Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
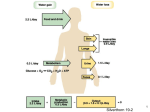
Renal: 11:00 - 12:00 Scribe: Teresa Kilborn Monday April 6, 2009 Proof: Hunter Neill Dr. Schafer Renal Physiology Page 1 of 4 DCT- distal convoluted tubule, PCT- proximal convoluted tubule, CD- collecting duct I. Renal Physiology – Lecture 5 [S2] a. Body water balance b. Sites and amounts of water reabsorption that occur along the nephron c. How water reabsoption in the distal nephron is regulated (by ADH) d. ADH (aka anti-diuretic hormone or aldosterone or vasopressin) works against diuresis or conserves water, is released by the posterior pituitary, and is regulated plasma osmolality and extracellular fluid volume e. Feedback mechanism of water reabsorption. II. Body water balance [S3] a. Water balance- in steady state, unless you are swelling up or really dehydrated, water intake has to be equal to water output b. Water intake is highly variable. The numbers he gives would be typical c. About half of our fluid intake is in the form of the fluids we drink. d. The rest comes from the food we eat and metabolism (end products of metabolism are CO2 and water) e. All of the input has to be balanced by the output f. A small amount of water is put out in the feces (changes to a lot with diarrhea), you have insensible water loss as it evaporates from your skin, and you lose water from your lungs as you breath out air with a higher humidity than you breath in g. Water output can greatly vary. If you are working outside or working out you’re probably sweating. Sweat is a hypotonic fluid and has half the osmolality of the plasma. It can be a source of a lot of water loss h. What makes the output equal to the intake? Regulating the urine output or flow rate. Most of urine is water. i. What we want to regulate is the excretion of water via the urine by regulating how much is reabsorbed in the final part of the nephron III. Introduction of a maximally dilute urine in the absence of ADH [S4] a. How do you generate maximally dilute urine? b. If you drink 1 L of water over ten minutes or more you are going to increase urine flow rate over the next hour or more. c. This is a rapidly responding system that you can quickly dilute your urine and put out an increased urine flow rate at a low plasma osmolality. d. How does this happen? When there is no production of ADH. The late DCT and CD stay water impermeable. You continue to reabsorb Na+ and Cl- by the NaCl co-transporter and the Na+ channels in the CD. As the salt is reabsorbed, the water can’t go with it and the urine is going to get more dilute than it was at the macula densa. It can get down to 75 or 50. e. Because you haven’t resorbed any water along the terminal part of the nephron your urine flow rate can be high. Maximal urine flow rates can be 10-12 mL/ min or 18 L/ day in a person who can’t produce ADH for example because of a defect in the pituitary production of ADH or a brain lesion. In those circumstances, you can have a urine flow rate that is 10-12% of the GFR. f. Even if you don’t have ADH, there are still the other parts of the nephron such as the PCT or descending loop of henle is still reabsorbing water and you are going to resorb 85% or more of water even in the absence of ADH g. When you have a high urine flow rate going through the CD system, it tends to reduce the osmolality of the medullary interstitium. Instead of having an osmolality of about 1200 at the tip, it will get as low as 600. So even if you give these individuals ADH, they still can’t concentrate urine as much as a normal individual because the medullary hypertonicity is not as high. More later. h. The reason for the loss of tenacity in this region is due to the loss of urea which is concentrated down in the tip of the papilla. IV. Introduction of a maximally concentrated urine in the presence of ADH [S5] a. What happens in the presence of ADH when you want to produce a maximally concentrated urine b. This will be a state of anti-diuresis. A state of low flow of urine and high osmolality. How do you get the water reabsorption and what makes the urine concentrated? The concentration of the urine can get as high as that that is found in the medullary region or about 1200. About 4X the osmolality of the plasma is what can be achieved. c. The part of the nephron that is outlined in blue is always impermeable to water The tubular fluid that comes to this region is always dilute d. ADH increases the water permeable of the late DCT and CD. It makes it very water permeable. e. Water can leave osmotically and in the outer cortex the osmolality of the tubular fluid is going to rise to that of the plasma f. As you go into the medulla of the kidney where the interstitial fluid is hypertonic, water will leave more and it will equivocate the osmolalilty of the urine to the osmolality of the medullary interstitium. With a diuretic the Renal: 11:00 - 12:00 Scribe: Teresa Kilborn Monday April 6, 2009 Proof: Hunter Neill Dr. Schafer Renal Physiology Page 2 of 4 osmolality of the medullary interstitium is maximal (1200) all