Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
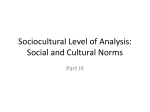
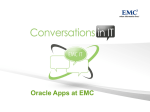
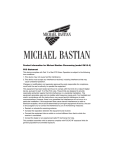
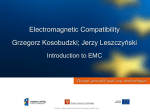
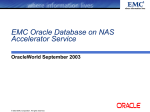
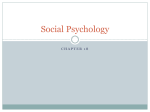
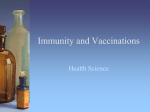
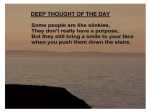
FEATURE www.conformity.com EMC For Medical Devices: A Review Of IEC 601-1-2, 2nd Edition Significant changes from the earlier version of this standard make testing more complex I n the European Union (EU), medical equipment marches to a different beat than other types of equipment in the areas of EMC and product safety. The reasons lie in several areas: regulatory, philosophical, and in the standards used. The first step in understanding the contrasts between the requirements imposed on medical products versus other types such as telecom and information technology equipment (ITE) is to look at the governing directives. Both ITE and medical equipment are governed by so-called “New Approach” directives. Under the New Approach, equipment must meet whatever directives apply to it to gain entry to the EU’s market; compliance is indicated by the application of the CE mark and the documentation of the steps taken to meet the applicable directives. The steps taken, of course, vary with each directive, and will include a combination of testing, documentation and, in some cases, notified body supervision of ongoing production and manufacturer quality systems. Most product directives set overall goals and methods for assessing responsibility, but leave detailed technical requirements to standards which are generated by international groups such as the IEC, CEN/CENELEC, and the ISO (a few directives contain the technical requirements without reference to external standards). These standards gain regulatory force—that is, become suitable for demonstrating conformity to a given directive - upon publication by the European Commission in the Official Journal of the European 12 CONFORMITY ®: JULY 2003 Isidor Straus Union. An up-to-date posting, organized by directive, is maintained on the Internet can be found at the following URL: http://europa.eu.int/comm/enterprise/ newapproach/standardization/harmstds/reflist.html Most of our readers are familiar with the EMC Directive (89/336/EEC) and the Low Voltage Directive (73/23/EEC). These govern the electromagnetic performance and safety of most electrical and electronic equipment. Both directives are generally applicable unless superseded by a “specific directive.” The Directive on Medical Equipment (93/42/EEC) and the related Directive on in-vitro medical devices (98/72/EC) are just such specific directives. Standards Overview For Medical Equipment And Devices A large number of standards have been designated and published for assessing compliance under these directives. These include a number that are highly specific to the construction and operation of particular device types, such as ophthalmic, respiratory, and x-ray equipment. In addition, there is a large family of standards, grouped under the EN 60601-x-x designation, which address the issues of EMC and safety that, in the absence of these overriding directives, would be addressed by the EMC and LVD requirements. FEATURE www.conformity.com The 60601 family is concerned with the safety of medical electrical equipment. The standards are grouped in two parts. Those numbered “–1-x” are considered relevant to the general requirements for safety, and are labeled “collateral standards.” Those numbered “-2-x” contain requirements for specific kinds of medical equipment. Some examples should make this clear: Table 1: Table 201 from the standard ● EN 60601-1-1 is entitled “Medical electrical equipment – Part 1-1: General requirements for safety. Collateral standard: safety requirements for medical electrical systems.” This is the primary safety standard containing requirements applicable to most types of equipment; the “Part 2” standards are far more specific. ● EN 60601-1-2 is entitled “Medical electrical equipment – Part 1-2: General requirements for safety. Collateral standard: Electromagnetic compatibility – Requirements and Tests.” This is the primary focus of this article. ● EN 60601-2-2 is entitled “Medical electrical equipment – Part 2-2: Particular requirements for the safety of high frequency surgical equipment.” This is an example of a product-specific standard. There are several dozen of these. From this, we see that EMC comes to be regulated under the Medical Directive(s) as part of a family of safety standards. This influences the requirements of EN 60101-2-2. EMC is viewed in the context of safety and clinical function. Table 2: Table 202 from the standard 14 CONFORMITY ®: JULY 2003 The demonstration of EMC compliance for medical equipment, which is covered by a “specific” directive, differs from the more familiar procedure used under the EMC and LVD Directives. For those, self-certification is the method of compliance; a test report is generated, and on that basis, the manufacturer CE marks his product and asserts compliance with a declaration of