Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
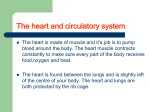
CARDIOVASCULAR AND RESPIRATORY PHYSIOLOGY – Biology 2 I. HEART SOUNDS - Auscultation (using a stethoscope) As the blood traverses the heart and the valves open and close, certain heart sounds are produced and can be identified through a stethoscope. The cardiac cycle sounds like “LUBB, DUP, PAUSE.” The first heart sound is the LUBB. This sound, marking the beginning of ventricular systole, occurs as the atrioventricular valves close. At this point the ventricles are contracting and the semilunar valves are closed for a period of isovolumetric contraction. As the pressure rises, the semilunar valves open and the blood is ejected. The DUP, the second heart sound, occurs at the beginning of ventricular diastole when the semilunar valves close. Just after the “dup” you may hear a faint sound. This is the sometimes inaudible third heart sound. The usually inaudible fourth heart sound might be heard just before the “lubb” sound. Both the third and fourth sounds are the result of systolic and diastolic blood flow rather than valve closings. Using a stethoscope, listen to your partner’s chest, preferably at about the fifth intercostal space (the region of the bicuspid valve) and at about the bottom of the sternum (the region of the tricuspid valve). See if you can hear the LUBB, DUP, PAUSE. The diagram shows the major auscultation sites. DESCRIBE the difference in heart sounds. II. PULSE PULSE, the pressure surges resulting from the rhythmic flow of blood through a vessel, results from the pumping of the heart. Blood moves through all blood vessels, and the pressure surge can be quantified and qualified in any vessel. However, for most purposes, we are interested in the pulse as measured in the major arteries. Using your three middle fingers and very light pressure, locate the following pulse points, preferably on your lab partner. MEASURE the pulse rate for a minute for at least three locations. TEMPORAL - side of the head, temporal region. CAROTID - neck, about 1 cm caudal and slightly medial to the angle of the jaw. RADIAL - lateral wrist POPLITEAL - back of knee. (Sometimes hard to find. This artery is deeper in some folks.) DORSALIS PEDIS - dorsum of foot, best felt slightly medial to proximal end of first metatarsal. You can also find a BRACHIAL pulse (where your arm bends) or a FACIAL pulse just anterior to the masseter muscle or the FEMORAL pulse in the groin area. Finding the pulse is usually not sufficient. You will want to know certain characteristics of the pulse. These include: RATE - How many beats per minute? The most accurate measurement seems to be to count for one full minute. For normally healthy people who have not been performing any vigorous exercises, it is usually adequate to count for 15 seconds and multiply by 4. In the cardiovascular efficiency test later in this exercise, you will be asked to count for 10 seconds and multiply by 6. The reason for this is that you will have been exercising and you want an immediate number. Over the course of a full minute, the pulse may slow down considerably, so a full minute count will not be as accurate as a 10 second count. A resting pulse usually averages about 70-80 beats per minute. Due to individual differences, average pulse rates between 40 and 110 are usually considered normal. An accelerated pulse rate is known as TACHYCARDIA, and an unusually slow rate is BRADYCARDIA. These conditions may or may not be pathological. If either condition is noted for an extended period of time, the cause should be determined by an appropriate health care professional. DESCRIBE your pulse or that of your partner for each of the following three characteristics: RHYTHM - Does the pulse maintain a regular rhythm or does it speed up or slow down or skip beats? For checking rhythm, the longer pulse count will be more accurate because you will have less chance of missing an irregularity. (Be assured that everyone has an occasional rhythmic irregularity!) TENSION - Does the pulse feel firm and strong, moderate, or weak and wimpy? Are there any changes in tension over the time span? AMPLITUDE - Can you see the pulse throbbing? If so, is it high (visible), moderate, or low (invisible)? All of the pulses can be visible on occasion. Often the easiest one to see is the radial pulse. Relax your arm and hyperextend your wrist slightly. Sometimes if you can see the radial pulse this way, you can also see the ulnar pulse. Various factors can affect rate, rhythm, tension and amplitude. Activity level, standing in one place, lying down, etc. all have different affects on pulse. III. BLOOD PRESSURE The force exerted by the blood against the blood vessel wall is the BLOOD PRESSURE. Technically, every vessel in the body has a blood pressure. The blood pressure we normally think of is the pressure exerted on