Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
SURGERY FOR CEREBRAL PALSY
PART 3: CLASSIFICATION AND OPERATIVE PROCEDURES
FOR THUMB DEFORMITY
M. A. TONKIN, N. C. HATRICK, J. R. T. ECKERSLEY and G. COUZENS
From the Department of Hand Surgery and Peripheral Nerve Surgery, Royal North Shore Hospital, the University of Sydney
and the Spastic Centre of New South Wales, Australia
Spastic thumb deformity is the result of imbalance between intrinsic and extrinsic forces acting
across unstable joints. This paper presents a classification of spastic thumb deformity based on the
accurate assessment of the deforming forces, outlines methods for their correction and reviews the
results of our surgery. Thumb reconstruction procedures were performed in 32 patients with 33
spastic thumb deformities. All patients were assessed pre- and postoperatively using the same
functional assessment system which was performed by the same team. The thumb was maintained
out of the palm in 29 patients and lateral pinch was established in 26 patients.
Journal of Hand Surgery (British and European Volume, 2001) 26B: 5: 465–470
In Type 3, combined deformity, there is spasticity of
both the intrinsic and extrinsic thumb muscles. The
flexor pollicis longus, adductor pollicis, first dorsal
interosseous and flexor pollicis brevis are all involved to
some extent and the abductor pollicis longus, extensor
pollicis brevis and extensor pollicis longus are relatively
paretic. The metacarpal is adducted and the metacarpophalangeal and interphalangeal joints are flexed giving a
true ‘thumb-in-palm’ posture (Fig 3).
The principle of surgery is to decrease the deforming
forces and, where necessary, to augment the weakened
muscles and to stabilize joints. The aim of this paper is
to describe the assessment of the patients and to review
the surgery performed in our department, applying the
above principles.
INTRODUCTION
Upper limb deformity in cerebral palsy is a consequence
of imbalance between spastic and paretic muscles, often
acting on unstable joints. The position of the thumb is
dependent on the imbalance of extrinsic and intrinsic
forces acting across the carpometacarpal, metacarpophalangeal and interphalangeal joints, any of which may
be unstable.
Thumb deformity significantly impedes hand function. In extension it limits the span and therefore the size
of objects that may be grasped. In flexion it acts as a
block by occupying space in the palm and the lack of
active thumb movement for pinch and grasp limits the
usefulness of the hand. Surgery may be indicated to
improve function or to facilitate hygiene.
We use a classification system modified from that
proposed by House et al. (1981) to describe the thumb
deformity (Table 1). The classification type is assessed
having asked the patient to make a fist attempting to
maintain the thumb in the lateral pinch position. In
Type 1, intrinsic deformity, there is spasticity of the
intrinsic thumb muscles causing adduction of the thumb
metacarpal, flexion of the metacarpophalangeal joint
and extension of the interphalangeal joint (Fig 1). The
deforming forces are the adductor pollicis, the first
dorsal interosseous and the flexor pollicis brevis
muscles. The relative tightness of the adductor and
short flexor will determine the position of the thumb
with one or the other occasionally dominant. The
abductor pollicis longus, extensor pollicis brevis and
extensor pollicis longus are paretic.
In Type 2, extrinsic deformity, there is spasticity of
the extrinsic thumb flexor (flexor pollicis longus) causing
flexion of the metacarpophalangeal and interphalangeal
joints. Metacarpal adduction is less marked (Fig 2). The
extensor pollicis longus is paretic and wrist extension
accentuates interphalangeal joint flexion. Isolated
extrinsic spasticity is uncommon.
PATIENTS AND METHODS
Thirty-two patients who had surgery for spastic thumb
deformity between 1986 and 1993 were retrospectively
reviewed. All patients were evaluated on several occasions preoperatively in the upper limb clinic run in
conjunction with the Spastic Centre of New South
Wales. A standard functional assessment was performed, including video-taping of set tasks. Five criteria
were chosen to assess functional ability: eating (ability
to hold knife and fork and cut up food), dressing
(pulling up trousers and doing up buttons), tying shoelaces, riding a bicycle (indicates ability to grasp and
release) and playing sports. Patients were graded as
independent, requiring assistance or totally dependent in
their performance of each task.