that happening is osmotic equivocation that is allowed because of the high water permeability g. Under these conditions you can get a urine volume as low as 400 mL and that is necessary to get rid of your metabolic such as urea and creatinine h. Urine flow rates can be .2-.3 mL/min under these conditions. i. Low urine flow rates with high osmolality. V. ADH action in principal cells [S6] a. What does the ADH hormone do? It binds to receptors located in cells of the late DCT and CD. b. Through a cascade of events you will have the intracellular production of cAMP which then causes the phosphorylation of proteins that causes the insertion of water channels into the luminal membrane of the distal tubule cell called Aquaporin 2 (AQP2). These are different channels than those found in the PCT. They are stored in vesicles under the luminal membrane. Once inserted into the membrane, it is water permeable. c. The basolateral membrane is always water permeable because of the presence of AQP3 and AQP4 that are always presence (you don’t have to know the names of these just that they are different from AQP2, just know the difference in AQP1 and AQP2- AQP1 is always present in the PCT) d. When you take away ADH, then the AQP2 are taken out of the luminal membrane. e. The process putting the AQP2 into or out of the membrane takes about 10-15 minutes f. You can change the osmolality or urine flow rate by changes in the ADH. You get anti-diuresis VI. ADH (vasopressin) release from posterior pituitary [S7] a. Another, older name for ADH is vasopressin b. Historically, they thought it was a hormone that raised BP. This only happens at high concentrations though, at lower doses it acts as an anti-diuretic hormone. c. There are cells that are in the supraoptic (primarily) and paraventricular nucleus of the hypothalamus that respond by swelling or shrinking as the plasma osmolality rises or falls. d. When they fire an AP, it goes from the supraoptic nucleus down the axon to the nerve endings that store the ADH. ADH is produced in the cell bodies in the supraoptic nucleus and carried by axon streaming to the secretory vesicles in the nerve endings in the posterior pituitary. An AP causes the exocytosis of the vesicles containing ADH into the plasma. VII. Increased plasma osmolality increases ADH release and thirst [S8] a. The normal plasma osmolality is from 275-290 and varies from individual to individual. b. At low plasma osmolality, the cells are going to be plump in the supraoptic nucleus and the release of ADH will be suppressed c. When the plasma osmolality rises the cells will shrink causing APs and the release ADH from the synapses. This is a physiological feedback mechanism. d. Another reaction happens due to another hypothalamic nucleus, as the plasma osmolality rises you have a thirst drive. e. Two things happen as plasma osmolality increases: you will concentrate your urine due to ADH and you have a thirst drive f. Thirst is a normal part of the mechanism to regulate the plasma osmolality and volume. It is not a sign that you are dehydrated. Is there any disadvantage of taking in a lot of water? Not really. You will just increase your urine flow. If you are prone to kidney stones, it is recommended that you increase your water intake so that you keep your urine dilute and solutes don’t precipitate. It is also recommended for people who have a lot of urinary tract infections to try to flush the bacterial load in the bladder. g. If you are constantly taking in a lot of water then you decrease your ability of your body to react to dehydration. You suppress the synthesis of ADH and the synthesis of water channels in the DCT and CD. So if you suddenly become dehydrated then you have a decreased capacity to concentrate your urine. h. If you take in too much water you are going to create difficulties, any extreme is detrimental VIII. Large loss of ECF volume leads to ADH releases and thirst even if plasma osmolality is low [S9] a. A deficient in ECF volume will cause an increase in plasma ADH levels and you will concentrate urine maximally even if the plasma osmolality is dilute. b. The decreased signal of ECF volume will override the effect of osmolality on the release of ADH c. The levels of ADH release with significant ECF volume depletion are much higher than they are with just an osmotic release of ADH. The significance is that ADH will end up having an effect on blood pressure. It will tend to increase the blood pressure. d. This happens only if you have significant loss of ECF – when you are really dehydrated. In which case, you want to conserve volume, increase ECF volume, and total body volume and you may do it at the expense of the plasma osmolality. Renal: 11:00 - 12:00 Scribe: Teresa Kilborn Monday April 6, 2009 Proof: Hunter Neill Dr. Schafer Renal Physiology Page 3 of 4 e. Ex. if you have a GI upset (diarrhea and vomiting) then you are losing a lot of salt and water. They are being prompted to release ADH and they are putting out a maximally concentrated urine. They will retain water, but if you are not keeping down