Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
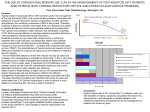
Tear functions in patients with pterygium Sibel Çalışkan Kadayifçilar*, Mehmet Orhan & Murat İrkeç Department of Ophthalmology, University of Hacettepe, Ankara, Turkey ABSTRACT. Purpose: In the etiology of pterygium abnormalities in tear functions have also been emphasized. In this study, tear function tests are evaluated in patients with pterygium. Methods: Schirmer’s test 1, tear film break-up time and mucus fern patterns were evaluated in 70 eyes with pterygium and in 70 eyes of the age matched control group. Marginal tear films were also assessed. Results: Tear film break-up time was significantly reduced in the pterygium group. Mucus fern patterns and marginal tear films were found to be markedly abnormal in the eyes with pterygium, however, there was no significant difference in Schirmer’s test 1. Conclusion: Tear function tests disclosed disrupted tear film stability which is more likely to be due to the altered mucin. This change may either be the primary factor inducing pterygium formation or reflect an existing pathology in the cells lining the ocular surface. Key words: pterygium – Schirmer’s test 1 – tear film break-up time – mucus fern test – mucin. Acta Ophthalmol. Scand. 1998: 76: 176–179 Copyright c Acta Ophthalmol Scand 1998. ISSN 1395-3907 A pterygium is a degenerative corneal limbal process which may progress onto the cornea in the interpalpebral area (Jaros & DeLouise 1988). Despite several theories, its etiology has not been adequately explained. Prolonged exposure to ultraviolet (UV) light has been implicated in the pathogenesis of pterygium (Hill & Maske 1989; Taylor et al. 1989, 1992; Adamis et al. 1990; Mackenzie et al. 1992; Coroneo 1993; Kwok & Coroneo 1994). One study performed in British Columbia, northern India, Thailand and Taiwan revealed that the ageadjusted prevalence rate of pterygium in sawmill workers – who worked indoors – was 25.3% compared to 7.1% in controls (Detels & Dhir 1967). This study provided evidence that the cause of the pterygium may be multifactorial. Mechanical irritation by dust particles and/or tear function abnormalities have also been proposed as etiologic factors (Coroneo 1993). Disruption of the tear film has been suggested to be the result of either rapid 176 evaporation or microtrauma from microparticles of dust or ice (Taylor 1980). In this study tear functions were investigated in patients with pterygium. Material and Methods Seventy eyes of 70 patients with pterygium were enrolled in the study. The patient group consisted of 36 women and 34 men with an age range between 21 to 75 (Mean 46.06∫13.21). Seventy eyes of 70 age matched patients with refractive problems and without any other ophthalmologic disorder constituted the control group. There were 34 women and 36 men in this group, with an age range between 23 to 73 (Mean 48.11∫10.12). There was no significant difference between the groups with regard to age (p±0.05) or sex (p±0.05). With slit lamp examination, patients with blepharitis and allergic conjuncti- vitis with significant papillary hypertrophy were excluded. During the initial examination, Schirmer’s test 1 was performed first, then marginal tear strip was assessed at least 15 minutes later, and tear film break-up time was estimated. Samples for the mucus fern test were taken on a separate day. Schirmer’s Test 1 Standard Schirmer tear test filter strip (Clement Clarke International) was inserted in the lateral lower fornix of the eye taking care not to touch the cornea. Topical anesthetics were not applied. The patient was instructed to keep the eyes open and to blink as necessary. After 5 minutes, the filter strip was removed and the amount of wetting from the fold was measured (Clinch et al. 1983). Marginal Tear Strip One drop of 1% sodium fluorescein was instilled to the lower fornix. The patient was asked to blink several times to distribute the fluorescein evenly. The eye was then examined using a slit lamp with a cobalt blue filter, and the meniscus formed by the tears at the lower lid margin was observed. This marginal tear strip was then designated as intact, not intact temporally, or not intact (Taylor & Louis 1980). Tear film break-up time (BUT) After the assessment of the marginal tear strip, tear film break-up time was meas- Table 1. Mean Schirmer’s test 1 results and tear film break-up time in pterygium and control groups. Tear function