Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lisa A. Lubbers, RN MSN CNP
October 16, 2014
South Dakota Perinatal Association
No
financial interest
1.
• Identify 3 risk factors for
hypoglycemia in neonates
2.
• Identify 3 main factors
impacting blood glucose
after birth
3.
• Identify 3 symptoms of
hypoglycemia in neonates
Primary
fuel for the body-brain has higher
demand for glucose
Brain can’t store adequate amounts in the
form of glycogen like liver, skeletal/cardiac
muscle can
Needs a steady supply
Irreversible neuronal injury can result from
hypoglycemia
Hypoglycemic brain more vulnerable to
damaging effects of ischemia
-sick infants have increased requirements
Glycogenesis-process
by which unneeded
glucose is converted to glycogen for storage
Glycogenolysis-process which causes the
breakdown of glycogen back into glucose
Gluconeogenesis-production of glucose in the
liver by means of nonglucose precursors like
lactate, pyruvate, glycerol, and amino acids
Insulin-secreted
by pancreatic BETA cells in
response to increase in plasma glucose
Decreases blood glucose by promoting glycogen
formation, suppressing hepatic glucose release,
driving peripheral uptake of glucose.
Doesn’t control entry of glucose in the brain or
liver
Glucagon-secreted
by pancreatic ALPHA cells
Promotes glycogenolysis and gluconeogenesis
Opposes effect of insulin by raising blood glucose
Other
counter regulatory hormones-cortisol,
growth hormone, catecholamines
Fetus
stores glucose as glycogen and
develops enzymatic process for mobilization
of stored energy prior to birth
Limited ability to convert glycogen to glucose as
a fetus so relies on placental transfer (facilitated
diffusion) of glucose to meet energy demands
Fetus
is capable of gluconeogenic activity
using lactate if needed to meet metabolic
demands in utero
When the cord is cut enzymes activate the
breakdown of glycogen back into glucose
molecules in the infants body
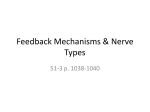
After
Delivery
In Utero
High insulin : glucagon
ratio -Suppresses lipolysis
{subcutaneous fat}
-Glycogen deposition
{
last 30% fetal life}
High glucagon : insulin
ratio
{
catecholamine release}
-Release of glucose
from glycogen
-Term infants have
enough hepatic
glucose for 10 hours
-Induces enzymes for
gluconeogenesis
•Occurs about4-6 h of
age
•Enzymes reach Adult
levels by 1-2 wk-slower
in preterm
Immediate
postnatal drop is physiologic
Balance between hepatic glucose output and
substrate uptake
Hepatic output dependent on adequate
glycogen stores, endogenous gluconeogenic
precursors, normal functioning gluconeogenic
and glycogenolytic systems and normal
endocrine system
At birth, glycogen stores greater than adults,
but 2x greater basal glucose utilization
equals rapid depletion
Hormonal
and enzymatic activities in FETUS
promote anabolism and substrate accretion
Hormonal and enzymatic activities in
NEWBORN provide for glucose homeostasis
after abrupt interruption of maternal glucose
supply-this needs to occur in the course of
seconds!
