Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Social immunity wikipedia , lookup
Germ theory of disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Innate immune system wikipedia , lookup
Common cold wikipedia , lookup
Globalization and disease wikipedia , lookup
Urinary tract infection wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Henipavirus wikipedia , lookup
Onchocerciasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Hepatitis C wikipedia , lookup
Gastroenteritis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
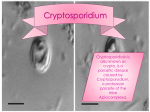
INVITED ARTICLE FOOD SAFETY David Acheson, Section Editor Cryptosporidium Species: New Insights and Old Challenges Brett A. Leav, Melanie Mackay, and Honorine D. Ward Division of Geographic Medicine and Infectious Diseases, Tufts–New England Medical Center, Boston, Massachusetts Cryptosporidium species are protozoan parasites that cause mainly enteric illnesses in humans and other animals. The mode of transmission is most commonly waterborne, but other sources of infection, including foodborne and person-to-person spread, have been documented. The environmental form of the parasite is resistant to most water purification methods, including chlorination. Cryptosporidium infection usually causes a self-limited diarrheal illness but can be life-threatening in immunocompromised individuals. There is no effective therapy for cryptosporidiosis. Cryptosporidium species are intracellular gastrointestinal parasites that were initially thought to cause disease only in animals [1]. The first case of cryptosporidiosis in a human was described in 1976 in a 3.5-year-old girl who developed self-limited enterocolitis [2]. The disease subsequently achieved widespread notoriety in the medical community during the early years of the AIDS epidemic and later after a massive outbreak in Milwaukee, Wisconsin, in 1993 [3]. The parasite continues to be a major threat to human health for 2 major reasons. First, the current methods of water purification are ineffective for its removal from the public water supply. Second, there is no effective therapy for cryptosporidiosis. Although most cases of cryptosporidiosis in humans are self-limited, the consequences of infection can be devastating in immunocompromised individuals and in children living in underdeveloped countries. Advances in our understanding of Cryptosporidium species have been limited because the organism can be propagated only in live animal hosts. Nevertheless, newer molecular techniques, such as PCR, have provided new insights into the complex epidemiology of this parasite. Received 4 October 2002; accepted 26 November 2002; electronically published 18 March 2003. Financial support: National Institutes of Health (grants AI51581A [to B.A.L.], AI46299 [to H.D.W.], AI45194 [to H.D.W.], and D3TW05571A [to M.M.]), US Department of Agriculture (grant 2000-02247), and American Waterworks Association Research Foundation (grant 2596 [to H.D.W.]). Reprints or correspondence: Dr. Honorine Ward, Div. of Geographic Medicine and Infectious Diseases, Tufts–New England Medical Center, Box 041, 750 Washington St., Boston, MA 02111 ([email protected]). Clinical Infectious Diseases 2003; 36:903–8 2003 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2003/3607-0012$15.00 EPIDEMIOLOGY Cryptosporidium infection is a zoonosis with mainly bovine and human reservoirs. Humans are thought to acquire the parasite by the ingestion of oocysts, which are shed in the stool of infected animals or other humans. In developing countries, cryptosporidiosis is endemic and is one of the most common causes of persistent diarrhea among children. In the developed world, cryptosporidiosis mainly occurs in sporadic outbreaks and epidemics. Immunodeficient people, particularly those with deficiencies in cell-mediated immunity, are especially susceptible to Cryptosporidium infection and experience the mostsevere consequences of this illness. Cryptosporidium infection is an important cause of diarrhea in the developing world [4]. An extensive review of cases of diarrhea demonstrated that the incidence of Cryptosporidium infection among immunocompetent patients from developing countries was 6.1%. Children from underdeveloped countries appear to be at particular risk for Cryptosporidium infection: serological evidence of previous infection was present in ∼50% of children in rural China and nearly all children living in an urban slum in Brazil. In the United States, there have been occasional outbreaks of infection in day care centers, foodborne outbreaks, and outbreaks associated with recreational water (public swimming pools, lakes, and ponds). The majority of reported cases of cryptosporidiosis in humans have been associated with contaminated drinking water; the largest such outbreak occurred in Milwaukee in 1993 [3]. Cryptosporidium infection is probably underdiagnosed as a cause of community-acquired diarrhea in the United States. Approximately 2% of stools tested (presumably for active enFOOD SAFETY • CID 2003:36 (1 April) • 903 teritis) are positive for Cryptosporidium species [5]. Furthermore, antibodies to Cryptosporidium have been detected in ∼30% of children and adults in the United States [6]. Even higher seroprevalence rates have been detected in certain populations, such as dairy farmers [6]. Patients with poorly controlled HIV infection and