tests Eyes with pterygium Controls Schirmer-1 (mm/5 min) BUT (sec) 17.10∫1.12 9.84∫0.40 19.86∫1.01 13.41∫0.58 Table 2. Distribution of Schirmer’s test 1 and tear film break-up time (BUT) values, mucus fern patterns and marginal tear strip continuity in pterygium vs. control groups and statistical results. Pterygium Test Number of eyes Controls % Number of eyes % Statistical result* Schirmer’s test-1 (mm/5 min) 0–4 5 5–9 5 10–14 15 15–19 24 Ø20 21 7.1 7.1 21.4 34.3 30 2 4 13 18 33 2.9 5.7 18.6 25.7 47.1 p±0.05 p±0.05 p±0.05 p±0.05 p±0.05 BUT (sec) 0–4 5–9 10–14 Ø15 2 34 25 9 2.9 48.6 35.7 12.9 3 18 14 35 4.3 25.7 20 50 p±0.05 p∞0.05 p±0.05 p∞0.05 Mucus Fern Pattern (Type) I 17 II 24 III 25 IV 4 24.3 34.3 35.7 5.7 36 25 7 2 51.4 35.7 10 2.9 p∞0.05 p±0.05 p∞0.05 p±0.05 Marginal Tear Strip Intact Not intact temporally Not intact 42.9 47.1 10 45 21 4 64.3 30 5.7 p∞0.05 p∞0.05 p±0.05 30 33 7 eyes (51.5%) with pterygium and in 21 (30%) control eyes. The difference was statistically significant (p∞0.01). In mucus fern test, type III and type IV crystallization patterns which signify abnormality of the tear film were observed in 41.4% of the eyes with pterygium and in 12.9% of the eyes in the control group (Table 2). There was a statistically significant difference (p∞0.01). Marginal tear film was intact in 42.9% of the eyes with pterygium and in 64.3% of the control eyes (Table 2). The difference was significant statistically (p∞0.05). Discussion *p∞0.05: Statistically significant, p±0.05: Not significant statistically. ured. The patient was asked to stare directly ahead without blinking; the eyelids were not held. The time interval between the last blink and the development of the first randomly distributed dry spot on the cornea was measured with a stop-watch. This test was repeated 3 times and the average was taken (Taylor & Louis 1980). Eyes with a dry spot consistently localized in the same corneal area indicating significant surface abnormality were excluded from the study. Mucus Fern Test 2–3 microliters of tear were collected with a capillary tube from the lower fornix without anesthesia, with care taken not to grasp on the conjunctival surface. The sample was allowed to dry on a light microscopy slide. The crystallization pattern was observed under light microscopy (160¿ and 400¿). Mucus crystallization patterns were classified into four groups (Rolando 1984; Rolando et al. 1988): Type I: Uniform and closely branching arborization. Type II: Single ferns are smaller and less branching is present. Type III: Small ferns with almost no branches; many empty spaces. Type IV: Ferning is absent and clusters of mucus can be present. Results were statistically evaluated using t-test, chi-square test and Mc Nemar test. Results Schirmer’s test 1 values were as low as 3 mm and as high as 50 mm with a mean of 17.10∫1.12 mm in the pterygium group. In the control group the mean was 19.86∫1.01 mm with a range of 4–50 mm (Table 1). The difference between the groups was not significant (tΩ1.71, p±0.05). Schirmer’s test 1 values were less than 10 mm in 10 eyes (14.2%) with pterygium and in 6 (9.6%) control eyes. The difference was not significant (p±0.05). The distribution of Schirmer’s test 1 values and statistical evaluation are shown in Table 2. BUT values were between 3 to 19 seconds with a mean of 9.84∫0.40 sec. in patients with pterygium and between 4 to 25 seconds with a mean of 13.41∫0.58 sec. in the control group (Table 1). There was a statistically significant difference between the groups (tΩ5.31, p∞0.05). The distribution of BUT values according to the groups with the statistical analysis is presented in Table 2. BUT of less than 10 seconds was observed in 36 The most popular theory in the pathogenesis of pterygium is UV insolation (Hill & Maske 1989; Taylor et al. 1989, 1992; Adamis et al. 1990; Mackenzie et al. 1992; Coroneo 1993; Kwok & Coroneo 1994) and differentiation of the limbal stem cells as a result (Kwok & Coroneo 1994). It has been hypothesized that, in susceptible individuals actinic damage causes an alteration in the cornea; the damaged tissue is then recognized as foreign and hypersensitivity reactions are mounted resulting in chronic inflammation. At the beginning a focal conjunctivitis develops at the corneoscleral limbus which later develops into a pterygium (Hill & Maske 1989). In this inflammatory process a variety of cells, soluble mediators, and complex regulatory pathways contribute to abnormal blood