what directives and standards were applied. FEATURE Most medical products do not undergo self-certification. Rather, a Notified Body reviews medical, quality, and other data, including the EMC and product safety reports and generates a certificate of compliance, which forms the basis for CE marking. EMC Under The Medical Directive At present, EMC compliance can be demonstrated using two versions of EN 60601-1-2. Either the 1993 version or the 2001 version may be employed. EN 60601-1-2:2001 was officially designated for the Medical Directive on December 13, 2002. There is a period of overlap, until November 1, 2004, when either version of the standard may be used for assessing conformity. It is important to note that there is no grandfathering for equipment assessed to the old standard after that date; the presumption of conformity ceases, which would require retesting to the new standard for equipment imported into the EU after than date. Thus, for equipment with any reasonable expected life, the later standard should be used. EN 60601-1-2:2001, draws on well known EMC standards used by the EMC Directive, but adds a lot of interpretive information and documentation requirements. It differs from the 1993 standard, and from most EMC Directive standards in two key ways: ● Relative to the 1993 standard, there has been a shift to current EMC standards and methods. The 1993 standard was based on the older IEC 801 series of EMC standards; the new one uses the IEC/EN 61000-4-x series that has matured in the intervening years, as well as the harmonic and flicker requirements, IEC 1000-3-2 and IEC 1000-3-3. ● Documentation requirements—the information that must be supplied to the user—are greatly increased in quantity and detail. Described in Section 6.8.201 of the standard, these include: A series of warnings and markings. These include general information on EMC, the effects that RF communications can have on medical equipment, markings of ESD sensitive connectors (which have been excluded from pin discharges) and series of warnings concerning them, and information on required physiological signal levels and warnings on the effect of low levels on accuracy Detailed listing of all accessories which can affect compliance, including cables and their maximum allowed lengths, as well as allowed transducers Circle Reader Service #8 or go to www.conformity.com/INFODIRECT CONFORMITY ®: JULY 2003 15 FEATURE Table 3: Comprehensive list of EN 60601-1-2 EMC requirements 16 CONFORMITY ®: JULY 2003 www.conformity.com FEATURE A detailed, standardized table running some 10 pages, which lists the types and levels of EMC performance the product is capable of, and gives instruction on the proper environments for operation. The tables follow the qualification test plan. Tables 1 and 2 show a portion of the information required. Table 1 is an emissions performance table that is filled in for the particular equipment with the aid of the flowchart in Figure 1. Similarly, Table 2 is a table covering some of the immunity modalities, while Figure 2 is a graphical guide to completing it. Note that for equipment which does not meet the suggested levels, instructions on what steps must be taken to control environmental EMC to achieve the same level of product functionality must be included. For example, for equipment with low RFI immunity, a shielded room might be suggested. A Closer Look At The Requirements The basic technical requirements are shown in Table 3. There are actually two tables—one set of requirements for life-supporting equipment, and another, with lower RFI immunity requirements, for non-life supporting equipment. At first glance, the table should look quite familiar to those used to the generic EMC standards, or the product specific telecom and information technology (ITE) requirements. The standard tests are applied. However, EN 60101-1-2 incorporates important differences in the definition of what constitutes acceptable performance and in a number of test application conditions. The issue of acceptable performance is both important, yet potentially tricky in interpretation. The general requirements Circle Reader Service #9 or go to www.conformity.com/INFODIRECT (section 3.201) contain the usual limits on controlling electromagnetic interference that could affect radio communications or other equipment, along with an immunity requirement that is more carefully drawn than in the default EMC Directive. This requirement is that the “essential performance” of the equipment shall have adequate immunity to electromagnetic disturbances. The term “essential performance” is discussed in the following paragraph (3.201.2) and in the definitions (Paragraph 2). The “essential performance” is defined as those “characteristics necessary to maintain the residual risk within acceptable limits.” Prior to EMC immunity testing, it is strongly suggested that an EMC risk analysis be performed. All functions – defined as those operating modes of clinical significance – should be considered. If this risk analysis is Circle Reader Service #10 or go to www.conformity.com/INFODIRECT CONFORMITY ®: JULY 2003 17 FEATURE performed, the equipment is to be tested in