Hand sensibility was assessed by testing joint position
sense, two-point discrimination, touch and temperature
sense and stereognosis. Shoulder and elbow positioning
and patterns of hand use including grasp and release
were documented. To assess the cause of the thumb
deformity, the positions of the carpometacarpal, meta465
466
THE JOURNAL OF HAND SURGERY VOL. 26B No. 5 OCTOBER 2001
Table 1—Classification of thumb deformity
Type of deformity
Deforming forces
Thumb position
Type 1, intrinsic
Adductor pollicis
First dorsal interosseous
Flexor pollicis brevis
Metacarpal adduction
MCP joint flexion
IP joint extension
Type 2, extrinsic
Flexor pollicis longus
MCP joint flexion
IP joint flexion
Metacarpal adduction less marked
Type 3, combined
Adductor pollicis
First dorsal interosseous
Flexor pollicis brevis
Flexor pollicis longus
Metacarpal adduction
MCP joint flexion
IP joint flexion
(True ‘thumb-in-palm’ deformity)
Abbreviations: MCP, metacarpophalangeal; IP, interphalangeal.
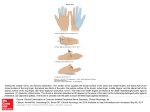
Fig 1 Type 1: intrinsic deformity.
carpophalangeal and interphalangeal joints were recorded during active fist formation, which determines
the classification type, and active radial abduction of the
thumb with simultaneous wrist and finger extension.
The passive range of motion of each joint was also
documented. This detailed examination allowed the
surgeon to determine the balance between spastic and
Fig 2 Type 2: extrinsic deformity.
paretic muscles and to identify underlying joint instability. A decision could then be made as to whether
release procedures alone were indicated or whether
transfers to supplement weak motors or joint stabilization procedures were also required (Goldner, 1988;
House, 1994; Manske, 1990; Zancolli and Zancolli,
1987).
THUMB DEFORMITY IN CEREBRAL PALSY
467
Fig 3 Type 3: combined deformity.
Surgical techniques
The following muscle releases, transfers and joint
stabilization procedures were utilized to balance the
deforming forces:
1. Releases. Adductor release was usually performed
through a curved palmar incision along the thenar
eminence crease (Matev, 1970) (Fig 4). The oblique and
lateral heads were released from their origins. When
indicated, the flexor pollicis brevis was also released and
the first dorsal interosseous was detached from its first
metacarpal origin through a dorsal incision. When a
dorsal approach was used the adductor was released by
selective incision of the tendinous fibres within the
muscle distally. To release an extrinsic contracture of the
flexor pollicis longus, an intramuscular tendon slide was
performed through a longitudinal incision in the distal
forearm. The tendon was released until it slid 1cm
distally within the muscle so as not to over-weaken the
thumb flexor (Fig 5).
2. Tendon transfers. Extensor pollicis longus re-route–
extensor pollicis brevis: the extensor pollicis longus was
divided proximal to the interphalangeal joint and
re-routed through the first dorsal compartment
and reattached to the extensor pollicis brevis at the
metacarpophalangeal joint (Manske, 1985). The
intrinsic connection to the interphalangeal joint was
maintained. Brachioradialis transfer: brachioradialis
was mobilized by extensive proximal dissection and
transferred as an active motor to abductor pollicis
longus or the thumb extensors. Abductor pollicis longus
tenodesis: a slip of abductor pollicis longus was
tenodesed either around brachioradialis or the first
dorsal compartment.
3. Joint stabilization. Metacarpophalangeal joint
sesamoid capsulodesis: the radial sesamoid was
attached to the metacarpal at the head–neck junction
via a suture through the metacarpal, tied dorsally
Fig 4 Incision for release of adductor pollicis.
Fig 5 Intramuscular slide of flexor pollicis longus
(Tonkin et al., 1995). Metacarpophalangeal or interphalangeal joint fusion was performed by resection
of the epiphyseal cartilage, preserving the growth
plate: stabilization was with an oblique K-wire
(Goldner et al., 1990).
468
Postoperatively, a short arm plaster cast maintained
the thumb in full radial abduction and 208 palmar
abduction for 5 weeks. Removable splinting was then
continued during an exercise programme in which the
patient was taught to abduct and extend the thumb
actively and to maintain the thumb out of the palm
during fist formation. Patients were also tutored in
activities requiring lateral, pulp and chuck pinch.
At follow-up, the standard functional assessment was
repeated by the same clinical team. The position of the
thumb joints during active and passive movements was
recorded and the ability to perform lateral pinch was
assessed.
RESULTS
There were 15 male and 17 female patients, of whom
three men and eight women were aged over 16 years.