the walls of the aorta by the blood as it exits the heart. This pressure is measured as close to the heart as possible (at the same level as the heart so that hydrostatic pressure is not a factor), normally on the brachial artery. This pressure is known as ARTERIAL BLOOD PRESSURE. The highest, or peak, blood pressure occurs as the blood is ejected into the arteries. This is the SYSTOLIC PRESSURE. Systolic pressure corresponds with ventricular systole, the contraction that ejects blood from the ventricle into the aorta. The lowest pressure recorded during the cardiac cycle is the DIASTOLIC PRESSURE, the amount of “non-push” pressure that is always present in the vessel. Diastolic pressure is a measure of the condition of the blood vessels. Diastolic pressure corresponds with the last part of ventricular diastole, the relaxation phase of the cardiac cycle. Blood pressure is measured in millimeters mercury (mm Hg). If a pressure number is 75, this means that the pressure exerted by the blood is sufficient to push up a column of mercury 75 mm (at STP). If your blood pressure is 120/80, the 120 is the systolic pressure, the force on the blood vessel as the blood is being ejected, and the 80 is the diastolic pressure, the amount of pressure exerted by the resting blood. The SPHYGMOMANOMETER is the instrument used for taking the blood pressure. Several different types of sphygmomanometers exist. You will be using a simple digital device – a wrist or arm cuff. No matter what type you are using, they work as follows. The cuff is inflated beyond the point that cuts off circulation in a given artery. The cuff pressure is measured on a gauge or a digital terminal. HYPERTENSION (significantly elevated blood pressure) is usually considered if the resting systolic pressure is above 140 and the resting diastolic pressure is above 90. You many have heard of “white coat hypertension,” the phenomenon whereby a person’s blood pressure only goes up in the doctor’s office. This very real phenomenon demonstrates the role of the psyche in physiological events. Sometimes people with severe “white coat hypertension” must have their blood pressures taken outside the medical setting. RECORD your blood pressure. PULSE PRESSURE is the mathematical difference between the systolic and diastolic readings. If you blood pressure is 120/80, your pulse pressure is 40. RECORD your pulse pressure and EXPLAIN what value might exist in knowing pulse pressure. Certain pathologies can be identified by checking blood pressures in different parts of the body. For instance, if all factors are equal, the blood pressure in the right arm should be approximately equal to the blood pressure in the left arm. Large discrepancies - as may occur after a stroke should always be investigated. If you are lying down, the ratio of your popliteal blood pressure to your brachial blood pressure should be approximately one. Gross discrepancies could indicate an arterial obstruction. EXERCISE AND BLOOD PRESSURE (Do this activity and record your results.) 1. Make sure that your partner has taken your resting blood pressure. Record 2. Keep the cuff wrapped snugly in place but not tight enough to cut off circulation. 3. Run in place for 2 minutes. 4. As soon as the run is complete, have your partner take your blood pressure. Record the new pressure. 5. Wait 3 minutes and have your partner take your blood pressure again. Record. Was your blood pressure back to normal after 3 minutes. If not, what factors do you think could account for the difference. VENOUS BLOOD PRESSURE Venous blood pressure cannot be measured directly with a standard sphygmomanometer. There is, however, a rather accurate indirect method of measuring venous blood pressure. This test works best in a warm room (to avoid vasoconstriction). 1. Hold your hand down and observe the veins on the dorsal surface. 2. Practice raising your hand slowly to a position above your head. Notice how the veins collapse. 3. Perform the actual test by extending your hand straight out on a level with your heart. Your partner can note the position. Slowly raise your hand until the veins disappear. 4. Your partner should now measure in centimeters the distance your hand traveled above your heart. This is the point where the venous pressure is overcome by gravity. 5. To convert this figure to blood pressure in mm Hg, use the fact that each 13.6 mm your hand rises above your heart will be represented by a 1 mm rise in the mercury. Therefore: mm Hg = _____cm x 10/13.6. RECORD your venous pressure. Your venous pressure should be between 0 and 10 mm Hg. How does your venous pressure correlate with the information in the figure below? IV. CARDIOVASCULAR FUNCTION One function of the heart is the transport of oxygen to energy-producing cells. When energy requirements increase, the heart may have to beat faster to circulate the blood so that those cells are supplied with the oxygen necessary for energy production. Pulse rate should increase to supply the oxygen demanded by the cell. When the demand goes down, the pulse rate should decrease accordingly. In the healthy person, the pulse should return to a baseline value within minutes after exertion. A CARDIOVASCULAR EFFICIENCY test is a test that indicates how well the heart is doing its job. For this particular test you will need a watch with a second hand. 1. Begin by sitting in a relaxed position while your partner takes a 10 second carotid pulse. 