Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
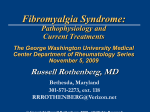
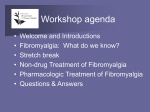
Fibromyalgia… Fiend or Feigned? Ted D. Williams Pharm D PGY1 Resident Syracuse VAMC May 2010 Outline • • • • • Spectrum of Disorders Proposed mechanisms Co-morbidities Assessment and diagnosis of fibromyalgia Evidence review on the treatment of fibromyalgia – Non-pharmacotherapy – Pharmacotherapy What is Fibromyalgia? • Chronic Pain Syndrome – A group of symptoms • Generalized pain • Specific trigger points • Etiology poorly understood • Treatments are of questionable efficacy • Several new medications have received FDA indications for the treatment of Fibromyalgia – Duloxetine (Cymbalta®) – Pregabalin (Lyrica®) – How do these Non-Formulary medications compare with formulary alternatives? Spectrum of Disorders Where does fibromyalgia fit? Organic Disease e.g. appendicitis Somatic Disorders Myogenic Disorder Physical manifestation of mental disturbances Conscious or unconscious Production of pseudo-neurologic symptoms Factitious Disorders Or Malingering Faking for psychosocial or financial gain Disparity between stated symptoms and physical findings Pain Phases Limbic Structures Periaquiductal Gray (PAG) Thalamus NRPG 1. 2. 3. 4. Cortex Initiation Transmission Perception Reaction NE (Alpha-2) NRM Locus Ceruleus NE 5HT Voltage-Sensitive Sodium Channels Stimulus Dorsal Horn (Pain Gate) Nociceptors Prostaglandins Proposed Mechanisms of Fibromyalgia • Intensely studied, poorly understood • Muscular – Strength deficits and atrophy are explained by de-conditioning • Hyperalgesia • Hypervigilance • Somatization Hyperalgesia • Studies extensively • Literature replete with positive findings • Results have poor repeatability, many confounders, small sample size, etc. • Lautenbacher S; Rollman GB. Possible deficiencies of pain modulation in fibromyalgia. Clinical Journal of Pain. 1997;13:189-96 • Staud, Roland. Abnormal Pain Modulation in Patients with Spatially Distributed Chronic Pain: Fibromyalgia. Rheum Dis Clin North Am. 2009;35: 263–274 Hypervigilance • Generalized Hypervigilance Hypothesis (GHH) – Theorizes that all noxious stimuli (tactile, auditory, etc) are amplified – Centrally mediated process, rather than peripheral pain derangement – Some support, but mixed results on non-tactile stimuli • Lollins, M, Harper, D, Gallagher, S et al. Perceived Intensity and Unpleasantness of Cutaneous and Auditory Stimuli: An Evaluation of the Generalized Hypervigilance Hypothesis. Pain 2009;141;215-221 Comorbidities of Fibromyalgia • Mood Disturbances – Concurrent depression at diagnosis 30% – Lifetime prevalence • Depression 74% • Anxiety Disorder 60% • Non-Restorative sleep nearly universal • Veterans – OR 2.32 in deployed vs. non-deployed Gulf War veterans after 10 years – OR 3.00 in female veterans with PTSD vs. without PTSD • Perrot, S., et al. Fibromyalgia: Harmonizing science with clinical practice considerations. Pain Practice 2008;8:177-189 • Eisen, et al. Gulf war Veteran’s Health: Medical evaluation of a U.S. cohort. Annals of Internal Medicine 2005:142:881-890 • Dobie, et al. Posttraumatic Stress Disorder in female veterans: Association with self-reported health problems and functional impairment. Archives of Internal Medicine 2004;164:394-400 Somatization? • There is good evidence that NE/5HT plays a important role in management of Fibromyalgia • Are there underlying genetic polymorphisms in NE and 5HT receptors or reuptake inhibitors or metabolism that make patients susceptible to both mood disturbances and fibromyalgia? • The debate rages on… Summary of Fibromyalgia Pathophysiology and Etiology • Fibromyalgia pain appears to be mediated by neurotransmitters (NE,5HT) involved mood and sleep • Fibromyalgia pain manifests peripherally, but appears to be centrally mediated • Rational pharmacotherapy should focus on targets of norepinephrine, serotonin, and voltage-gated sodium channels Diagnostic Criteria of Fibromyalgia • 1990 ACR Criteria – The combination of • widespread pain • mild or greater tenderness in 11 of 18 tender points – Sensitivity of 88.4% – Specificity of 81.1% Applying enough pressure to whiten the examiner's fingernail bed generates approximately 4 kg/cm2 of pressure • Wolfe, A. et al. The american college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis and Rheumatism 1990; 33:160 - 172 Adding Fibromyalgia to the problem list • Fibromyalgia is not equal to generalized pain • Treatment of fibromyalgia is different than other pain syndromes • Verify the source of the problem list item – Chart Lore – Patient Reports – Specialty clinics • Diagnosis should come from Rheumatology Fibromyalgia Prognosis • “Patient with established fibromyalgia, seen in rheumatology centers in which there is a special