Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
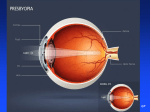
Fitting & Evaluating the New Soft Multifocals Wm. Edmondson, MAT, O.D., FAAO & Latricia Pack, O.D., FAAO Northeastern State University, Oklahoma College of Optometry 918-456-5511 X 4015; [email protected] Abstract This presentation provides clinicians with guidelines for the most successful techniques in fitting the new generation of hydrogel & GP contact lens multifocals. Discussion of popular, recent multifocal designs are included. Objectives 1. To utilize universal principles in fitting most hydrogel & GP CL multifocals. 2. To identify & select patients with the most appropriate presbyopic corrections 3 To become acquainted with the basic “out-of-phoropter” techniques to evaluate the performance of the multifocal contact lens. 4. To become familiar with techniques for utilizing patient feedback to modify the distance & add power of the lens. 5. To incorporate the most current presbyopic research & contact lens options to maximize patient success Outline A. Using the New Generation of Multifocal Contact Lenses–> Simultaneous Vision 1. 2. 3. 4. B. PureVision / Soflens Multifocal - Bausch & Lomb Focus Progressive / Focus Dailies Progressive - CIBA Vision Proclear/ Freq. 55 Multifocal – CooperVision Toric Hydrogel Multifocals Multifocal Terms 1. 2. 3. 4. Binocular Multifocal: Multifocal on both eyes; Binocular Balanced Enhanced Multifocal: Multifocal on both eyes; One eye enhanced for either dist.or near Modified Monovision: Multifocal on one eye; single vision (dist.or near) on other eye Standard Monovision: SV lenses on both eyes; One for distance and one for near C. Universal Truths to maximize success in presbyopic fitting 1. 2. Don’t rely on current glasses (or SV CL) Rx Learn how to Evaluate spectacle Rx and astigmatism a. Selecting patients: Initial “suggested” for maximum early success Significant Distance spherical spectacle Rx –> greater than +/- 1.00D Yes ---------> RGP or Hydrogel Multifocal No ----------> Alternatives to multifocals: - Multifocal in one eye only - Traditional Monovision or near lens only - Distance contact lenses plus reading spectacles - Other b. Refractive cylinder: 1. 0.75D or less --------> Soft Multifocal or RGP Multifocal 2. 0.75D -2.50D ------ -> RGP/ Soft Toric Multifocal 3. Other options: D. Universal Truths to maximize success in presbyopic fitting (Cont.) 3. Pre-fitting Consultation a. Evaluation: Visual needs, & Ocular health & Physical characteristics b, Pre-fitting Consultation: Patient expectations c. Protocol: Review findings make recommendation d. Emphasize correcting presbyopia (not fitting this new bifocal) 4. Selecting, Evaluating & Modifying the Initial Lenses on the Patient a. b. Identify patient’s Dominant eye Selecting the distance power for the initial multifocal trial lens 1. Distance spectacle correction -----> Vertexed to corneal plane a. Sphere only ---------- gas perm. multifocals b. Sphero-cyl equivalent -- most current hydrogels 2. Diagnostic distance lens power Rx-> a. Make sure exactly corneal plane Rx or more (+) b. If more minus –> patient will use some of the (+) “add power” for distance c. Use Free lenses, Trial frame, or Flippers <------> Out of the Phoropter 1. Normal “room” illumination ( Avoid mirrored rooms if possible) 2. Evaluate Binocularly -----> Both eyes open —> “How do things look” a. Dist. ---> Initially use whole chart with 20/30 as bottom row b. Near ---> use magazines or newspapers: 20/40 to 20/30 print d. Time to let lenses settle & motor activity: Have patient walk out of exam lane k 5. Problem Solving: Modification based on Patient Feedback a. Add trial lenses binocularly until you obtain the best balance between: Distance vision vs. near vision 1. Add (+) O.U. ------------> if clarity needed at near 2. Add (-) O.U. ------------> to enhance distance vision 3. Maximum plus to maximum acuity b. “Cannot binocularly make distance sharp without losing near vision” 1. Monocularly add minus to dominant