The average age of the male patients under 16 years was
nine years. The average age of the females under 16
years was 11 years. Eleven patients were quadriplegic
(nine purely spastic, two with athetoid motion) and 21
were hemiplegic (17 with a primary diagnosis of cerebral
palsy, one with a head injury, one hydrocephalus and
two cerebrovascular accidents). The patients were
reviewed at an average 32 (range 10–88) months after
surgery.
In our series, 16 of the patients had a Type 3,
combined deformity. Eleven patients had Type 1,
intrinsic deformity and the remaining five had the
relatively uncommon Type 2, extrinsic deformity.
The thumb was maintained out of the palm in 29 of
the 32 patients (30 of the 33 thumbs). In 28 patients, this
was achieved with one operation. Three patients underwent one further operation and one had a total of four
operations. The majority of patients required three or
four surgical techniques to correct the thumb deformity
and these are outlined in Table 2. The number of release
and augmentation procedures are listed in Tables 3 and
4 respectively.
Lateral pinch was established in 26 thumbs: to the
middle phalanx of the index finger in 18 and to the
middle phalanx of the middle finger in eight. In the latter
group, the thumb was prevented from pinching against
the index finger by IP joint flexion in three cases and by
poor volitional control of index finger flexion which
trapped the thumb in the remaining cases. In four
thumbs, intermittent lateral pinch was possible but this
was not of functional use. In three thumbs, lateral pinch
was not established.
The number of patients who improved by one
functional grade is recorded in Table 5. No patient
improved from dependent to independent functioning.
None of the patients was made worse by surgery.
The preoperative and postoperative active positions
of the carpometacarpal, metacarpophalangeal and
interphalangeal joints are listed in Table 6: measure-
THE JOURNAL OF HAND SURGERY VOL. 26B No. 5 OCTOBER 2001
ments were available for 29 of the thumbs. Although the
average improvement in metacarpal abduction was only
198, this was functionally significant when it allowed the
thumb ray to be brought out of the plane of the palm.
In the 18 patients who underwent a sesamoid
capsulodesis, the position of the metacarpophalangeal
joint was improved from an average of 308 hyperextension preoperatively to 158 flexion postoperatively. There
were two patients in whom the sesamoid capsulodesis
failed and the procedure was repeated. One of these
patients subsequently required metacarpophalangeal
joint arthrodesis.
Five patients with severe wrist, finger and thumb
deformities had surgery primarily to improve cosmesis
and hygiene. They had flexor releases and transfers to
correct wrist and finger position and at the same time a
flexor pollicis longus release. Appearance was improved
in all five and lateral pinch established in two cases.
DISCUSSION
The decision to proceed to surgery should follow
detailed and repeated examinations, both within the
clinic and within the patient’s usual environment
(House, 1994; Swanson, 1982; Zancolli et al., 1983).
The assessment involves not only the surgeon and child,
but also the parents or guardians, the co-ordinating
physician, occupational and physical therapists and a
social counsellor. It is useful to video-tape the patients
performing different tasks. The selection of patients and
the functional outcome depend on a number of factors
including: the type and severity of the neuromuscular
disorder; the nature and extent of the deformity; the
quality of volitional muscle control; hand sensibility;
and the age and intelligence of the patient (Zancolli and
Zancolli, 1987).
Our classification of thumb deformity has evolved as
our experience with the condition has grown. We have
found that predictable results are dependent on an
accurate assessment of the deforming forces and underlying joint instability. Specific surgical techniques are
then directed to particular types of deformity as outlined
in the following paragraphs.
Releases
In order to produce a functional balance of thumb
motors, we prefer to weaken rather than defunction
spastic muscles by tenotomy. This maintains some
activity in the released muscle and reduces the possibility
of inadvertently over-correcting the deformity.
Adductor release (types 1 and 3)
In younger patients, a more controlled release of the
adductor is achieved through the palmar approach. This
allows correction of the thumb deformity without loss of
THUMB DEFORMITY IN CEREBRAL PALSY
469
active adduction. The dorsal approach is useful in older
patients with a myostatic contracture and for easy access
to the first dorsal interosseous. When a dorsal approach
is used, the selective incision of tendinous fibres distally
within the adductor muscle weakens but does not
defunction the muscle.
Flexor pollicis longus release (types 2 and 3)
The release should be intramuscular, allowing the
tendon to slide 1 cm distally, as it is important not to
over-weaken the muscle.