vessel formation (Sunderkotter et al. 1991). Early unknown factors from precursor cells to current specific cytokines like Interleukin-8 have been reported to be angiogenic (BenEzra et al. 1990). Recently, it has also been shown that inflammation induces angiogenic peptide vascular endothelial growth factor (VEGF) mRNA and protein to high levels in corneal epithelium, keratocytes and inflammatory cells (Amano et al. 1997). Though UV light and environmental factors play a significant role, the development of pterygium only in some people, not in all, living under the same conditions suggests the role of other factors in the pathogenesis. Tear function abnormalities have been proposed as an etiologic factor due to the observation that a pterygium is further exacerbated by elevation of pterygium head, dryness and dellen formation (Coroneo 1993). No abnormalities in Schirmer’s test, tear 177 Fig. 1. Mucus fern patterns. Upper left, Type I (400¿); Upper right, Type II (400¿); Lower left, Type III (400¿); Lower right, Type IV (400¿). break-up time or rose bengal staining of the cornea were found in eyes with pterygia (Biedner et al. 1979; Taylor 1980; Jensen 1982). It has been suggested that drying of the tear film by wind, devitalized tissues of the medial third of the palpebral aperture and this allowed actinic radiation damage to the conjunctival and corneal epithelium and Bowman’s membrane (Coroneo 1993). To evaluate functions of the tear film, we employed a combination of Schirmer’s test 1, BUT and mucus fern test. We considered values less than 10 mm/5 minutes for Schirmer’s test 1, shorter than 10 seconds for BUT, and type III–type IV patterns for mucus fern test, abnormal (Lemp 1973; Shapiro & Merin 1979; Rolando 1984; Nelson 1994). There was no significant difference in Schirmer’s test 1, which is important in evaluation of the aqueous phase of the tear film. BUT was significantly shorter in the eyes with pterygia. Taylor has reported BUT measurements shorter than 10 seconds in 6 of 26 eyes with pterygia, however, when compared to the control group this was not statistically significant (Taylor 1980). Our groups differed with regard to the mucus fern test and marginal tear strip continuity. Taylor also stated significant discontinuity of the marginal tear strip in the eyes with ptery- 178 gia (Taylor 1980). In our study, in the eyes with pterygia, strong correlation between BUT and mucus fern test, and between BUT and marginal tear strip continuity were found with McNemar test. Tear film stability is ensured by compositional factors like lipid, aqueous, mucus layers and hydrodynamic factors like corneal sensitivity and mechanical factors via eyelid blinking (Tseng 1994). In cases with pterygium, normal lid movement may be compromised and this may lead to secondary changes in the desiccated epithelium, resulting in less wettable areas in BUT. In this study, cases with dry spots consistently developing at one location have been excluded in order to reduce the effect of this hydrodynamic factor on tear film stability. BUT and mucus fern test are used to detect mucus deficiency clinically (Tabbara & Okumoto 1982). Mucin glycoproteins are the major macromolecular components of the mucus. Mucin plays an important role in decreasing the surface tension of tears and increasing the wettability of the hydrophobic lipoprotein epithelial surface (Lemp et al. 1971). It was believed that the precorneal mucus layer is derived from goblet cells – goblet cell-secreted mucin (GCM) –, however, recent studies have suggested that there are at least two types of ocular mucins and that the tear film predominantly consists of a unique type of mucosal epithelium-associated mucin (MEM) that can exist in membraneous and secreted forms (Chang & Tseng 1992). These findings have led to a new concept that nongoblet epithelial cells of cornea and conjunctiva play an active role in maintaining the tear film stability. It is likely that MEM expressed by nongoblet epithelial cells can interact with GCM secreted by conjunctival goblet cells and, through this mucin interaction, the interfacial tension between tear fluid and epithelial cell membrane is lowered and tear film is thus stabilized. So, in addition to compositional and hydrodynamic factors, tear film stability is also controlled by the ocular surface epithelia (Tseng 1994). Recently it has been shown that human conjunctival epithelium expresses human mucin genes MUC1 and MUC4, goblet cells