the mode (and with operating settings and configuration) that is most critical from the perspective of the patient. If this risk analysis is not performed, all modes must be tested. Documentation of the test must include details of the test methods, equipment configuration, operating mode and the state of controls, the use of any www.conformity.com physiological or other signal simulators and accessory equipment, and when necessary, justification for any deviations from prescribed methods or levels of performance. There is an explicit list of performance degradations associated with essential performance and safety that are proscribed (“compliance criteria,” paragraph 36.202.1(j)): ● component failures ● changes in programmed parameters ● resetting to factory defaults ● changes of operating mode ● false alarms ● cessation or interruption of intended operation, even if accompanied by alarm ● inaccuracy (error of displayed numerical data) large enough to affect diagnosis or treatment ● noise, signal artifact, or distortion interfering with interpretation of physiologically produced signals ● failure of automatic diagnosis or treatment equipment to diagnose or treat, even if accompanied by alarm Clearly, the emphasis is on the maintenance of clinical function in the anticipated electromagnetic environment. EN 60601-1-2:2001 replaces a prior edition dating back to 1993. In the world of EMC standards, a lot has happened, with many EMC standards having been developed and/or revised. We estimate that testing to the new edition takes 50% to 75% more time than testing to the 1993 edition, due to the increased in the number of tests required and the more careful specification of acceptable function. Let’s look at some specifics. In the area of tests required and test levels, many changes have occurred. The IEC 801-x immunity standards were used in 1993. They have been replaced by the IEC/EN 61000-4-x and IEC/EN 61000-3-x requirements. This brings in several new tests that were not performed under the 1993 edition: Figure 1: Instruction flowchart matching table 201 18 CONFORMITY ®: JULY 2003 ● Harmonics and flicker (IEC 61000-32 and –3) ● Conducted RFI (IEC 61000-4-6), from 0.15 to 80 MHz ● Power Frequency Magnetic Field (IEC 61000-4-8) ● Voltage dips and interrupts (IEC 61000-4-11) FEATURE In addition, for several of the tests that were previously performed, there have been some changes in the levels that equipment is required to meet. ● ESD: Levels have been increased for contact discharge from 3 kV to 6 kV. Also, connector pins are only exempted from discharge if they are marked with an ESD sensitivity symbol ● RFI radiated: The frequency range for radio frequency susceptibility testing has changed. It was 27 – 1000 MHz; now, it is 80 – 2500 MHz. The change at the lower end is due to the introduction of conducted RFI requirements. At the high end, the frequency range has been extended, in part because of the expanding use of equipment at higher frequencies, especially in the cellular and networking arenas. Figure 2: Instruction flowchart matching table 202 Circle Reader Service #11 or go to www.conformity.com/INFODIRECT FEATURE ● EFT (electrical fast transient): The test levels for non-permanent AC wiring (i.e., the wall plug) have been doubled from 1 to 2 kV; DC power leads, formerly exempt, are now subject to a 2 kV level, and the test level for I/O leads has been doubled from 0.5 to 1 kV. For equipment capable of operating at multiple supply voltages, including autoranging, the test is repeated at minimum and maximum voltages. ● Medical equipment has been divided into two categories—life supporting and non-life supporting. Life supporting equipment is subject to more stringent requirements in several areas, including RF immunity (see Table 3) and voltage dips and interrupt performance. The categorization of life- and non- lifesupporting equipment existed in the previous edition, but the differences in required performance are now more marked. www.conformity.com Perhaps the most important changes concern the test methodology. Because medical equipment is specialized, and because clinical function is of paramount concern, a number of changes have been introduced in the way several tests are performed. Here are the most noteworthy: ● Equipment Configuration Guidelines: The general guide is that equipment is to be configured for immunity testing in the manner which is likely to make it most susceptible to interference. Within the normal parameters of operation, gain should be maximized, and any input signals, such as simulated physiological signals, should be at the minimum levels. Consideration should be given to monitoring essential functions, whether in software or hardware, that are not observable in normal operation. The Annex gives an example for a dialysis machine. These machines contain bubble detector alarms, which are operated by viscosity or acoustic detection. These internal measurements could be affected during immunity testing, inhibiting bubble detection and, hence, some method of ensuring proper function must be devised. Care has to be taken in termination of equipment leads and connection to simulation that