2. Multiply this number by 6 and record in the chart as the baseline. 3. Run in place for 10 ten-second innings with ten-second rest periods between the innings. 4. Your partner will record the data and keep time. 5. As you run in place, count the number of times your right foot strikes the floor. Run as fast as you can. As you finish each inning, tell your partner how many right-foot hits you had. Your partner will record this. 6. Ten seconds after finishing the 10th inning, your partner should take your carotid pulse again. Your partner should again take the carotid pulse at 2 minutes, 4 minutes, and 6 minutes after the exercise is complete. Record the data. V. RESPIRATORY FUNCTION A spirometer is an instrument that measures different volumes of air involved in respiration. Basically, air, exhaled from the lungs, causes displacement of a closed chamber that is submerged in water. Air blown into the inverted chamber (through a hose) will cause the chamber to rise; this moves the indicator arrow along a scale, calibrated in liters. Because the water in the spirometer is cooler than body temperature, the air will contract and take up less volume…………so you need to use the chart below that contains correction factors. Be sure to multiply your values by the correction factor for the temperature of your spirometer water. We are only going to do the Vital Capacity Measurement. FIRST: Determination of Resting Respiratory Rates 1. Count the number of exhalations in 60 seconds. 2. Make 3 counts while standing quietly. 3. Record and calculate the average. Trial 1: Measuring VITAL CAPACITY (VC) Vital capacity is the amount of air that can be forcibly exhaled following a maximal inhalation. 1. Stand and slowly and deeply breathe in and out for a while. 2. Breathe in as deeply as possible, insert the mouthpiece. 3. Breathe out as forcibly as possible. 4. Read and record. In addition to the experiments described above, four other measurements of lung capacity can be calculated: Residual Volume (RV): The lungs are never completely emptied, always containing about 1200 ml of air in adults. Functional Residual Capacity (FRC): This is the amount of air remaining in the lungs after normal exhalation, FRC = ERV + RV. Inspiratory Capacity (IC): The amount of air which can be inhaled after normal expiration, IC = TV + IRV. Total Lung Capacity (TLC): This is the amount of air contained in the lungs after a maximal inhalation, TLC = TV + IRV + ERV + RV. Table 1. Correction Factors for Converting Spirometer Volumes to Body Temperature. Spirometer Temperature (OC) Correction Factor Spirometer Temperature (OC) Correction Factor 15 1.130 23 1.085 16 1.124 24 1.08 17 1.118 25 1.075 18 1.113 26 1.068 19 1.107 27 1.063 20 1.102 28 1.057 21 1.096 29 1.045 22 1.091 30 1.039 Predicted Measured Vital Capacity VC (ml): TV + IRV + ERV = Notes: Do not assume that these volumes should match exactly. Inconsistency is expected to be relatively large because the apparatus used is crude, and the results depend on voluntary efforts on the part of the subject. Vital capacity varies with sex, body size and age. Its value, based on data collected from large numbers of non-smoking individuals living in a low pollution area, may be predicted as follows: Men: Women: Predicted VC = 0.121 H - 0.0136 A - 3.18 Predicted VC = 0.078 H - 0.0154 A - 1.05 H = height in inches A = age in years Predicted VC in Liters Calculate the predicted vital capacity for your gender, height and age, and compare with the measured value (corrected). Measured values within + 20% of predicted are considered normal. RESIDUAL VOLUME (RV) and TOTAL LUNG CAPACITY (TLC) Residual Volume and Total Lung Capacity cannot be determined with the spirometer because they consist of (or include) the volume of air that cannot be exhaled under any circumstances. However, these values can be roughly predicted for normal individuals using the factors listed in Table 2. Table 2. Factors for Estimating Residual Volume (RV) and Total Lung Capacity (TLC) from Vital Capacity (VC). For VC, use the value that you measured with the spirometer. Age Residual Volume (RV) Total Lung Capacity (TLC) 16-34 RV = VC x 0.250 TLC = VC x 1.250 35-49 RV = VC x 0.305 TLC = VC x 1.305 50-69 RV = VC x 0.445 TLC = VC x 1.445 Calculate your predicted Residual Volume and Total Lung Capacity from your