- Relatively Larger Tongue:
Obstructs airway
Obligate nasal breathers
Difficult to manipulate & stabilize with
laryngoscopic blades
4- Differently Shaped Epiglottis
Infant epiglottis ohmega (Ώ) shaped and angled away
from axis of trachea
More difficult to lift an infant’s epiglottis with
laryngoscopic blade
5- Funnel shaped larynx
The only complete ring
Narrowest part of infant’s larynx is the cricoid cartilage:
Tight fitting ETT may cause edema.
Uncuffed ETT preferred for patients < 8 years old
Recently, the concept of the child having a funnelshaped airway with the cricoid as the narrowest portion
of the airway has been challenged. Based on
bronchoscopic images,
Dalal and colleagues (2009) suggest for infants and
children the glottis, not the cricoid, may be the
narrowest portion.
Five Cardinal Anatomical Features
of Infant’s Larynx
1- Higher Larynx
Acute angulation between plane of tongue & plane of
glottis makes exposure difficult ►straight blade
►exaggerated by mandibular hypoplasia (Pierre Robin
syndrome).
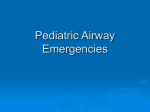
Positioning
Adapted from
Walls et al.
Manual of
Emergency
Airway Management.
2nd Ed. 2004.
3- Anteriorly Angulated Vocal Cords:
The anterior attachment of vocal cords are lower than
posterior attachment ► difficulty in nasal intubations
where “blindly” placed ETT lodges in the anterior
commissure rather than in the trachea.
Respiratory Physiology
Obligate nasal breathers
Immaturity of coordination between respiratory efforts
and oropharyngeal motor/sensory input.
During quiet respiration, the tongue rests against the roof
of the mouth.
Respiratory Physiology
Respiratory Parameters
High metabolic rate (5-8 ml/kg/min)
Tidal volume (6-7 ml/kg/min)
High respiratory rate (40-60 breaths/min)
High alveolar ventilation (130 ml/kg/min)
Lung compliance is less while chest wall compliance is
more than those in adults {reduced FRC and atelectasis}
►PEEP.
Respiratory Physiology
Effect of Edema on WOB
Laryngoscope Blades
Macintosh
Miller
Using The Miller Blade
Better in younger
children with a floppy
epiglottis
Straight Laryngoscope
Blade – used to pick up
the epiglottis
Intubation Positioning
Goal is to align three axes
OA/PA/LA
Medical positioning
Head tilt chin lift
Towels (older = head, younger = shoulders)
Trauma positioning
Manual in-line stabilization
PositioningMedical
vs.
Trauma
Positioning
Intubation Approach
Remember, much different than adults
Externally
Larger head/occiput
Head flexes forward and can obstruct
Internally
Larger tongue
Friable tissues
Different angles and shapes
Airway Differences
Nose
Tongue
Trachea
Cricoid
Airway
Special Techniques for Intubation
Rigid Laryngoscopy
The retromolar, paraglossal, or lateral approach to rigid laryngoscopy
utilizing a straight blade.
ET Tube sizes
Age
kg
Newborn
3 mos
1 yr
2 yrs
12
ETT
3.5
6.0
10
4.5
Length (lip)
3.5
9
3.5
10
4.0
11
12
Children > 2 years:
ETT size:
ETT depth (lip):
Age/4 + 4
Age/2 + 12
Equipment choosing
Other methods for choosing ET tubes
Uncuffed tubes (in mm):
age
4
Cuffed tubes:
+ 4
Uncuffed size - 0.5
Tube Placement
ETT depth – use the black line
(Age in years/2) + 12
ETT internal diameter x 3
Tracheal Tube Sizes
Insufflation Pressure ?
Muscle Relaxants?
Age
Size (mm ID)
Insertion length
(Alveolar ridge)
Preterm 1000g
Preterm 1000-2500g
2.5
3.0
6-9 cm
Neonate-6 Month
3.0-3.5
10 cm
6 Month – 1 Yr
3.5-4.0
11 cm
1-2 Yrs
4.0-5.0
12 cm
Beyond 2 Yrs
age (yrs)/4 + 4
age (yrs)/2 + 12
Techniques to open the Airway
Nasopharyngeal Airway
Size
Hazards: long, bleeding 30%, intracranial placement
Techniques to Open the Airway
Head tilt- Chin lift - Jaw Thrust – Oropharyngeal Airway
Aligning of the Upper Airway Axes
( More than 6 Years Old)
Three-axes theory?