MUC5 and corneal epithelium MUC1 (Inatomi et al. 1995, 1996; Gipson & Inatomi 1997). In conclusion, our study revealed significant abnormalities in BUT, mucus fern test and marginal tear strip in the eyes with pterygia. The altered mucus pattern is likely to act as a primary change inducing pterygium formation or reflecting an existing pathology in the cells lining the ocular surface. Hence, as we do not know whether BUT was lower before the development of pterygium,unraveling the mucin genes in patients with pterygia may help to find out the main factor causing the tear film instability. References Adamis AP, Starck T & Kenyon KR (1990): The management of pterygium. Ophthalmol Clin North America 3: 611–623. Amano S, Kuroki M & Adamis AP (1997): Requirement for vascular endothelial growth factor in wound-related corneal neovascularization. Invest Ophthalmol Vis Sci 38: 701. Biedner B, Biger Y, Rothkoff L & Sachs U (1979): Pterygium and basic tear secretion. Ann Ophthalmol 11: 1235–1236. BenEzra D, Hemo I & Maftzir G (1990): In vivo angiogenic activity of interleukins. Arch Ophthalmol 108: 573. Chang HA & Tseng SCG (1992): Characterization of precorneal mucus layer. Invest Ophthalmol Vis Sci 33(S): 951. Clinch TE, Benedetto DA, Felberg NT & Laibson PR (1983): Schirmer’s Test: A closer look. Arch Ophthalmol 101: 1383–1386. Coroneo MT (1993): Pterygium as an early indicator of ultraviolet insolation: A hypothesis. Br J Ophthalmol 77: 734–739. Detels R & Dhir SP (1967): Pterygium: A geographical study. Arch Ophthalmol 78: 485– 491. Gipson IK & Inatomi T (1997): A major conjunctival goblet cell mucin in the human, mouse and rat is the gel-forming mucin MUC5AC. Invest Ophthalmol Vis Sci 38: 465. Hill JC & Maske R (1989): Pathogenesis of pterygium. Eye 3: 218–226. Inatomi T, Spurr-Michaud S, Tisdale AS & Gipson IK (1995): Human corneal and conjunctival epithelia express MUC1 mucin. Invest Ophthalmol Vis Sci 36: 1818–1827. Inatomi T, Spurr-Michaud S, Tisdale AS, Zhan Q, Feldman ST & Gipson IK (1996): Expression of secretory mucin genes by human conjunctival epithelia. Invest Ophthalmol Vis Sci 37: 1684–1692. Jaros PA & DeLouise VP (1988): Pingueculae and pterygia. Surv Ophthalmol 32: 41–49. Jensen OL (1982): Pterygium, the dominant eye and the habit of closing one eye in the sunlight. Acta Ophthalmol (Copenh) 60: 568–574. Kwok LS & Coroneo MT (1994): A model for pterygium formation. Cornea 13: 219–224. Lemp MA, Dohlman CH & Kuwabara T (1971): Dry eye secondary to mucus deficiency. Trans Am Acad Ophthalmol Otolaryngol 75: 1223–1227. Lemp MA & Hamill JR (1973): Factors affecting tear film break-up in normal eyes. Arch Ophthalmol 89: 103–105. Mackenzie FD, Hirst LW, Battistutta D & Green A (1992): Risk analysis in the development of pterygia. Ophthalmology 99: 1056–1061. Nelson JD (1994): Diagnosis of keratoconjunctivitis sicca. Int Ophthalmol Clin 34: 37–55. Rolando M (1984): Tear mucus ferning test in normal and keratoconjunctivitis sicca eyes Chibret Int J Ophthalmol 2: 32–41. Rolando M, Baldi F & Calabria G (1988): Tear mucus crystallization in children with cystic fibrosis. Ophthalmologica 197: 202–206. Shapiro A & Merin S (1979): Schirmer test and break-up time of tear film in normal subjects. Am J Ophthalmol 88: 752–757. Sunderkotter C, Beil W, Roth J & Sorg C (1991): Cellular events associated with inflammatory angiogenesis in the mouse cornea. Am J Pathol 138: 931–939. Tabbara KF & Okumoto M (1982): Ocular ferning test: A qualitative test for mucus deficiency. Ophthalmology 89: 712–714. Taylor HR (1980): Studies in tear film in climatic droplet keratopathy and pterygium. Arch Ophthalmol 98: 86–88. Taylor HR & Louis WJ (1980): Significance of tear function test abnormalities. Ann Ophthalmol 12: 531–551. Taylor HR, West SK, Munoz B, Rosenthal FS, Bressler SB & Bressler NM (1992): The long-term effects of visible light on the eye. Arch Ophthalmol 110: 99–104. Taylor HR, West SK, Rosenthal FS, Munoz B, Newland HS & Emmett EA (1989): Corneal changes associated with chronic UV irradiation. Arch Ophthalmol 107: 1481– 1484. Tseng SCG (1994): Evaluation of the ocular surface in dry-eye conditions. Int Ophthalmol Clin 34: 57–69. Received on April 29th, 1997 Accepted on September 3rd, 1997 Corresponding author: Sibel Çalıskan Kadayifçilar*, M.D. 6. Sokak 22/4 06500 Bahçelievler Ankara, Turkey Tel: 90 312 213 82 79 Fax: 90 312 223 73 33 *Currently affiliated with Department of Ophthalmology, Baskert University, Ankara, Turkey 179