patients receiving immunosuppressive agents are at particular risk for cryptosporidiosis. Other causes of immunodeficiency, such as solid-organ transplantation or primary immunodeficiencies, x-linked hyper-IgM syndrome, severe combined immunodeficiency, selective IgA deficiency, and possibly IFN-g deficiency, are also thought to increase the risk of infection with Cryptosporidium species [7]. TRANSMISSION The best-documented routes of transmission are waterborne, foodborne, and person-to-person spread. The majority of the documented outbreaks of waterborne infection in the world have been attributed to contaminated drinking water supplies, although contaminated water used for recreational activities has also been implicated [5]. The first reported waterborne outbreak of cryptosporidiosis occurred in 1984 and was attributed to fecal contamination of a public artesian well in Texas. In the spring of 1993, the largest outbreak of waterborne disease of any kind recorded occurred in Milwaukee. More than 400,000 of ∼1,600,000 people in the greater Milwaukee area developed cryptosporidiosis after consuming contaminated drinking water. The onset of illness correlated with an increase in the turbidity of the treated water from Lake Michigan, despite use of water purification methods that were standard at the time [3]. Although the source of contamination remains uncertain, recent genotypic analysis of 4 of the isolates indicates consistency with a human origin [8]. Unfortunately, despite the public attention garnered by this massive outbreak, there have been many subsequent outbreaks of Cryptosporidium infection attributed to contaminated drinking water in the United States and the United Kingdom. This is in part due to increased surveillance, but it also reflects our inability to rid the public water supplies of this troublesome parasite. Concern about the safety of the public water supply has prompted government authorities to issue standards for the detection of Cryptosporidium species. These guidelines have been updated as recently as 2001, and our ability to detect Cryptosporidium species in the public water supply has unquestionably improved [9]. However, although surveillance has improved, there is still no consensus between scientists and public officials about the safe limits of Cryptosporidium species in the water supply. Furthermore, implementation of practical, affordable, and effective methods for the elimination of the parasite from drinking water remains an elusive goal. The current strategy for elimination 904 • CID 2003:36 (1 April) • FOOD SAFETY of Cryptosporidium species from the public water supply involves preventing contamination of water sources, physical removal of the organisms, and chemical or physical disinfection. However, these methods are only capable of reducing the number of oocysts, not eliminating the parasite from the water supply. Therefore, it is imperative that patients at risk for Cryptosporidium infection contact their local public water authorities for advice about the safety of their water supply. More sophisticated approaches, such as filtration, ultraviolet light irradiation, and ozone treatment, have not been widely applied for various reasons, including financial and health-related concerns [10]. Although waterborne routes of transmission have been the most notable, foodborne and person-to-person spread have also been documented. Cryptosporidiosis has been attributed to ingestion of contaminated apple cider, chicken salad, milk, and food prepared by an ill food handler [5, 11, 12]. Cryptosporidium species have also been detected in seawater and have even been found in commercially harvested oysters [5]. Another potential source of infection may be raw vegetables sold in the marketplaces in developing countries [5]. However, in the latter 2 cases, a causative relationship has not been established between environmentally detected Cryptosporidium species and cases of infection in humans. Nevertheless, although waterborne outbreaks of cryptosporidiosis in humans have been documented more frequently, foodborne transmission may be underappreciated. Finally, it should be mentioned that, although cattle are thought to be the most common animal reservoir of Cryptosporidium species, other species of animals, including reptiles, birds, and insects, have been shown to harbor the parasite [5]. It is not clear what role these other animal hosts have in the transmission of Cryptosporidium species. TAXONOMY Cryptosporidium species, like Cyclospora, Isospora, and Toxoplasma species, are members of the phylum Apicomplexa. Cryptosporidium species were initially distinguished by their size, host specificity, and site of infection within the animal. Recently, molecular techniques have been used to establish a genetic basis for these distinctions [13, 14]. There are currently thought to be 10 valid species of Cryptosporidium: Cryptosporidium andersoni, Cryptosporidium baileyi, Cryptosporidium felix, Cryptosporidium meleagridis, Cryptosporidium muris, Cryptosporidium nasorum, Cryptosporidium parvum, Cryptosporidium saurophilum, Cryptosporidium serpentis, and Cryptosporidium wrairi. Cryptosporidium infections have been described in 152 different mammalian species. Although Cryptosporidium organisms are known to be zoonotic pathogens, human-to-human transmission seems be the most common mode of transmission in