measured Vital Capacity. CARDIOVASCULAR LAB – DATA and Questions NAME_______________________________ I. DESCRIBE the difference in heart sounds at the different sites in the space to the left of the diagram. (aortic, pulmonic, tricuspid, mitral) II. MEASURE the pulse rate for a minute for at least three locations. Location __________________ Rate___________________ Location __________________ Rate___________________ Location __________________ Rate___________________ DESCRIBE your pulse or that of your partner for each of the following three characteristics: Rhythm: Tension: Amplitude: III. RECORD your blood pressure. Systolic _____________ Diastolic_____________________ Record your pulse pressure ______________________ What value might exist in knowing pulse pressure? EXERCISE AND BLOOD PRESSURE: Resting BP__________ BP after a run _____________ Was your blood pressure back to normal after 3 minutes? account for the difference.? BP after 3 min___________ If not, what factors do you think could RECORD your venous pressure ____________________ Your venous pressure should be between 0 and 10 mm Hg. How does your venous pressure correlate with the information in the figure that is shown in the lab instructions? IV. CARDIOVASCULAR FUNCTION Base Pulse___________ Steps Inning 1_________ Steps Inning 6_________ After Pulse___________ Steps Inning 2_________ Steps Inning 7_________ 2-min Pulse___________ Steps Inning 3_________ Steps Inning 8_________ 4-min Pulse___________ Steps Inning 4_________ Steps Inning 9_________ 6 min Pulse___________ Steps Inning 5_________ Steps Inning 10________ Create a graph (paper on next page) where you plot your number of steps (y axis) against the innings (x axis). What fluctuations do you observe? How can you explain these? Now create a second graph where you plot pulse rate (y axis) again time (x axis). This is a GENERAL FATIGUE CURVE. Does your curve surprise you? Why or why not? At about minute 4, you may notice a dip below the baseline level. What do you suppose accounts for this dip? What does it mean if your pulse rate is not back to normal after 6 minutes? How does your cardiovascular efficiency stack up against the cardiovascular efficiencies of your classmates? Did anything surprise you about this test? How many times per year does your heart beat (on the average)? ________________________ V. RESPIRATORY FUNCTION Record your resting respiratory rate: 1st 2nd 3rd Average Resting Respiratory Rate (breaths/min) Record the following for yourself: Vital Capacity (VC) _________________ Determine the temperature of the spirometer = determine your corrected Vital Capacity. C. Using the chart in the lab instructions, Corrected Vital Capacity (VC) ____________________ Predict the following using the corrected Vital Capacity: Residual Volume (RV) _________________ Total Lung Capacity (TLC) _____________________ Men: Women: Predicted VC = 0.121 H - 0.0136 A - 3.18 Predicted VC = 0.078 H - 0.0154 A - 1.05 H = height in inches A = age in years Predicted VC in Liters Calculate the predicted vital capacity for your gender, height and age, and compare with the measured value (corrected). Measured values within + 20% of predicted values are considered to be normal. Predicted Vital Capacity (ml) = ___________________________ Measured Vital Capacity (ml) = ___________________________ % difference in two numbers = ___________________________ Calculate your predicted Residual Volume and Total Lung Capacity from your measured Vital Capacity. Predicted Residual volume (ml) = Predicted Total Lung Capacity (ml) = On the next page, record the vital capacity for each of the people in your class. You will be recording from a transparency where people have placed their data. You will then graph your results according to the instructions. Data: Vital Capacity Measurements for Period ___ Student # Average Vital Capacity (mL) Height (cm) Weight (kg) Athletic fitness L, M, H Gender (m or f) Smoking environment (y or n) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 Analysis 1. Produce the following graphs with vital capacity on the “y” axis: a. Vital lung capacity vs. height (two lines, one female and one male) b. Vital lung capacity vs. weight c. Vital lung capacity vs. assessment of athletic fitness (bar graph) d. Two lines: Vital lung capacity vs. height (smoking environment) Vital lung capacity vs. height (non-smoking environment) SUMMARY CONCLUSION: Write a paragraph generalizing and describing what you have learned about vital lung capacity and the variables that were examined. Cardiovascular Function Graphs: Half of graph: # of steps vs. innings - Other half of graph: pulse rate vs. time Vital Lung Capacity vs. Height (men and women separate) Vital Lung Capacity vs. Weight Vital Lung Capacity vs. Assessment of Fitness (bar graph) Vital Lung Capacity vs. Height (two lines – smoking and non-smoking environments)