Metabolized
Production of energy-via glycolysis
several different ways in BODY:
Aerobic Metabolism-1 molecule of glucose yields 36
molecules of ATP for energy
Anaerobic Metabolism-1 molecule of glucose yields 2
molecules
Storage as glycogen
Conversion to gluconeogenic precursors
Brain
:glucose is completely oxidized to
provide 99% of cerebral energy production
Brain is another story-dependent on enzymes and
reactions
GLUT proteins transport glucose across blood brain
barrier into brain cells
During hypoglycemia ketone bodies, lactate,
glycerol, and AA can also be converted to
pyruvate and citric acid cycle—so another source
but not efficient
http://davisdialogues.blogspot.com/2011_08_01_archive.html
Glucose
requirement for a healthy near
term/term infant is 5-8 mg/kg/min (D10W at
80 ml/kg/day gives a GIR of 5.5mg/kg/min)
Many other factors can contribute to
requirements-may need much more
App: glucose infusion rate calculator
GIR (mg/kg/min)= IV rate X %dextroseX.167
wt in kg
Preterm
Infants
Small For Gestational Age (SGA)
IDM
Large for Gestational Age (LGA)
Stressed/Sick Infants
Maternal Medications
Other
causes:
Persistent neonatal hyperinsulinism and
nesidioblastosis (AR caused by regulatory defects
in beta cell function)
Beckwith Wiedemann-unknown cause
Inborn errors of carbohydrate, protein, or lipid
metabolism
Endocrine deficiencies (hypopituitarism)
Several new genetic mutations have been
identified
Iatrogenic –umbilical arterial catheter position
near pancreas (high T 6-9 low L3-4)
The
most common causes:
Preterm
SGA
LGA
IDM
Sick infants
Majority of glycogen stored in 3rd trimester
Available stores rapidly depleted
At TERM 5-8% of liver and muscle weight is
glycogen storage
Immature counter regulatory response to low
glucose concentrations
Preterm, SGA
lack adipose required for ketone production
or unable to mobilize free fatty acids from adipose
Preterm-may not have enzymes required for he
breakdown of glycogen into glucose (glycogenolysis)
Less
than 10% for weight
Causes
Placental insufficiency-chronic stress
Chromosome/genetic abnormalities
Metabolic disorders
Intrauterine viral infection
Multiple gestation
Nutritional status
Maternal chronic illness/stress
Ingestion of drugs/toxins
Some maternal medications
Low
glycogen and fat stores
Inadequate metabolic control
Chronically stressed fetus may use most of
the placentally transferred glucose for
growth and survival
Greater
than 90%
Insulin is a growth hormone-suppresses
glucagon response
Causes hyperinsulinemia r/t:
Undiagnosed GDM (ethnicity, PCOS, family hx of
Type II DM)
Inborn errors
Endocrine disorders
Glucose
crosses placenta/insulin does not
Fetal glucose level 70-80% of mother’s
Infant produces insulin in response to higher
blood sugars
At cord clamping, glucose supply is gone but
insulin production in infant remains elevated
The expected nadir is more rapid than non
IDM infants (1-6 hours)
May take several days to down regulate
insulin production
Fetal
hyperglycemia=increased production
Insulin
IGF-1
Leptin
All
lead to stimulation of fetal growth
Higher
energy needs
Hypoxic infants may rely on anaerobic
glycolysis (inefficient-large amount of
glucose used for low yield)
Aerobic metabolism yields 38 ATP per
molecule of glucose
Anaerobic yields 2 ATP per molecule of
glucose
Therefore, rapidly deplete stores
Current literature does not endorse a particular
number (40,45,47,50)
Symposium on Pediatric Endocrinology 2014->45 for
symptomatic infants and >65 for hyperinsulinism
Blood glucose level can only approximate
cerebral glucose level
All agree treatment for symptomatic infants
Goal is to screen infants in high risk groups-and
intervene appropriately
At risk infants may need to be screened
differently depending on their risk factors
Consider an evidence based algorithm for your
facility
Glucose
goals may vary depending on disease
process, chronological age
Consider goal of 50 mg/dl after 24 hours of
age-especially if high risk category
If requiring high GIR, consider weaning IV for
glucose levels >60 mg/dl
Potential
disruption in bonding/breastfeeding
Repeated heel sticks
Invasive procedures
Uncertainty in what “right” number should
be
Discrepancy in bedside POC and lab glucose
values-POC underestimates
Variation in specimen handling and
obtainment
Infants
at risk may have their first low
glucose concentrations after 3 normal
measurements and even after 24 hours of
age
3 normal measures don’t ensure complete
transition
Consider including 24 hour check into algorithms
Need
to be certain infant maintains normal
glucoses on routine diet for at least 3
feed/fast cycles prior to discharge
Screening for and management of postnatal glucose homeostasis in late-preterm
(LPT 34–3667 weeks) and term small-for-gestational age (SGA) infants and infants
who were born to mothers with diabetes (IDM)/large-for-gestational age (LGA) infants.