any solid food then the retention of the water will dilute their plasma. f. SQ: Refers to the first lecture when osmolality was described as staying the same during a loss of ECF, how does that occur if ADH is being released in such conditions that would then affect osmolality? Ans: you can lose isotonic volume by a hemorrhage and the osmolality of the body compartments wouldn’t change. During GI upset, you are losing isotonic fluid so plasma osmolality doesn’t go down, but it becomes diluted by this mechanism as consequence. The ECF volume goes down, you have ADH release, and you conserve water to the extent that it starts to dilute the plasma. The dilute plasma osmolality does not turn off the ADH release because the low ECF volume is an overriding stimulus. g. It also happens in CHF patients. These patients are retaining excessive amounts of salt and water and they are behaving as if their ECF volume is down even if they have extreme edema. These patients will produce a lot of ADH that will concentrate their urine and dilute their plasma which is a serious side effect. They may develop hyponatremia which is low salt/sodium concentrations in the plasma which can lead to arrhythmias and muscular excitability changes, coma and even death. IX. Hypertonicity of the inner medulla and the role of urea [S10] a. Why do we have the hypertonicity of the medulla? Why is there a high concentration of salt and urea in medullary interstitium? When you go up the thin and thick segment of the ascending loop of henle, the diluting segment, it makes the tubular fluid more dilute. There is passive sodium resorption in the thin inner medullary and active sodium resorption in the thick ascending limb. You are dumping salt in here without water because it is water impermeable. There is a rise in the sodium chloride concentration in the medullary interstitium because of this. b. 50% of urea is resorbed in the PCT. Urea concentration in the inner medullary interstitium is high and urea is picked up. The remainder of the loop from the tip to this region is urea impermeable, so all of the urea gets trapped in the tubular fluid. Urea concentration will rise in this region of the nephron. By the time you get to the macula densa the concentration of urea is about what it started. Then you resorb water and the concentration of urea in the tubular fluid rises. The urea concentration in your final urine is going to be much more than 600. It will make up most of the osmolality of the urine. There is a favorable concentration gradient of urea to move out of the tubule, but it doesn’t because this portion of the nephron is impermeable to urea until you get to the medulla where in anti-diuresis, an active transporter is activated. There is a passive diffusion mechanism that allows urea to diffuse out of the tubular fluid and into the medulla. The increased urea permeable allows urea to diffuse into the medullary interstitium and make it hypertonic. Also a reason that during diuresis you tend to lose urea in the medullary interstitium and the medullary interstitium osmolality will only rise to 600 instead of 1200. In diuresis you have dilute urine, there is not as much urea and it will move from the medullary interstitium to the tubular fluid, so you lose hypertonicity due to urea. X. Countercurrent exchange in the vasa recta [S11] a. How do you maintain the hypertonicity of the medulla interstitium when you have constant blood flow? Two reasons. First very little blood flow goes to the medulla. Only about 10% of the blood flow reaches the medulla and an even small amount reaches the papilla. Secondly, most of the circulation is arranged loops like the nephron, but here talking about the peritubular capillaries called vasa recta. The significance of the vasa recta loops is that as blood flows down these loops solute is going to enter (i.e. sodium, chloride, and urea) and that will make the blood hypertonic. If the blood went straight back to the vein from there it would have a high sodium, chloride, and urea concentration, but instead it travels back up through the ascending region of the vasa recta and it does so it enters a region of lower concentration of salt and urea in the medulla interstitium in which it equivocates to. b. What goes back to circulation through the renal vein does have a slightly higher concentration because not all of the salt and urea that is resorbed in the deceasing limb is excreted during the ascending limb. But you want this to maintain balance. In the steady state, the amount that is being returned via the blood matches the amount that is being added by the nephron. c. Low blood flow and the countercurrent flow of blood is what establishes and maintains the high osmolality of the plasma medulla interstitium XI. Response to water deprivation [S12] a. Someone sweating excessively or in a desert will lose water that will result in a rise in plasma osmolality that stimulates the release of ADH from the posterior pituitary. This can also be triggered by a fall in ECF volume. b. ADH increases the water permeability of the distal