Tracheal Intubation
Laryngoscopic Blade Sizes
Age
Miller
Macintoch
Preterm
0
-
Neonate
0
-
Neonate-2 Yrs
1
-
2-6 Yrs
-
2
6-12 Yrs
2
2
>12 Yrs
3
3
Micro-cuff ETT
More anatomical fit
Sealing at low pressures
More distal position
Greater permeability for nitrous
oxide
For neonates ≤3 kg and infants ≤1
year, ID 3.0-mm
For children 1 to 2 years of age, ID
3.5-mm
For children ≥2 years, ID (mm) =
age/4 + 3.5
Post-intubation croup was 0.4%
(2/500 children)
Endotracheal tubes fabricated without the Murphy eye
are known as Magill tubes,
whereas those that have this opening are called Murphy
tubes.
However, there are potential disadvantages to the
presence of a Murphy eye on an endotracheal tube,
including a tendency for accumulation of secretions and
the possibility that a stylet, catheter, or bronchoscope
may get stuck, requiring the removal of the entire
assembly.
LMA: Reusable Classic, Disposable Unique, ProSeal
Silicone
Softer,
deeper mask
bowl, bite
block,
improves
stability
PVC
Silicone
LMA Sizing
LMA Size
Patient Size
1
Neonate / Infants < 5 kg
1½
Infants 5-10 kg
2
Infants / Children 10-20 kg
2½
Children 20-30 kg
3
Children/Small adults 30-50 kg
4
Adults 50-70 kg
5
Large adult >70 kg
LMA
Used in any age
Easy to place
Few complications
Contraindications:
Gag reflex
FBs
Airway obstruction
High ventilation pressure
Does not secure airway
Following its blind passage through the oral cavity, the
proper seating of an LMA is generally heralded by a
slight rise of the device when the mask’s cushion
is inflated with air. Care should be taken to use the
minimal effective inflation pressure for the cuff, typically
up to 60 cmH2O. The routine use of a manometer is
advocated
The more cephalad and anterior position of the larynx of
a child as compared with an adult has prompted the use
of an alternate insertion technique in children. In this
case, the LMA is inserted with its cushion placed against
the hard palate. The device is then rotated through 180
degrees until the cushion is seated at the laryngeal inlet .
This method for the insertion of an LMA appears to be
especially useful in preschool and young school-age
children.
LMA sizes
Mask size
Patient’s weight
Maximum cuff
volume (ml)
(Least effective
volume)
Largest TT (mm
ID)
1
1-5 kg
4
3.5
1.5
5-10 kg
7
4.0
2
10-20 kg
10
4.5
2.5
20-30 kg
14
5.0
3
> 30 kg
20
6.0, non-cuffed
Causes of Difficult Airway
Congenital Anomalies
Tumors
Infection
Musculoskeletal Problems
Loose or missing teeth.
Size and configuration of palate.
Size and configuration of mandible (side view).
Location of larynx in relation to the mandible.
Presence of inspiratory stridor :epiglottitis, croup,
extrathoracic foreign body.
Both inspiratory and expiratory stridor: aspirated foreign
body, vascular ring, or large esophageal foreign body.
Prolonged expiration: lower airway disease?
Baseline oxygen saturation in room air.
Bilateral microtia (ear deformity easily notable) is
associated with mandibular hypoplasia & difficulty in
visualizing the laryngeal inlet (42%) & with unilateral
microtia (2.5%).
Are there congenital anomalies that may fit a recognizable
syndrome? The finding of one anomaly mandates a search
for others.
microtia
Musculoskeletal Problems
Ankylosis of jaw, cervical spine
Unstable or dislocated cervical vertebrae
Wired jaw
Cervical cord tumor
Halo traction apparatus
Facial trauma, fractures, laceration, burns
Evaluation of the Upper Airway
(Diagnostic Testing)
X-ray, MRI and CT.