Committee on Fetus and Newborn Pediatrics
2011;127:575-579
©2011 by American Academy of Pediatrics
Most neonates are free of symptoms-development of symptoms
can be ameliorated by presence of alternative substrates
Many symptoms can be linked to other issues
General
Abnormal cry
Poor feeding
Hypothermia
diaphoresis
Neurologic
Tremors/jitteriness
Irritability
Lethargy
Hypotonia
seizures
Cardio respiratory
Tachypnea
Apnea
cyanosis
Confirm
with STAT lab blood glucose but
DON’T delay treatment in symptomatic
infant
Tend to be 10-20% higher than whole blood (POC)
values
Follow
up checks are imperative
Should
be feed within 1 hour of age
Screen 30 minutes after feed
Consider gavage feeding if not
nursing/nippling well
Glucose less than 25 mg/dL (birth to 4 hours) or
less than 35 mg/dL (4-24 hours):feed and
recheck 1 hour after feeding
If still less than 25 or 35:treat with intravenous
glucose infusion and/or 2ml/kg D10W bolus
D10W at 80 ml/kg/day give GIR of 5.5 mg/kg/min
Merits of bolus are debatable, may stimulate insulin
and this may pose risk for rebound hypoglycemia
Goal: 40-50 mg/dL
If hyperinsulinism is suspected consider insulin
level, serum ketone bodies, and free fatty acids
to confirm diagnosis-if persistent hypoglycemia
beyond 24 hours of age
Infants
with hyperinsulinemia may require
>12 mg/kg/min IV glucose to maintain
euglycemia!
Central IV access if using >12.5% dextrose
Worry about fluid overload
Weaning
Stable glucose 12-24 h
Follow preprandial glucose
Decrease infusion rate 10-20% each time glucose
>50-60 mg/dl
Hydrocortisone
Decreased peripheral utilization
Stimulates gluconeogenesis
? Consider when needing >15 mg/kg/min
Glucagon
Rapid rise in glucose
Must have adequate glycogen stores (not premies or
SGA)
Temporizing measure
200 mcg/kg IV, SC, IM
Response within 20 min-1 hr
Lasts up to 2 hours
Watch for rebound hypoglycemia
Diazoxide-inhibits
secretion of insulin
Treatment of persistent (more than a few days)
or severe hypoglycemia d/t hyperinsulinism
Positive response usually 48-72h
Sodium and fluid retention is common
Somatostatin
(octreotide)-inhibitor of growth
hormone, glucagon, and insulin
Pancreatectomy
Sugar Babies Study-published 9/2013
Randomized, double blind, placebo controlled
Stratified by maternal diabetes and birth weight
Twins assigned independently
Placebo was carboxymethyl cellulose gel
Large enrollment group (514)-242 became
hypoglycemic and were randomized
New Zealand
40% dextrose gel with and without feeding
Focus on at risk infants
35 weeks or older
48 hours of age or less
IDM
SGA
LGA
Keep
mom and baby together
Potentially no interruption in breastfeeding
Decrease use of formula
Easy to administer
Low cost
BG
measurements at 1h, q3-4h ac for 1st 24 h
then q 6-8h ac for next 24 h
Continuous glucose monitor placed SQ as
soon after birth as possible and remained for
at least 48h or up to 7days until
hypoglycemia resolved
Breast fed (or syringe fed expressed BM)
Formula fed offered up to 60 ml/kg/day 1st
day and 90 ml/kg/day on 2nd day
Dry
baby’s mouth with gauze
Squirt a small amount of dextrose gel into a
small cup
Using a syringe draw up 0.5 ml/kg (200
mg/kg) of gel
Using a gloved finger dispense ½ the dose
onto the buccal mucosa of one cheek and
massage thoroughly
Repeat with the other ½ dose in the other
cheek
Encourage the infant to feed
Blood
glucose checked 30 min after
administration
If continued hypoglycemia repeat
If reoccurrence treat again, up to 6 doses of
gel in 48 hours
Primary outcome-treatment failure
Blood glucose less than 47 mg/dL 30 min after the
second of 2 doses of gel
Secondary outcome
Admission to NICU
Frequency of breastfeeding
Volume of breast milk/formula
IV dextrose
Dextrose gel
Method of feeding at 2 weeks
Incidence of rebound or recurrent
hypoglycemia(glucose <47mg/dL after successful tx)
Time to achieve glucose >47 mg/dL
Duration of glucose < 47 mg/dL
Infants
in the dextrose gel group less likely
to be admitted for hypoglycemia
Treatment babies less likely to receive
additional dextrose