Extensor/abductor augmentation
The decision as to which extensor/abductor requires
augmentation is based on the preoperative evaluation
and also an intraoperative assessment of the tendon-unit
(recipient) which best draws the thumb out of the palm
(Fig 6). The choice of transfer depends on the
assessment of individual muscle control as well as
the usual principles of tendon transfers. Many transfers
are available (palmaris longus, flexor digitorum superficialis and even wrist extensors and flexors are possible
alternatives to brachioradialis and extensor pollicis
longus), but most are compromised by spasticity or
paresis. Therefore, the position obtained immediately
postoperatively is not always maintained. Accordingly,
function postoperatively relates to the quality of control
present preoperatively.
Our preferred techniques for extensor and abductor
augmentation are extensor pollicis longus to extensor
pollicis brevis transfer (especially in type 1) and
brachioradialis to abductor pollicis longus or extensor
pollicis brevis. The former procedure supplements
metacarpophalangeal joint extension but decreases
extensor activity to the interphalangeal joint. The latter
procedure provides an active motor to abductor pollicis
longus or extensor pollicis brevis and results in more
predictable function than an abductor pollicis longus
tenodesis. However, brachioradialis requires extensive
proximal dissection and is sometimes weak and under
poor volitional control. We now commonly employ the
extensor pollicis longus to extensor pollicis brevis
transfer in combination with brachioradialis to abductor
pollicis longus for type 1 and 3 deformities.
Joint stabilization procedures
These are required when underlying joint instability
compromises efforts to rebalance the forces or when,
owing to lack of volitional control; it is the only means
of controlling joint position. This is particularly
important for the metacarpophalangeal joint, where
hyperextension instability is exacerbated by augmentation of motors acting distal to the joint (extensor pollicis
longus, extensor pollicis brevis). This in turn leads to an
Fig 6 Intraoperative traction to assess which recipient tendon places
the thumb in the optimal position.
Table 2—Techniques used at operation
Release
Release and tenodesis
Release and transfer
Release, transfer and stabilization
Release, tenodesis and stabilization
Release, tenodesis and transfer
Release, tenodesis, transfer and stabilization
8
1
1
1
1
5
16
Table 3—Release techniques
Technique
Palmar adductor release
Palmar adductor plus first dorsal interosseous
Dorsal adductor release
Dorsal adductor plus first dorsal interosseous
Flexor pollicis longus slide
Number
12
1
9
3
20
Table 4—Augmentation of thumb extension/abduction
Technique
EPL re-route–EPB
Brachioradialis–EPB
Brachioradialis–EPL
Brachioradialis–APL
FDS–EPL
PL–EPL
APL tenodesis
Number
13
7
4
2
1
1
24
Abbreviations: EPL, extensor pollicis longus; EPB, extensor pollicis
brevis; APL, abductor pollicis longus; FDS, flexor digitorum superficialis; PL, palmaris longus.
adduction moment acting on the thumb metacarpal
rather than the desired abduction moment.
Metacarpophalangeal joint capsulodesis is an effective
way of overcoming hyperextension of this joint (Tonkin
et al., 1995). Metacarpophalangeal joint fusion (Goldner
et al., 1990), preserving the physis in immature bone, is
470
THE JOURNAL OF HAND SURGERY VOL. 26B No. 5 OCTOBER 2001
Table 5—Functional improvement
Task
Eating
Shoe-laces
Dressing
Bike
Sport
15
5
12
5
10
No. improved
Table 6—Active position of thumb joints (mean)
Preop
Postop
During
During
During
During
fist formation
radial abduction
fist formation
radial abduction
CMC joint{
MCP joint
IP joint
98
98
38
7108*
338
788*
248
58
178
7118*
258
58
{
The position of the CMC joint refers to the angle between the thumb metacarpal and the radial border of the forearm. When they are parallel, the
joint is in a neutral position.
*A negative figure implies extension beyond the neutral position of the joint (i.e. radial abduction at the CMC joint and hyperextension at the MCP
and IP joints).
Abbreviations: CMC, Carpometacarpal; MCP, Metacarpophalangeal; IP, interphaangeal.
used when capsulodesis cannot control hyperextension
or when tendon transfers fail to overcome a metacarpophalangeal joint flexion deformity. Carpometacarpal
joint fusion is rarely indicated except when it is
impossible to control metacarpal adduction: there is
then some preservation of movement from the scaphotrapezial joint. This is preferable to complete loss of
thumb metacarpal motion which results from an
interposition bone graft between the first and second
metacarpals. Interphalangeal joint fusion may be
considered for persistent flexion deformities or if the
joint is unstable.
