Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
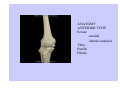
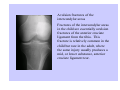
THE KNEE JOINT: 4 bones: femur, tibia, patella and fibula 3 separate joints: tibiofemoral, patellofemoral, and tibiofibular joint Function: allows certain movements, restricts others, and provides load transfer through the lower limb. JOINT MOTIONS: 3 translations 3 rotations ANATOMY ANTERIOR VIEW Femur -medial -lateral condyles Tibia Patella Fibula LATERAL ANATOMY: Lateral Supracondylar line L. intermuscular septum Lateral epicondyle Lateral condyle Tibial plateau Lateral tibial condyle Gerdy’s tubercle Tibial tuberosity Apex of fibular head “styloid process” Fibular head MEDIAL ANATOMY: Femur: Adductor Tubercle - distal end of adductor magnus tendon - uppermost part of MCL Medial epicondyle Tibia: Medial condyle Tibial plateau FEMUR: INTERCONDYLAR FOSSA Separates the medial and lateral femoral condyles posteriorly -within the capsule -not part of articular surface therefore, not covered by articular hyaline cartilage. Posterior intercondylar fossa (tibia) Popliteal surface Medial/Lateral supercondylar line -VM, AddM,/BF, plantaris TIBIOFIBULAR JOINT: The fibula is attached to the tibia proximally with ligaments, and along its length by the interosseous membrane. Tib/Fib joint + ligaments of talus, calcaneus and tibia allow very little motion between fibula and tibia. - Fixed joint - Head of the fibula moves with ankle motion MENISCUS: Lateral meniscus Medial meniscus Transverse meniscal ligament Posterior menisco-meniscal ligament Anterior/Posterior horn -attached to intercondylar tibial plateau -vascular like periphery MENISCOFEMORAL LIGAMENTS: Anterior meniscofemoral ligament (Ligament of Humphry) Posterior meniscofemoral ligament (Ligament of Wrisberg) Increase stability of the knee joint by moving the lateral meniscus slightly medially and anteriorly when the knee is in flexion. VASCULAR/NERVOUS: Femoral artery Popliteal artery Popliteal vein Tibial nerve Sural n. Common peroneal n. Peroneal communicating n. Saphenous n Genicular arteries SYNOVIAL FLUID: Decreases viscosity at high shear rates The high viscosity helps to maintain a fluid film by resisting squeezing out with the joint at rest. PATELLA: Medial contact of femur in extreme flexion (rose) Facet for medial femoral condyle Facet for lateral femoral condyle Attachment of patellar ligament Lateral release 4 x’s body weight with knee flexed 70-80 degrees of flexion ACL: Primary restraint to anterior translation of the tibia and contributes the most at 30° flexion. -Prevents hyperextension of the knee - Secondary restraint to internal tibial rotation - Resists adduction and abduction at full extension - 'guides' the screw home rotation of the knee joint as it approaches terminal extension ACL: -Footprint -Roof of intercondylar notch during extension -Difficulty in placement of ACL BUNDLES of ACL: 2 functional units: Anteromedial bundle taut in flexion Posterolateral bundle taut in extension -Increases knee stability -Likelihood of partial ruptures in these positions PCL: Primary restraint posterior translation of tibia Secondary restraint external tibial rotation at 90° flexion, which reduces upon knee extension Near full knee extension, the anterior bundle of the PCL slackens, and the posterolateral structures become the primary restraint. PCL footprint No fan out like the ACL The fibers are almost parallel to bone Medial collateral ligament functional units The medial collateral ligament is the primary restraint to abduction and internal tibial rotation. Secondary role of MCL: Provides anterior knee stability, which is enhanced by external tibial rotation. With anterior cruciate disruption the medial collateral ligament provides most of the anterior stability of the knee. Stabilising role of the lateral collateral ligament Primary restraint to adduction of the knee Secondary restraint to anterior and posterior drawer, when the drawer displacements are large. Combined with the other lateral structures the lateral collateral ligament is a significant restraint to external rotation of the tibia. Meniscal biomechanics and Functional anatomy Medial meniscus has a firm bond to MCL Lateral meniscus has no attachment to LCL Because the popliteus tendon attaches to the posterolateral corner of the lateral meniscus, there is some additional mobility and decreased vascularity in this location. The transverse ligament joins the anterior horns of the two menisci. Posterolateral rotatory instability Frequently, the lateral collateral ligament, fabellofibular ligament, and popliteofibular ligament are ruptured together. This results in an increase in external tibial rotation at all angles of knee flexion and adduction and posterior drawer from 0 to 60° flexion with external tibial rotation. Varus-valgus test A varus or valgus moment is applied at full extension and approximately 30° knee flexion. The MCL is the primary restraint against valgus moments at 30° flexion whereas it is a secondary restraint at full extension. The LCL is a primary restraint against varus moments over the range 5 to 25° flexion. This test assesses medial or lateral capsule or ligament damage. Anteromedial rotary instability test The tibia is rotated externally and an anterior drawer test is carried out at 90° flexion. This test illustrates posteromedial capsule, MCL, and ACL disruption. When the MCL is intact, tibial external rotation tightens it and anterior drawer is less than in neutral rotation. Tests for posterolateral instability Damage to the posterolateral structures causes external tibial rotation at all angles of knee flexion. PCL damage allows the tibia to also displace posteriorly during external rotation at 90° knee flexion, exaggerating the