the operating conditions under test are representative of normal operation. Patient connected leads are given special attention: they are not to be connected to CDN devices, and should use the standardized RC termination (including, where applicable, the “artificial hand”) of CISPR 16-1. ● Radiated and Conducted Immunity: These tests are usually carried out with 1 KHz amplitude Circle Reader Service #12 or go to www.conformity.com/INFODIRECT 20 CONFORMITY : JULY 2003 ® FEATURE modulation. Physiological signals, such as those associated with pulse and respiration, have significant amplitude at lower frequencies. The standard mandates that a different modulation rate be used for these signals. Specifically, where physiological functions are measured or controlled these immunity tests should be performed with a 2 Hz amplitude modulation. Shifting to a lower modulation rate also influences (lengthens) the rate at which the test is performed. Both the radiated and conducted tests span a wide frequency range. This range can either be scanned digitally, in increments of no more than 1%, or continuously. With the normal 1 kHz modulation rate, the minimum dwell time for discrete frequency steps is the longer of either settling time of EUT plus settling time of test setup, or 1 second. With 2 Hz modulation, the minimum dwell time is at the greater of the settling time or 3 seconds. With continuous modulation, the sweep time must be no greater than 4.5 x 10 -3 /X decades per second, where X is the dwell time for a discrete 1% step. In other words, the speed at which the tests can be conducted is related to the types of signals processed by the equipment. Circle Reader Service #13 or go to www.conformity.com/INFODIRECT Circle Reader Service #14 or go to www.conformity.com/INFODIRECT CONFORMITY ®: JULY 2003 21 FEATURE Another test issue concerns how to deal with frequencies within the range of those tested where the equipment is intentionally designed to be sensitive. Obviously, a strong RF signal would produce a response. The solution is to establish an exclusion band around the sensitive frequency or frequency www.conformity.com band. For signals below 80 MHz (which corresponds to the conducted immunity test), the exclusion extends +5% and –5% above and below the affected frequency range. For signals above 80 MHz (which corresponds to the radiated immunity test) the exclusion band is widened to +10% above and –10% below the sensitive frequency range. ● Dips and Interrupts: The voltage dips and interrupts of EN 61000-4-11 are applied, but the performance criteria vary depending on the power drawn by the equipment and whether Test and Equipment Mains Power or Current Non-Life Supporting Life Supporting Dips, <1kVA Must function normally Must function normally Dips, >1 kVA, <16 Amps/phase No damage, operator resettable (IEC criterion C) Must function normally Dips, >16 A/phase No Requirement for testing power dips No damage, operator resettable, alarm if function affected (IEC Criterion C plus alarm) Interrupts (All Powers) No damage, operator resettable. (IEC Criterion C) No damage, operator resettable, alarm if function affected (IEC Criterion C plus alarm) Table 4: Dips and interrupts (EN 61000-4-11) requirements for medical equipment Circle Reader Service #15 or go to www.conformity.com/INFODIRECT 22 CONFORMITY : JULY 2003 ® FEATURE the equipment is considered to be life supporting, as shown in Table 4. For dips, all equipment drawing less than 1 kVA must be unaffected and continue to operate normally. Between that power level and 16 Amps of mains current, life supporting equipment must still be unaffected, but non-life supporting equipment need only be undamaged and restartable with operator intervention. Higher power equipment that is life-supporting must either continue operating, or signal problems with an alarm; if non-lifesupporting, there is no requirement. For 5 second interrupts there is a similar division in requirements. Nonlife-supporting equipment need only be undamaged and restartable with operator intervention; life-supporting equipment must signal an alarm if any essential function is affected. Summing Up If you are involved in the design or compliance aspects of medical equipment, you need to be familiar with EN 60601-1-2. The 2001 edition is now in effect, and the 1993 version will not be valid after November of 2004. A considerable number of differences exist between the requirements of the new and the old editions of the standard. For those familiar with compliance testing of other equipment, but less familiar with the special requirements for medical devices, there are a lot of wrinkles in test methodology, test planning, and required documentation, which we’ve reviewed in this article. THE SHOW IS COMING! THE SHOW IS COMING! And Conformity is ready for it! Watch for your August issue containing the special IEEE EMC Symposium Show Supplement. About The Author Isidor Straus is the Executive Editor of Conformity. He can be reached at [email protected]. Don’t forget to visit us at Booths 528 & 530 AUGUST 18-22, 2003 Circle Reader Service #16 or go to www.conformity.com/INFODIRECT CONFORMITY ®: JULY 2003 23