interest in the disease and followed up for as long as 7 years, have markedly abnormal scores for pain, functional disability, fatigue, sleep disturbance, and psychological status, and these values do not change substantially over time.” – Wolfe, A. et al. Health status and disease severity in fibromyalgia. Arthritis and Rheumatism 1997;40:1571-1579 • “If treatments do not work in a sustained and useful way, they should not be used.” – Wolfe, A. Letter to the editor regarding: Management of Fibromyalgia. Annals of Internal Medicine 1999;131:850-858 Assessment of Fibromyalgia • Fibromyalgia Impact Questionnaire (FIQ) – – – – – Activities of Daily Living (ADLs) Pain at various times Fatigue Anxiety Mood • Self assessment • Easy to use, and provides more information than simple pain scores • Very sensitive to changes in perceived pain and functional status • Bennett, R. The Fibromyalgia Impact Questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clinical and experimental rheumatology 2005:S154-162 Goals of Fibromyalgia Therapy • Primary Goal: – Improve Functional Status • Secondary Goals: – Reduce Pain – Streamline therapy • Tertiary Goals: – Manage resource utilization • e.g. limit unnecessary testing, and visits • Usually involved setting up scheduled, frequent visits with the appropriate provider • Perrot, S. Dickenson, AH, Bennett, RM. Fibromyalgia: Harmonizing Science with Clinical Practice Considerations. Pain Practice 2008;8:177–189 • Wolfe, A. et al. Health status and disease severity in fibromyalgia. Arthritis and Rheumatism 1997;40:1571-1579 • Hughes G, Martinez C, Myon E, Taieb C, Wessely S. The impact of a diagnosis of fibromyalgia on health care resource use by primary care patients in the UK: an observational study based on clinical practice. Arthritis Rheum.2006;54:177–183. Treatment Strategies • Non-Pharmacological – Patient Education – Cognitive Behavioral Therapy (CBT) – Sleep Hygiene – Occupational/Physical Therapy • Pharmacological – Depression/Anxiety Management – Pain Management Non-Pharmacological Treatment – Primary Treatment Mode • Patient Education – Nature of the disease and disease course – Modes of therapy (Physical, behavioral, pharmacologic) – Goals of therapy (ADL, pain) • Cognitive Behavioral Therapy (CBT) – Improvements in sleep (50% reduction in sleep disturbances) – Improvements in functional status – Effects persist while therapy continues • Sleep Hygiene – Simple sleep hygiene counseling improves symptoms, but not as much as more intensive CBT • Physical Therapy – Improves functional status but not mood – Effects more persistent after discontinuation of therapy than CBT • Thompson, PA, et al. Effects of a 1.5 day multidisciplinary outpatient treatment program for fibromyalgia. American Journal of Medical Rehabilitation 2003;82:186-191 • Edinger, JD et al. Behavioral Insomnia therapy for fibromyalgia patients. Archives of Internal Medicine 2005;165:2527-2535 • Redondo, JR. et al. Long-term efficacy of therapy in patients with fibromyalgia: A physical exercise-based program and a cognitive-behavioral approach. Arthritis and Rheumatism. 2004;51:184-192 Pharmacological Treatment • Mood Management • Pain Management Formulary Requirements • For moderate-to-severe fibromyalgia: – Pregabalin • restricted to non-response to – – – – – max-tolerated gabapentin up to 3,600mg/day Amitriptyline Fluoxetine Venlafaxine Tramadol + APAP • along with exercise and cognitive behavioral program – Duloxetine • For moderate-to-severe fibromyalgia: • Pregabalin is preferred • Let’s see what the evidence supports… Tricyclic Antidepressants • JAMA 2009 Meta Analysis – Doses studies were amitriptyline 12.5mg-50mg daily • One nortriptyline study – Strong evidence for reduction in • • • • pain fatigue mood sleep disturbances – TCAs had the largest effect size of all antidepressants – Durability of Response • Most studies were less than 12 weeks • One study of 26 weeks found no significant change in pain vs. placebo • Leventhal suggested a “holiday” to restore efficacy in case of tachyphylaxis • Hauser, W, Bernardy, K, Uceyler, N, Sommer, C. Treatment of fibromyalgia syndrome with antidepressants: a meta analysis. JAMA 2009;301:198-209 • Leventhal, LJ. Management of Fibromyalgia. Ann Intern Med. 1999;131:850-858. SNRIs • Duloxetine – 2009 JAMA meta analysis of antidepressants in fibromyalgia • Improvements found in – Pain – Mood – Sleep • No effects found on – Fatigue • Effect size smallest in SNRIs and SSRI – Russell, IJ, et al. Pain 2008 • No clear dose-response relationship between 20mg, 60mg and 120mg daily doses • Venlafaxine – Cites a single RCT showing no benefit • Phantom Reference , no such article in the journal +/- 2 years, nothing in OVID search of all journals – Open label trials suggest possible benefit – Evidence is