motion of the fibula relative to the lateral femoral condyle. Posterolateral drawer test - knee flexed between 60 and 90° flexion and the foot rotated externally, the lateral tibial plateau will displace posteriorly. The pivot shift test Reduction test - knee is flexed from full extension under a valgus moment. Subluxation test - reverse of reduction test. The knee is extended from a flexed position under a valgus moment. Both tests assess for anterolateral instability, which is caused by a full tear of the anterior cruciate ligament, sometimes combined with injuries to the lateral structures, such as a stretching of the lateral collateral ligament. Patellar tendon The patellar tendon is one of the longest collagenous structures of the body and is designed to transmit very high tensile loads. Maximum stress and modulus of the patellar tendon have been reported as double that of the cruciate ligaments from the same knee (Butler et al, 1986). During normal daily activity such as walking and stair climbing, the tensile force in the patellar tendon can reach three times bodyweight. Typically occur in older patients with associated joint space narrowing. They may present with loading type pain or mechanical symptoms such as catching. At arthroscopy, preservation of as much meniscal tissue as possible should be the principle. Patients with significant joint space narrowing should be warned beforehand that partial meniscectomy may not provide the degree of pain relief that the patient may expect, and that progression of the arthritic process can be expected. If indicated, an extensive synovectomy and removal of any impinging osteophytes should be part of the procedure p complications. The portal of bacterial entry may be a graze or laceration near the knee, infected eczema or athlete's foot more distally. Treatment of the inflamed bursa includes prevention of further mechanical irritation, rest and antiinflammatory medication. In the presence of cellulitis or any evidence of bacterial infection, antibiotics are indicated. Abscess formation will, of course, require incision and drainage. pp patellar ligament to the inferior pole of the patella and this patellar tendinitis may be associated with an enlarged infrapatellar bursa. Treatment of the inflamed bursa includes prevention of further mechanical irritation, rest and antiinflammatory medication. In the presence of cellulitis or any evidence of bacterial infection, antibiotics are indicated. Abscess formation will, of course, require incision and drainage. Baker’s cyst The cyst is the constantly swollen bursa in relationship to the semimembranosus tendon and although it arises in the medial part of the popliteal fossa, it usually presents as a central popliteal fossa mass. The majority of Baker's cysts appear spontaneously, and typically persist for 1 or 2 years before spontaneous resolution. Exploration and excision are advisable if the cyst enlarges rapidly, or if there is any doubt as to the nature of the lesion. Avulsion fractures of the lateral tibial condyle A lateral tibial condyle avulsion fracture occurs in severe rotary strains when the anterior cruciate ligament is ruptured at the same time. The avulsion fracture is called a Segond fracture and was thought to be pathognomonic of anterior cruciate ligament rupture when the telltale flake avulsion was noted on routine x-ray or MRI. However, it is now known that it may also be associated with posterior cruciate ligament rupture. Avulsion fractures of the intercondylar areas Fractures of the intercondylar areas in the child are essentially avulsion fractures of the anterior cruciate ligament from the tibia. This fracture is relatively common in the child but rare in the adult, where the same injury usually produces a mid, or lower substance, anterior cruciate ligament tear. Group 1 -fractures are minor, distal and undisplaced. Group 2 -fracture separation of the whole tuberosity with displacement of the fractured segment. Group 3 -proximal fractures with major displacement, and comminution involving also the upper tibial region. Conservative treatment is recommended for fractures with minimal or no displacement. All other displaced fractures are best managed by internal fixation usually with a tension band technique. Styloid process - direct blow or avulsion LCL if affected instability May rupture the peroneal nerve or result in hematoma present around the nerve may interfere with its function. Common fractures of the patella A stellate type of multifragmental fracture is usually the result of falling onto a flexed knee. Transverse fractures occur when, with the quadriceps muscle tightly contracted, a relatively minor blow to the anterior knee region causes a transverse break in the patella separating the superior and inferior fragments. The transverse patellar fracture is most stably fixed by a tension band wire technique. Stellate fracture- encircling wires and fragmentary wire fixation. Patella trauma A fracture involving the full thickness of the patella in a child is extremely rare. However fractures of the patellar articular facets are less uncommon. Patellar dislocations in children Lateral - This is by far the most common variety. Intercondylar - This is a rare type of dislocation wherein the patella is seen to be turned on its side and fixed in the intercondylar region. Medial - This is extremely rare, and when present, is usually iatrogenic. Lateral patellar dislocation in children may be either congenital or acquired. Osgood-Schlatter’s disease Etiology of this painful condition, with a very tender mass developing at the insertion of the patellar tendon, is due to a traction avulsion lesion of the tibial tubercle and represents an avulsion fracture healing to a degree and then further being avulsed.