Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
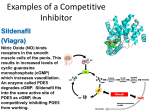
Impotence Drugs and Obstructive Sleep Apnea By Regina Patrick, RPSGT Three drugs commonly used to treat impotence are sildenafil (trade name, Viagra), vardenafil (Levitra), and tadalafil (Cialis). These drugs inhibit the actions of the enzyme phosphodiesterase-5 (PDE-5), resulting in vasodilation and increased bloodflow in penile tissues and therefore an erection. Men with impotence often have obstructive sleep apnea (OSA), a disorder in which a person stops breathing intermittently during sleep due to obstruction of the upper airway. OSA may contribute to erectile dysfunction, but scientists are not sure how. As PDE-5 inhibitor drug use increases, some scientists are beginning to find that the medications that successfully treat impotence may also worsen OSA. This shifted scientific focus on using UK-92,480 to treat impotence. In 1996 Pfizer patented sildenafil, and on March 27, 1998, sildenafil became the first PDE-5 inhibitor drug approved by the U.S. Food and Drug Administration (FDA) for the treatment of impotence.5 PDE-5 & OSA Inhibiting PDE-5 – while great for counteracting a major cause of impotence (e.g., insufficient blood flow in penile tissues) – has unintended consequences in other tissues where it is found. REGINA PATRICK, For example, blocking PDE-5 in the respiratory RPSGT tract reduces the tone of respiratory muscles and impairs immunological processes in the airways. These factors can contribute to a worsening of OSA. In OSA the upper airway collapses inwardly intermittently Background during sleep. Scientists are not fully sure why OSA occurs. The nucleotide molecule cyclic guanosine One thought is that the upper airway muscle tone in some monophosphate (cGMP) relaxes smooth muscle tissues. people with OSA is lower than normal.6 During sleep, upper The enzyme PDE-5 degrades cGMP into guanosine monophosphate (GMP). Once cGMP is degraded into GMP, airway muscle tone further decreases. As a result, structures the relaxing effect no longer occurs. such as tonsils and adenoids that are supported by the Currently, scientists know of 11 classes of PDE enzymes muscles are easily drawn inward during inspirations to the that are labelled PDE-1 through PDE-11. PDE-5 is found in point that the structures can completely collapse into the blood platelets (thereby playing a role in immunity), the upper airway and block airflow. This then results in apnea lungs, and vascular smooth muscle. Its role in vascular (cessation of breathing). smooth muscle tone has been of particular interest in Some scientists suspect that an increase in cGMP due to research studies. PDE-5 inhibition may exacerbate relaxation of upper airway muscles.6 For a person with OSA, this may mean an even greater collapsibility of the upper airway and therefore PDE Inhibitor Drugs increased episodes of apnea during sleep. In the 1980s, scientists were working to develop PDE inhibitor drugs with the hope that such substances would prevent the degradation of cGMP, thereby allowing it to exert PDE-5 & Nitric Oxide its vasodilating effect for a longer period of time. This would Adding credence to this suspicion, a 1996 in vitro study allow the prospective drug to be used to treat high blood led by Ingolf Gath found that inhibiting PDE-5 resulted in pressure and angina (thoracic pain resulting from insufficient relaxation of diaphragm tissue samples from guinea pigs.7 blood flow to the heart). Initially, scientists focused on a The Gath study focused on the molecule nitric oxide (NO), molecule M&B 22,948 – now called zaprinast – which since which plays a role in the synthesis of cGMP. The process the 1970s had been investigated for its ability to reduce begins with nitric oxide synthase II (NOS II), an enzyme allergic reactions.1 By the 1980s, zaprinast had demonstrated that synthesizes NO. Once NO is formed, it interacts with another enzyme, guanylate cyclase, to synthesize cGMP. an ability to lower blood pressure in anesthetized dogs2 and Gath found that when the diaphragm tissue was bathed dilate blood vessels in in vitro studies.3,4 It also was found in the NOS II inhibitor L-NNA (NGnitro L-arginine) and then to inhibit several classes of PDE enzymes, giving it a weak electrically stimulated to induce contractions, the strength vasodilating effect.2 Nevertheless, scientists worked to alter of contraction was stronger than when the tissue was bathed zaprinast’s chemical structure (which is very similar to cGMP) in SNAP (S-nitroso-N-acetyl-D,L-penicillamine), a substance in order to create a compound that would be more selective that releases an NO molecule in chemical reactions. for the PDE-5 class of enzymes and therefore have a stronger Inhibiting the actions of NOS II reduces the amount of NO, vasodilating effect. which in effect lowers the production of cGMP. With less In 1994 scientists at Pfizer laboratories in England had cGMP available, the muscle sample could be contracted more success with a compound named UK-92,480 (now known easily. Increasing the amount of NO resulted in increased as sildenafil). Despite its greater selectivity for PDE-5 and a cGMP production. With increased amounts of cGMP, the stronger vasodilator effect than zaprinast, clinical studies muscle sample relaxed and was more difficult to contract. proved it was ineffective as a treatment for high blood Modulating NO synthesis indirectly demonstrated that cGMP pressure or angina. However, during clinical studies subjects can impact respiratory muscle tone. had frequently reported improved erections as a side effect. 