Rebound hypoglycemia uncommon and
similar in frequency in both groups
Recurrent hypoglycemia less common in
babies in the dextrose gel group
Total duration of low glucose concentrations
not significantly reduced with dextrose gel
Treatment was well tolerated
No serious adverse events
Treatment more effective than feeding alone for
reversal of hypoglycemia in at risk late preterm and
term babies in the first 48 hours
Babies who received dextrose gel less likely to be
admitted to NICU for management of hypoglycemia,
to receive additional dextrose gel or formula feeds,
or to be fed formula at 2 weeks of age
Dextrose gel didn’t increase the risk of rebound or
recurrent hypoglycemia
Initial concern for dextrose gel adversely affecting
breastfeeding, but this wasn’t demonstrated
Dextrose gel should be considered for first line
management of late preterm and term hypoglycemic
babies in the first 48 hours of life
Dextrose gel can be a useful ADJUNCT in the
evaluation and management of hypoglycemia
Multidisciplinary
team-pediatricians,
neonatologists, nurse practitioners,
dieticians, lactation consultants, nursing,
pharmacists
Algorithm provides GUIDELINE
Asymptomatic Infant With Risk
Factors
•POCT at one hour >45 continue
feeds and check 2 additional
prefeed POCT
•POCT at one hour <45- apply
dextrose gel and feed again
(breast or formula supplement)
Initiate feed
within 1 hour
2 hour serum
blood glucose
•If <20 apply dextrose gel
and feed immediately, plan
for other intervention
•21-44 apply dextrose gel and
feed immediately recheck
serum and POCT 30 min
after feed
•>45 continue feeds and
check POCT prefeed x 2
•On all at risk infants
•If less than 50 supplement 2040 ml every feed and obtain
prefeed POCT.
24 hour
check
Symptomatic Infant
•Apply dextrose gel and
feed immediately
•If unable to feed apply gel
while placing IV
<45
IV fluids
•D10W at 80 ml/kg/day
•Consider 2 ml/kg bolus
•Every 30 min-1hr until
stable
•May need increasing GIR
•May need supplement if
unable to maintain POCT
•Follow at 24 hours no
matter what
POCT
Glucose
is an important fuel
Several reasons why infants are at risk
No uniform consensus on definition
All agree to treat symptomatic infants
Most important to have a uniform strategy
at your facility
New adjunct-dextrose gel
Kris
Karlsen-STABLE program
Carmen Henke, RN NNP-BC
[email protected]
American Academy of Pediatrics (2011). Clinical Report: Postnatal
Glucose Homeostasis in Late Preterm and Term Infants. Pediatrics.
127(3)575-579.
Arya, V.B., Senniappan, S., Guemes, M., Hussain, K. (2014). Neonatal
Hypoglycemia. Indian Journal of Pediatrics. 81(1):58-65.
Gardner, S.L. et al.. Merenstein and Gardner’s Handbook of Neonatal
Intensive Care. 7th edition. 2011:Mosby
Harris, D.L., Weston, P.J., Signal, M., Chase, J.G., and Harding, J.E.
(2013). Dextrose gel for neonatal hypoglycaemia (the Sugar Babies
Study): a randomised, double-blind, placebo-controlled trial. The
Lancet. 1-7. doi.10.1016/s0140-6736(13)61645-1.
Hawden, J.M. (2013). Definition of neonatal hypoglycemia: time for a
rethink? Archives of Disease in Childhood Fetal and Neonatal Edition.
98:F382-383.
Karlson, K.A. (2013). The S.T.A.B.L.E. Program: Pretransport/Postresuscitation Stabilization Care of Sick Infants Guidelines for Neonatal
Healthcare Providers. 6th ed.
McGowan, J.E. (2006). Neonatal Nutrition and Metabolism (2nd ed).
(2006). Cambridge University Press.
Rozance, P.J. (2014). Update on neonatal
hypoglycemia. Current Opinions in Endocrinology
Diabetes and Obesity, 21:45-50.
Rozance, P.J. (2012). Editorial: Neonatal
Hypoglycemia-Answers, but More Questions.
161(5):775-776.
Tin, W. (2014). Defining neonatal hypoglycaemia: A
continuing debate. Seminalrs in Fetal and Neonatal
Medicine, 19:27-32. doi.org/j.siny.2013.09.003.
UpToDate (2014). Neonatal Hypoglycemia. Retrieved
January 16, 2014 from
http://www.uptodate.com/contents/neonatalhypoglycemia
Verklan, M.T. and Walden, M.(4th ed.). Core
Curriculum for Neonatal Intensive Care Nursing.
Saunders Elsevier (2010).