Quantifying the functional outcome in this group of
patients is difficult. We have used a simple evaluation
system based on five daily tasks. We accept that the
estimation of thumb position is also imprecise, relying as
it does on the co-operation of the patient and the eye of
the examiner (albeit the same one in every case).
Furthermore, the final functional outcome is dependent
on the success or failure of other surgical procedures on
the limb (Gschwind and Tonkin, 1992; Tonkin and
Gschwind, 1992). We tend not to combine thumb
surgery with wrist and finger procedures, other than to
consider an flexor pollicis longus lengthening or
adductor release, if indicated, at the time of forearm
surgery. The correction of a wrist flexion deformity may
alter the attitude of the thumb significantly and we
therefore prefer to wait for 6–12 months after the former
procedure before considering a more sophisticated
correction of the thumb deformity.
The aim of surgery is to obtain firm lateral pinch to
the middle phalanx of the index finger during fist
formation, and radial abduction during finger and
thumb extension prior to grasp. The key to achieving
consistent release of the spastic thumb-in-palm deformity and to establishing functional lateral pinch is the
accurate determination of the deforming forces and the
identification of joint instability. This paper presents the
results of our early surgery applying these principles. It
is not designed to do anything other than describe our
results, our failures and to develop a philosophy which,
we hope, provides a logical approach to the choice of
release, augmentation and stabilization procedures.
References
Goldner JL (1988). Surgical reconstruction of the upper extremity in cerebral
palsy. Hand Clinics, 4: 223–265.
Goldner JL, Koman LA, Gelberman R, Levin S, Goldner RD (1990).
Arthrodesis of the metacarpophalangeal joint of the thumb in children
and adults: adjunctive treatment of thumb-in-palm deformity in cerebral
palsy. Clinical Orthopaedics and Related Research, 253: 75–89.
Gschwind C, Tonkin M (1992). Surgery for cerebral palsy. 1. Classification and
operative procedures for pronation deformity. Journal of Hand Surgery,
17B: 391–395.
House JH, Gwathmey FW, Fidler MO (1981). A dynamic approach to the
thumb-in-palm deformity in cerebral palsy. Journal of Bone and Joint
Surgery, 63A: 216–225.
House J (1994). Disorders of the thumb in cerebral palsy, stroke and tetraplegia.
In: Strickland JW (Ed.) The thumb. Edinburgh, Churchill Livingstone,
1994: 179–187.
Manske PR (1985). Redirection of extensor pollicis longus in the treatment of
spastic thumb-in-palm deformity. Journal of Hand Surgery, 10A:
553–560.
Manske PR (1990). Cerebral palsy of the upper extremity. Hand Clinics, 6:
697–709.
Matev IB (1970). Surgical treatment of flexion–adduction contracture of the
thumb in cerebral palsy. Acta Orthopaedica Scandinavica, 41: 439–445.
Tonkin M, Gschwind C (1992). Surgery for cerebral palsy. 2. Flexion deformity
of the wrist and fingers. Journal of Hand Surgery, 17B: 396–400.
Tonkin MA, Beard AJ, Kemp SJ, Eakins DF (1995). Sesamoid arthrodesis for
hyperextension of the thumb metacarpophalangeal joint. Journal of
Hand Surgery, 20A: 334–338.
Swanson AB (1982). Surgery of the hand in cerebral palsy. In: Flynn JE (Ed.)
Hand surgery. Baltimore, Williams and Wilkins, 1982: 476–488.
Zancolli EA, Goldner LJ, Swanson AB (1983). Surgery for the spastic hand in
cerebral palsy: report of the committee on spastic hand evaluation.
Journal of Hand Surgery, 8: 766–772.
Zancolli EA, Zancolli E Jr. Surgical rehabilitation of the spastic upper limb in
cerebral palsy. In: Lamb DW (Ed.) The paralysed hand. Edinburgh,
Churchill Livingstone, 1987: 153–168.
Received: 1 September 2000
Accepted after revision: 14 March 2001
Mr Michael A. Tonkin, Department of Hand & Peripheral Nerve Surgery,
Royal North Shore Hospital, St Leonards, NSW 2065, Australia.
E-mail: [email protected]
# 2001 The British Society for Surgery of the Hand
doi: 10.1054/jhsb.2001.0601, available online at http://www.idealibrary.com on