18 A2Zzz 2008 • volume 17 • number 2 PSG Results With this in mind, a 2006 Brazilian study headed by Suely Roizenblatt investigated the effect of the drug sildenafil on sleep and respiration in men with severe OSA.6 This study was the first to demonstrate that sildenafil can aggravate breathing problems in patients who have severe OSA. The study involved 14 subjects who did not have hypertension, respiratory disease, cardiac disease, or pulmonary hypertension (i.e., high pressure within the pulmonary arteries). They were studied for three nights with the first night being the baseline polysomnography (PSG) night. On the second PSG night, the subjects selected one of two envelopes – one containing a sildenafil pill or the other containing a placebo pill. (The subject was blind as to which envelope contained the actual drug.) On the third PSG night one week later, the subject took the pill contained in the second envelope. The researchers found that on the night the subject took the actual drug there was: 1) a significant increase in the desaturation index (18 desaturation events/hour on both baseline and placebo night vs. 30 events/hour on sildenafil night); 2) a significant increase in the average duration of a desaturation event from 8 seconds on baseline and placebo night to 10 seconds on sildenafil night; and 3) an increase in the apnea-hypopnea index (AHI) from 32 respiratory events/hour on both baseline and placebo night to 48 events/hour on the sildenafil night. Roizenblatt and colleagues concluded that the PDE-5 inhibitor drug sildenafil could worsen OSA, and they suggest that the drug may do this by prolonging the effects of NO in airway tissues. However, they are unwilling to say that all PDE-5 inhibitor drugs worsen OSA. Nasal congestion is a common side effect of PDE-5 inhibitor use that may contribute to a worsening of OSA. Various researchers have found that when cGMP levels rise due to PDE-5 inhibition, the excess cGMP triggers NO levels to rise.6,8,9 The excessive NO level causes an overproduction of eosinophils and mast cells in the airway. Inflammation, swelling, and congestion result. These three factors in the nasal passages can restrict airflow, which in turn may contribute to the collapsibility of the upper airway and worsen OSA. Conclusions Although the Roizenblatt study indicates that PDE-5 inhibitors worsen OSA, significantly more research is needed to more clearly understand how PDE-5 inhibitor drugs impact sleep-disordered breathing. The results of the Roizenblatt study present these possible areas of investigation for future research: 1) determining whether there is a link between the severity of OSA and the risk of upper airway collapse with PDE-5 inhibitor use; 2) determining whether PDE-5 inhibitors impact gas exchange in the lungs; 3) determining whether PDE-5 inhibitor use can blunt one’s response to airway obstruction; and 4) determining to what extent PDE-5 inhibitor drugs other than sildenafil can worsen sleep-disordered breathing. It has been estimated that 80% of men with OSA have erectile difficulties.10 PDE-5 inhibitor drug therapy for erectile difficulties may potentially set the stage for continued erectile problems by worsening OSA. For this reason, sildenafil and possibly other PDE-5 inhibitor drugs may need to be used with caution in men with OSA. References 1. Burka JF, Eyre P. Modulation of the formation and release of bovine SRS-A in vitro by several antianaphylactic drugs. Int Arch Allergy Appl Immunol 1975;49(6):774–781. 2. Kling J. Viagra was discovered using a rational drug design approach. Mod Drug Discov 1998;1(2):31-38. Available at: http://pubs.acs.org/hotartcl/mdd/98/ novdec/disc.html. Accessed March 10, 2008. 3. Shibata T, Ogawa K, Ito T et al. Role of cyclic GMP of canine vascular smooth muscle in relaxation by organic nitrates. Jpn Circ Journ 1986;50(11):1091–1099. 4. Nakagawa H, Okumura K, Hashimoto H et al. Effects of atrial natriuretic polypeptide and organic nitrates on levels of relaxation and cyclic nucleotide of canine coronary artery with and without endothelial injury. Heart Vessels 1988;4(1):19–25. 5. U.S. Department of Health and Human Services. Food and Drug Administration. FDA Talk Paper. FDA approves impotence pill, Viagra. March 27, 1998. Available at: http://www.fda.gov/bbs/topics/ ANSWERS/ANS00857.html. Accessed March 18, 2008. 6. Roizenblatt S, Guilleminault C, Poyares D et al. A double-blind, placebo-controlled, crossover study of sildenafil in obstructive sleep apnea. Arch Intern Med 2006;166:1763–1767. 7. Gath I, Closs EI, Godtelarmbrust U et al. Inducible NO synthase II and neuronal NO synthase I are constitutively expressed in different structures of guinea pig skeletal muscle: implications for contractile function. FASEB J 1996;10:1614–1620. 8. Toward TJ, Smith N, Broadley KJ. Effect of phosphodiesterase-5 inhibitor, sildenafil (Viagra), in animal models of airways disease. Am J Respir Crit Care Med 2004;169:227–234. 9. Kiroglu AF, Bayrakli H, Yuca K. Nasal obstruction as a common side-effect of sildenafil citrate. Tohoku J Exp Med 2006;208(3):251–254. 10. Teloken PE, Smith EB, Lowdosky C et al. Defining association between sleep apnea syndrome and erectile dysfunction. Urology 2006;67(5):1033–1037. Regina Patrick, RPSGT, has been in the sleep field for 22 years, and she currently works as a sleep technologist at St. Vincent Mercy Sleep Disorders Center in Toledo, Ohio. A2Zzz 2008 • volume 17 • number 2 19