Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
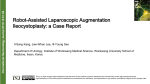
Umbilical metastasis after laparoscopic cholecystectomy: Case Report M.ANAJJAR.𝟏 ,S.BENAMMI.𝟐 , M-S. BELHAMIDI.𝟏 ,M.BOUZROUD.𝟏 , M.ESSARGHINI.𝟏 , B.AITIDIR.𝟏 , M. TARCHOULI.𝟏 , S-M. BOUCHENTOUF.𝟏 , A. AIT AL.𝟏 I, A. BOUNAIM .𝟏 Department of Visceral Surgery I, Military Hospital Mohammed V- Rabat 𝟏, Pediatric Anesthesiology-Reanimation, Pediatric Hospital .𝟐 CONGRES NATIONAL DE CHIRURGIE MARRAKECH 2017 Introduction • Late trocar-site neoplastic dissemination following a laparoscopic cholecystectomy of a primary gallbladder unexpectedly diagnosed is a serious complication associated with a severe prognosis. Rare cases have been described in the literature since the breakthrough of laparoscopy . • The aim is to report a case of neoplastic diffusion after laparoscopic cholecystectomy CONGRES NATIONAL DE CHIRURGIE MARRAKECH 2017 Material and Methods • We report the case of a 66-year-old man who underwent laparoscopic cholecystectomy for chronic lithiasic cholecystitis with 4 trocar site, 2 years form the observation . Histological examination revealed a well-differentiated vesicular • adenocarcinoma infiltrating the vesicular wall arriving to the perimuscular cellular tissue. Corresponding to the PT2 stage of the TNM classification. However the patient refused the surgical resumption. umbilical region with inflammatory signs (Fig. 1). Palpation revealed a hard mass with 7 cm of major axis centered by an inflamed and squamous umbilicus. from the umbilical lesion and carrying the round ligament was performed (Fig 3). There was no invasion of the vesicular bed nor detectable hepatic lesions nor peritoneal metastases. A cutaneous biopsy of the lesion was performed, showing a skin invasion • The histological study revealed an by a slightly differentiated and umbilical localization of a moderately infiltrating adenocarcinoma. differentiated adenocarcinoma and Abdominal CT showed secondary all peri-operative sections were lesion in the peri-umbilical lesions free. The patient did not abdominal wall , with a normal receive adjuvant chemotherapy. The hepatic parenchyma and vesicular patient died four months later due to bed (Fig. 2). diffuse parietal carcinoma. • The patient returned after two years reporting abdominal pain in the • A parietal resection passing 5 cm Figure 1. Umbilical lesion Figure 2. Abdominal CT Figure 3. Operative sight CONGRES NATIONAL DE CHIRURGIE MARRAKECH 2017 Results • Gallbladder cancer is a rare cancer but with a sever prognosis. It is often fortuitously discovered during or after cholecystectomy. Its incidence is estimated at 1 to 2% worldwide. Preoperative diagnosis is made in less than 10% of cases. The seeding of tumor cells on trocar pathways following laparoscopic cholecystectomy is a serious complication of vesicular cancer fortuitously discovered. And this complication have been reported a few times in the literature since the advent of laparoscopy . Most of these metastases are seen in patients with advanced vesicular cancer but may also be reported after surgery for T1 or T2 stages • The orifice used for the extraction of the gall bladder is the most metastatic implantation site encountered. The survival of patients with this complication is weak, estimated at 18.5% after 2 years. The risk of occurrence of such a complication is higher after laparoscopic cholecystectomy than after open cholecystectomy. Moreover, laparoscopic surgery is baned in patients with preoperatively diagnosed gallbladder tumors. In addition, conversion to open surgery is necessary in the case of perioperative suspicion of gallbladder tumors. The development of neoplastic implantation on the trocar path, sometimes for very early stages, initially led to baning laparoscopic approach for any type of cancer. It is often a diffuse peritoneal involvement. Whereas thephysiopathology of the neoplastic dissemination on trocar pathways is yet undimmed, it is speculated that it is multi-factorial : pneumoperitoneum with carbon dioxide, intraabdominal high pressure, laparoscopic instruments, intraoperative vesicular manipulation and effraction, implantation of cancer cells during gallbladder extraction And immunosuppression. Despite the lack of a proven impact on survival, there is no consensus on the need for resection of trocar trajectories. CONGRES NATIONAL DE CHIRURGIE MARRAKECH 2017 Conclusions Although laparoscopic cholecystectomy is widely used in the treatment of vesicular lithiasis, it may be a provider of neoplastic dissemination on trocar orifices following unrecognized vesicular cancer. Despite the lack of scientific evidence of their effectiveness, preventive surgical rules remain consensual: Avoid any effraction And to minimize vesicular manipulations, systematic use of an extraction bag and conversion to laparotomy in the case of suspected cancer References 1-Disseminated bony metastases following incidental gallbladder cancer detected after laparoscopic cholecystectomy .F Youssef, Aw Khan, and Br Davidson, Prof 2-Late Development of Umbilical Metastasis After Laparoscopic Cholecystectomy for a Gallbladder Carcinoma HM Jeon et al. Oncol Rep 6 (2), 283-287. Mar-Apr 1999. 3-Umbilical port metastasis from gallbladder carcinoma after laparoscopic cholecystectomyin European Journal of Surgical Oncology 23(2):1867 · May 1997 4-Gallbladder carcinoma late metastases and incisional hernia at umbilical port site after laparoscopic cholecystectomy A. CIULLA, G. ROMEO, G. GENOVA, G. TOMASELLO, G. AGNELLO, G. CASTRONOVOG Chir Vol. 27 - n. 5 - pp. 214-216 Maggio 2006 CONGRES NATIONAL DE CHIRURGIE CONGRES NATIONAL DE CHIRURGIE MARRAKECH 2017