regions of the nephron and the distal collecting duct and water resorption increases which causes a high urine osmolality and a decrease in urine volume which tends to bring plasma osmolality back to normal. You’re excreting more solutes relative to water. Renal: 11:00 - 12:00 Scribe: Teresa Kilborn Monday April 6, 2009 Proof: Hunter Neill Dr. Schafer Renal Physiology Page 4 of 4 c. The fall in plasma osmolality is going to signal for thirst which will cause you to drink and tend to restore plasma osmolality. d. For people that have access to water, even if ADH mechanism doesn’t work like in people with central diabetes insipidus where they can’t concentrate their urine, they can still maintain water balance via the thirst mechanism. Diabetes is another word for high urine flow rate. People with central diabetes insipidus produce 12-18L of urine a day. e. You have to have problems with both limbs of the water balance mechanism to get hyperosmotic plasma. XII. Response to water excess [S13] a. If you are taking in a lot of water, then it dilutes the plasma osmolality and you inhibit the osmotic receptors that have nerve endings in the hypothalamus so they cause a decrease in the release of ADH and a decrease in the water permeability of the late distal tubule and collecting duct. This leads to a decreased water resorption so a low urine osmolality and a high urine out flow. A dilute urine will increase the plasma osmolality back to normal. b. The excess water and low plasma osmolality will suppress the thirst drive, you’ll drink less, and that will also help to bring plasma osmolality back to normal. c. SQ: Can you drink too much water? Ans: You can. You can poison yourself by drinking too much water. If you take in too much water you can increase the amount you secrete in your urine, but you reach a limit even if you are suppressing ADH and producing 12-18 L of urine/ day. Eventually your sodium concentration will fall and you’ll have effects on neuromuscular excitability and CNS effects. First you will feel confused and disoriented. Then seizures and coma. This is especially true when it happens over a short period of time. What is happening is that the cells in your brain are swelling and there is only a limited amount of space in the cranium so they start putting pressure on the neurons of your brain. d. SQ: As long as the amount you’re drinking is not exceeding the amount you’re peeing then you won’t have any problems? Yes. If you are taking in a lot of water; however, you may not to be able adjust as quickly as a normal individual would if you suddenly stop taking in water. XIII. Key Points- Body Water Balance [S14] - Read of slide XIV. Daily Na+ intake [S15] a. We take in about 8-15 g/day which is 150-250 mmol/day b. If you don’t add any salt to your food, then you can decrease your intake to 70-120 mmol/day c. If you don’t add it when you’re cooking then you can decrease your intake to 50-70 mmol/day d. If you are on a low salt diet then typically you have to avoid dairy products, meat, cheese, all processed foods, canned foods, lunch meats, etc. e. It’s difficult to get someone to adhere to a low salt diet. f. Prepared foods typically have high contents of salt because it makes it taste better. You have to avoid prepared foods if you want to lower your salt intake. XV. Na + intake affects ECF volume and body weight [S16] a. Sodium is the main ion in the ECF. b. When we talk about salt balance, we’re really talking about trying to maintain an ECF volume. c. If you take someone who is on a low salt diet and you suddenly raise their salt intake, the salt regulation system is slow, so you will have a period of positive sodium balance. d. Then if you suddenly reduce their amount of salt intake, there is a lag again for the body to catch up so there is a gain of ECF volume because you are retaining more salt which makes your thirsty and you take in more water. e. These changes are reflected as a change in body weight, usually most changes in body weight over a short period of time are due to how much salt you are taking in or excreting because of a change in the ECF volume XVI. Na+ handling in the nephron [S17] a. 2/3rds of sodium is resorbed in the PCT. 25% in the thick ascending limb. A much lower amount in the DCT and only 3% in the late DCT and CD. XVII. Aldosterone action on principal cells [S18] a. This is where we have a regulation of salt by aldosterone in the principal cells of the late distal tubule and the CD. b. Aldosterone binds to a nuclear receptor that increases the production of sodium channels, potassium channels, sodium potassium ATPase, and stimulates Kreb cycle enzymes. c. This increases sodium resorption- returning it to the blood and increases potassium secretion. d. This receptor can be blocked by another type of potassium sparing diuretic called Spironolactone that is a competitive inhibitor. XVIII. Key points- Body Salt (Na+) Balance [S19] a. Read off slide. b. Some individuals are sensitive to salt intake that causes their blood pressure to rise when that take in extra salt. [End 47:38]