lacking • Hauser, W, Bernardy, K, Uceyler, N, Sommer, C. Treatment of fibromyalgia syndrome with antidepressants: a meta analysis. JAMA 2009;301:198-209 • Russell, IJ, et al. Efficacy and safety of duloxetine for treatment of fibromylagia in patients with or without major depressive disorder: Results from a 6 month, randomized, double-blind, placebo-controlled, fixed dose trial. Pain 2008;136:432-444 • Goldenberg, et al. Management of Fibromyalgia Syndrome. JAMA 2004;292:2388-2395 SSRI • 2009 JAMA meta analysis of antidepressants in fibromyalgia – Hauser, W, Bernardy, K, Uceyler, N, Sommer, C. Treatment of fibromyalgia syndrome with antidepressants: a meta analysis. JAMA 2009;301:198-209 – Studies were of • Fluoxetine 20-80mg • Paroxetine (mean 40mg) • Citalopram 20-40mg – Improvements found in • Pain • Mood – No effects found on • Fatigue • Sleep – Effect size smallest in SNRIs and SSRI – These data suggest it isn’t just a mood disorder, otherwise SSRIs would be great! Antiepileptics • Pregabalin FDA Approved – Doses below 300mg daily ineffective – Most sustained effect at 450-600mg daily • Gabapentin off label – 1200-2400mg daily • Hauser, W. et al 2009 – 30% pain reduction NNT • Gabapentin 5 • Pregabalin (>=300mg/day) 6.6-9.4 – Significant improvement in pain and FIQ for both gabapentin and pregabalin • Hauser, W. Bernardy, K, Uceyler, Sommer. Treatment of fibromyalgia syndrome with gabapentin and pregabalin – a meta-analysis of randomixed controlled trials. Pain 2009;145:69-81. Opioids • No studies have demonstrated efficacy of opioids for the treatment of neuropathic or fibromyalgia pain • Sullivan, MD, Edlund, MJ, Steffick, D, Unutzer, J. Regular use of prescribed opioids: association with common psychiatric disorders. Pain 2005;119:95-103. – Presence of mood disorders is a strong predictor of opioid use • (OR 3.15 CI 1.69-5.88, p<0.001) – Presence of Panic disorder OR 8.46 • PTSD not reported – Drug abuse disorder OR 4.75 • Mood disorders were historically treated with opioids • Some evidence for efficacy of opioids for refractory depression and OCD • Patients may report feeling better, but risk-to-benefit must be considered • Tramadol Synthetic Opioids – Has SNRI activity • R,R (+) isomer – SERT antagonist • S,S (-) isomer – NERT antagonist – Low opioid activity – Demonstrated superior to placebo in improving FIQ and time to discontinuation • Tramadol/Acetaminophen 75mg/650mg 4x/day • Tapentadol – new in 2009 – Has NERT activity, with slight SERT activity – Strong opioid affinity – No studies in neuropathic or fibromyalgic pain • Bennett, RM, Kamin, M, Karim, R, Rosenthal, N. Tramadol and Acetaminophen Combination Tablets in the Treatment of Fibromyalgia Pain: A Double-Blind, Randomized, Placebo-Controlled Study. The American Journal of Medicine 2003;114:537-545 NSAIDs & Prednisone • Goldenberg DL; Burckhardt C; Crofford L. Management of Fibromyalgia Syndrome. JAMA 2004;292(19):2388-95. – No more effective than placebo Other Agents • Pramipexol • Carisoprodol • Sodium oxybate EBM & Formulary Synthesis • Parallel, complimentary Pathways • Adequate trials 8 weeks – SSRI Remodeling – Side effects are bothersome – Timing, FIQ, and titration are essential – If not effective, discontinue • First Line – TCA (NE, 5HT, Sleep) – Gabapentin (VSSC) • Second Line – Tramadol (NE, 5HT) – SSRI (5HT) – Pregabalin (VSSC) NE 5HT VSSC Amitriptyline 12.5mg QHS May Titrate to 50mg QHS SSRI at Standard Dose Tramadol 75mg QID • Third Line – Duloxetine (NE) Venlafaxine is formulary preferred, but has little evidence to support its use Gabapentin Titrate to 400-600mg TID Duloxetine 20-120mg QD Pregabalin Titrate to 100-200mg TID Hot Potato – Who manages Fibromyalgia? Rheumatology (+) Diagnosis (-)No Immunological Component Behavioral Health Pain Clinic (-) Opioids are not useful (-) Effective pharmacotherapy affects Behavioral Health treatment (+) Psychiatric/behavioral comorbidities (+) Tx are CBT & psychoactive medications (-) Patients dislike implications Summary • Therapy Goals – Fibromyalgia is a chronic pain disorder with a poor prognosis – Therapy goals should be improvements in ADL, not necessarily pain score – Sleep and mood management are essential • Pharmacotherapy – Complimentary mechanisms of action should be used in accordance with Formulary Guidelines • TCAs and Gabapentin • SSRI/SNRI/Tramadol and Pregabalin – Opioids have no place in fibromyalgia therapy • No demonstrated efficacy in reducing pain scores • But patients do feel better • Therapy Management – Assessment tools like FIQ are easy to use and can help compare overall function from one medication to the next – If an agent isn’t effective after 8-12 weeks, discontinue, don’t just add on – Multidisciplinary coordination is essential to provide maximum benefit and to control healthcare utilization