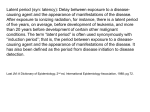
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cancer Epidemiology An Introduction • • • • • • The Epidemiologic Perspective Aims of Cancer Epidemiology Methods of Epidemiology Historical Perspective and Examples Contemporary Studies The Future Epidemiology • “Distribution and determinants of disease frequency in human populations” – Humans: not laboratory animals, cells – Populations: not individuals, case series – Frequency: Quantification of occurrence and risks – Distribution: Descriptive epidemiology – Determinants: Analytic epidemiology Aims of Cancer Epidemiology • Uncover new etiologic leads – study of the distribution of cancer – quantify the risk associated with different exposures and host factors • Promote insights into the mechanisms of carcinogenesis • Assess efficacy of preventive measures • Investigate predictors of survival Methods of Cancer Epidemiology • Descriptive Studies – – – – Incidence, mortality, survival Time Trends Geographic Patterns Patterns by Age, Gender, SES, Ethnicity • Analytic Studies – Case-control – Cohort Challenges to Interpretation – Observational vs. Experimental Design – Cancer “clusters” – Study Design and Conduct • Study Size • Biases: Misclassification, confounding, selection – – – – Exposure assessment important Epidemiology and “strong” and “weak” effects Impact on a population level Replication critical Cancer Epidemiology Sources • US SEER Registry System • IARC International Registries • State/Hospital Registries • Etiologic Clues – “Alert” Clinician – Experimental Studies Cancer Epidemiology Historical Perspective • 1700: Italian Physician noted breast cancer more common among nuns • 1775: Percivall Pott noted scrotal cancer more common among chimney sweeps • 1700s: pipes and lip cancer, snuff and nasal cancer • 1842: Uterine cancer in Verona, Nuns vs. others • 1800s: Occupational cancers Cancer Epidemiology Historical Perspective • • • • • • • • Tobacco and Lung Cancer Asbestos and Lung Cancer Leather Industry and Nasal Cancer Dyes and Bladder Cancer Ionizing Radiation and Many Cancers DES and Vaginal Adenocarcinoma EBV and Burkitt’s Lymphoma HPV and Cervical Cancer Attributable Risk • Environmental 5% • Lifestyle 45% • Occupational 4% • Pharmacologic 2% • Biologic (viruses) 4% Cancer Epidemiology Current/Future Topics • • • • • • • Infectious Agents Obesity Physical Activity Diet Hormones Immunologic Factors Inherited Susceptibility (Polymorphisms) Cancer Epidemiology Current/Future Topics • • • • • • • Tumor (somatic) Alterations Cancer Classification Biomarkers of Exposure/Effect Improved US Registry System Study Pooling Epidemiologic/Statistical Methods Survivorship Head and Neck Cancer as a Model for Gene-Environment Interaction Andrew F. Olshan, Ph.D. Departments of Epidemiology and Otolaryngology/Head & Neck Surgery University of North Carolina Epidmiology of Head and Neck Cancer • Squamous Cell Carcinoma of oral cavity, pharynx, larynx • One of the 10 most frequent worldwide (3rd among males) • Oral (10.1 /100,000) Males (15.1) Females (5.9) Blacks (12.3) Whites (10.0) Larynx Males (6.9) Females (1.4) Blacks (6.6) Whites (3.9) • 40,100 new cases/year in US 11,800 new deaths • Survival- Five-year 54% oro-pharyngeal, 65% laryngeal – Blacks (34%) Whites (56%) SCCHN as a Model System • KNOWN Risk Factors • Molecular Markers – – – Tumor Suppressor Genes Oncogenes Virus • Other Characteristics – – Preneoplastic lesions Recurrence/second primaries Exposure Biologically Effective Dose Internal Dose DNA Adducts Agent or Metabolites SUSCEPTIBILITY Preclinical Biologic Effect Mutation Oncogenes Tumor Suppressor Preneoplastic Lesions Genetic/Metabolic DNA Repair Nutritional Status Immunologic Status CLINICAL DISEASE Tobacco and Alcohol 100 Alcohol Drinks/Wk 37.7 <1 5 to 14 15 to 29 30+ Relative Risk 10 23.8 7.9 5.80 1 NSmoker From Blot 88 1 to 19 20 to 39 Cigarettes Per Day (20+ years) 40+ Research Question – Do polymorphisms of activation, detoxification, and DNA repair genes confer a differential risk of head and neck cancer in individuals with exposure to tobacco and alcohol? Carolina Head And Neck CancEr Study • Population-Based NC Study – 46 Counties (Central/Eastern NC) – Rapid Case Ascertainment (1-2 months) – Physician Consent – 1,700 cases (4 yrs) • Whites (1330), blacks (402), <50yrs (225) • Oral (779), Pharynx (364), Larynx (589) 46 County Study Area Vance Rockingham Person Caswell Granville Halifax Forsyth Guilford Alamance Franklin Orange Nash Davie Durham Edgecombe Davidson Iredell Randolph Chatham Wilson Wake Catawba Rowan Pitt Johnston Lincoln Greene Lee Cabarrus Montgomery Harnett Stanly Gaston Moore Wayne Lenoir Craven Mecklenburg Cumberland Union Sampson Duplin Onslow Pender Brunswick New Hanover CHANCE STUDY – DMV Controls – Phone number search, letter, phone call – Frequency Matched (age, race, gender) CHANCE STUDY – In-person interview • • • • • • • Demographics Smoking/Alcohol Hx Diet (74 items NCI DHQ) Oral Health Medical Hx Screening Hx Family Hx of Cancer – Blood Draw (3 tubes) or Mouth rinse – Genotyping (HTG)- Taqman method CHANCE Study TARGET GENES – CYP1A1 CYP1B1 CYP2C9 CYP2E1 – NAT1 GSTM1 GSTT1 GSTP1 – EPHX1 – ADH2 NQO1 ADH3 – AGT – XPD XRCC1 APE1 MPO ADH4 MnSOD HOGG1 CHANCE Study • Tumor Blocks • Tumor expression arrays • Medical Records • • • • Social Factors Access to Health Care Screening Follow-up of Cases (new survivor study)