eye, a. do not occlude non-dominant eye while testing b. typically -0.25D to -0.50D c. Both eyes still have a dist. and near Rx; “Enhancing” distance in one eye 2. Use the next lower add in the dominant eye; Enhances distance clarity: c. “Near vision not good, but distance isn’t bad” 1. Monocularly add plus to non-dominant eye a. Both eyes still have a dist. and near Rx b. “Enhanced” vision at near in non-dominant eye 2. Monocularly use the next higher add in the non-dominant eye d. Monocular addition of 0.25 - 0.50D power typically all that is needed ---> success vs. failure 6. Insert a. b. c final lenses to be dispensed Binocular acuity: for you and patient Monocular acuity: for medico-legal documentation in chart Reconfirm appropriate lens movement with slit-lamp 7. Patient education: Let the patient know a. You will be working with them to “fine tune” their Rx to meet problems and there may yet be lens changes b. There may be an adaptation period (including slight shadowing of letters) c. Night driving, be cautious (halos around lights) 8. Return to office in 3 about days: Long enough to evaluate vision, short enough to prevent frustration. Use patient feedback to modify CL prescription 9. Patient Feedback including Hx & requirements a. Patient displeased with “Crispness” of vision with soft -> RGP Multifocals b. c. d. e Health issues with hydrogel lenses ---------------> RGP Multifocal Pt displeased with comfort of RGP’s --------------> Soft Multifocal Part time wearer -----------------------------> Soft Multifocal Alternatives Specific Lenses: Frequency 55 Multifocal: -------› methafilcon A (group 4, 55%, Dk 18.8) & Proclear Multifocal ----------- omafilcon A (group 2, 62% Dk 34.0 1. 2. 3. Design: Center near progressive multifocal for dominant (dist. enhanced eye) & center near progressive multifocal for non-dominant (near enhanced eye) Parameters a. Three add powers: +1.00, +1.50, +2.00, +2.50 a. Distance Rx: +4.00 to -6.00 dist power (use vertexed spherical equiv. power) b. Other: 8.7mm b.c. / 14.4 dia / monthly replacement: 6-pack For Rx’s a. for near: between adds round down to lower add b. for dist: with sphero-cyl equivalent between to 0.25 powers -> more minus PureVision / Soflens Multifocal 1. 1. 2. 3. 4. 5. (Bausch & Lomb) Dist. Rx: +6.00D to -10.00D Add Powers: Low (up to +1.50); High (+1.75 to +2.50) Base Curves: 8.5mm or 8.8mm , Dia.: 14.5mm Polymacon / 38% / Group 1 / Dk 8.4, 2 wk replacement Initial Lens Selection a. Distance Power: Vertexed spherical-equivalent b. Base Curve: » 8.5mm base curve c. Add: i. Low add +1.50 or less OU ( Early presbyope under 50) ii. +1.75D to +2.25D add: Enhanced Multifocal - Dominant Eye --› Low Add ; Non-Dominant Eye --› high Add iii. +2.50 add & up High Add O.U. New Bausch & Lomb PureVison Multifocal Focus Progressives & Focus Dailies Progressives: (CIBAVision) 1. 2. 3. 4. 5. Single progressive add up to +3.00 / aspheric, center near design One trial power designated on box for distance and near Focus Progressives: –---------------> vifilcon A (group 4, 55%, Dk 16) a. Two base curves: 8.6mm/8.9mm with a 14.0 dia b. Power Availability: +6.00 to -7.00 c. One month replacement ( option of 2 weeks): available as 6-pack Focus Dailies Progressives: -----------> nelfilcon (group 2, 69%, Dk 26) a. Base curve: 8.6 with a 13.8 dia b. Power Availability: +5.00 to -6.00 c. Daily replacement: available as 30- or 90-pack Initial Focus Progressive lens selected from: Trial CL Power = Spherical Equivalent Distance Power + 1/2 the add power Example: Spectacle Rx: -3.00 dist / +1.50 add —> Trial = (-3.00 plus +0.75D) –> -2.25D a. b. Focus Progessive, “Initial Power Selection Table” 1. Uses distance BVA spectacle Rx ( —> spherical equivalent) 2. Table vertexes the sphero-cyl Rx to spectacle plane 3. Spectacle add 4. How good is the “Initial Power Selection Table “ ??? Or the use of the following Focus Progressive equation: Other Alternatives 1. Soft toric multifocals b. Cooper UltraVue Toric c. CIBA Progressive Toric i. Essentials Soft Toric D Others