Radiologic airway examination in a child with a compromised
airway must be undertaken only when there is no immediate
threat to the child's safety and only in the presence of skilled
and appropriately equipped personnel able to manage the
airway.
Endoscopic evaluation (flexible fiberoptic endoscopy)
Arterial blood gas analysis (chronic airway obstruction
with respiratory acidosis)
Encephalocele
Bilateral Cleft Palate
Hallermann-Streiff S.
Achondroplasia
Pierre Robin S.
Down S.
Crouzon S.
Seckel S.
Treacher Collins S.
Goldenhar S.
Apert S.
Nager S.
Mucopolysaccaridosis
Type IH (Hurler)
Type 1 H/S (Hurler-Scheie)
Type II Hunter
Type III (Sanfilippo)
Tumors
Cystic hygroma
Hemangioma of tongue, pharynx
Teratoma
Infection
Retropharyngeal abscess
Epiglottitis
Laryngotracheobronchitis
(subglottic croup)
Ludwig’s angina
Adenotonsillitis, abscess, hypertrophy (
obstructive sleep apnea)
Scleroderma
Laryngeal web
I-LMA
Only sizes 3, 4, 5
Same rules and sizing
as LMA
Need special armored
tube for intubation
New similar devices
exist
Leave LMA portion in
place in field
Combitube
Two sizes
Small (4 to 5.5 feet tall)
Regular (over 5.5 feet tall)
Not useful in most kids
Easy to place
Contraindications
Gag reflex
Esophageal disease
Caustic ingestions
FBs/Airway obstruction
Bougie
Replaces stylet
Able to use with poor
view
Feel tracheal rings
Feel carina
Intubate over it
Keep blade in place
Two person technique
Need to practice
Other Toys
Lighted stylet
Flexible fiberoptic
scopes
Rigid fiberoptic scopes
Bullard
Shikani
Video laryngoscopy
Bullard laryngoscope
Optimal External Laryngeal Manipulation (OELM)
OELM is particularly helpful for infants & children with immobile or
shortened necks.
Either by an assistant or the laryngoscopist.
Intubation Guides
Lighted Stylet
Light Wand
TTJV
Glidescope Video Laryngoscope
Ventilation Techniques
Multi-handed Mask Ventilation
Intubation through LMA (Blind)
Fibreoptic Intubation through LMA
Fibreoptic Assisted Intubation
Surgical Airways Cricothyrotomy
Indications (only if >10 years old)
Failed airway
Failed ventilation
Predictors of difficulty
Previous neck surgery
Obesity
Hematoma or infection
Cricothyrotomy Techniques
Open
Locate CTM
Stabilize larynx/prep
Incise skin
Vertical
Horizontal through CTM
Insert spacer/dilator
Closed
Locate CTM
Stabilize larynx/prep
Insert needle
Direct inferiorly
Insert guidewire
Remove needle
Insert cuffed tube
Small skin incision
Check breath sounds
Insert dilators/UC tube
Check breath sounds
Percutaneous Cricothyrotomy
Percutaneous needle cricothyrotomy provides only a
mean for oxygen insufflation and does not reliably
provide adequate ventilation.
If glottic or subglottic pathology is not suspected, LMA
placement to establish ventilation may be
appropriately attempted first.
Cricothyrotomy Complications
Bleeding
Laryngeal or tracheal injury
Infection
Pneumomediastinum
Subglottic stenosis
Retrograde Intubation
Broselow Tape
8 color codes (6-36 kg)
Broselow-Luten Emergency
System
Color-coded bags with equip
Quicker, more efficient
Broselow Tape
Equipment sizes
Airway adjuncts
Intubation equip
Oxygen delivery
Vascular access
Defibrillation
NGT, suction caths
BP cuff
Chest tubes
Foley
Medications
Antiarrhythmics
Arrest medications
Anticonvulsants
Overdose meds
Increased ICP meds
Induction agents
Paralytics
Vasopressors
IV drips
Broselow Tape
THANK YOU