the United States [5, 11]. Recent efforts to use PCR to amplify specific genetic loci have led to a much better understanding of the biological characteristics and transmission of the parasite. These studies have confirmed that C. parvum, the most common cause of cryptosporidiosis in humans, can be divided into 2 major genotypes. These 2 genotypes, human and bovine, are also referred to as genotype 1 and genotype 2, respectively [13]. With rare exceptions, C. parvum genotype 2 is capable of infecting humans and animals, whereas genotype 1 infects only humans [13]. This classification may be an oversimplification, however, because several recent studies have shown significant genetic polymorphisms between isolates of the same genotype. We and others have shown tremendous heterogeneity among genotype 1 isolates at the Cpgp40/15 (also known as “gp60/45/15”) locus, which encodes surface glycoproteins present on invasive stages of the parasite [15, 16]. Furthermore, these studies suggest that Cryptosporidium organisms may undergo genetic recombination within and between the 2 prototypal genotypes. Recently, Feng et al. [17] provided experimental evidence for genetic recombination after infection of a murine host with 2 different genotype 2 isolates via microsatellite analysis. Although the clinical significance of these genotypes is not completely clear, some patterns are beginning to emerge. Most infections in humans appear to be caused by genotype 1 [5]. However, some studies have shown that genotype 2 infections are more common, particularly during the spring and in sporadic outbreaks in rural agricultural communities [11]. Infections in humans due to genotype 1 isolates have been reported to be associated with increased quantity and duration of oocyst shedding [18, 19]. Finally, it should be noted that other species and genotypes of Cryptosporidium in addition to C. parvum might infect humans. Several recent reports have described the isolation of C. meleagridis, C. felis, and the “dog” genotype from humans [5, 11]. The relative importance of these other species of Cryptosporidium in infections in humans is currently uncertain. Furthermore, because the taxonomy of Cryptosporidium is in a state of flux, the validity of some of the more unusual species may not endure. PATHOGENESIS Infection with Cryptosporidium begins when the ingested oocysts release sporozoites, which subsequently attach to and invade the intestinal epithelial cell. The parasite has a particular predilection for the jejunum and terminal ileum. This point deserves emphasis, because diagnostic evaluations, such as endoscopy, may miss the site of infection. In patients with AIDS, other sites within the gastrointestinal tract may be involved, including the stomach, duodenum, and colon, as well as the biliary tract [7]. The histopathological features of cryptosporidiosis include a minimal inflammatory infiltrate and blunting of the villus. More-pronounced inflammatory changes, such as disruption of the epithelial cell barrier and more-extensive infiltration of the lamina propria with inflammatory cells, are seen in immunodeficient patients [20]. The mechanism by which Cryptosporidium infection causes diarrhea remains elusive. The diarrhea is typically noninflammatory and is often profuse. The parasite does elicit a local inflammatory response, and increased production of prostaglandins and several cytokines, particularly IFN-g, has been described [21]. It is possible that these inflammatory mediators may consequently alter solute transportation in the intestinal epithelial cell, leading to osmotic diarrhea. Cryptosporidium infection has also been shown to inhibit apoptosis in infected epithelial cells as well as promote it in adjacent epithelial cells in vitro [21]. This could theoretically prolong parasite survival and impair absorption in the intestinal mucosa. The presence of an enterotoxin has also been hypothesized but never conclusively demonstrated [21]. Whatever the mechanisms by which Cryptosporidium infection causes disease may be, attachment to and invasion of host cells are crucial primary events in pathogenesis. However, little is known about specific parasite and host molecules involved in these processes. Knowledge of such molecules is essential for understanding the pathogenic mechanisms used by this parasite. Increasing recognition of Cryptosporidium species as emerging pathogens in humans has led to the identification of proteins, including CSL, GP900, p23/27, TRAP C1, gp40/45, cp47, and gp15/Cp17, which are implicated in mediating these interactions [22]. However, progress in establishing the functional role of these proteins has been hindered by the inability to propagate C. parvum in vitro and the lack of suitable systems for genetic manipulation of the parasite. IMMUNE RESPONSE Cell-mediated immunity appears to be the major component of the immune response to Cryptosporidium infection. Although there is a prominent humoral response to infection, the exact role of antibodies in host defense to Cryptosporidium infection is unclear. The correlation between the decreased number of CD4⫹ T cells and the risk of Cryptosporidium infection is evidence of the critical role that immune cells play in immunity [23]. Studies that use murine models in which CD4⫹ T cells were lacking confirmed the central role of these cells in adaptive immunity [23]. The cytokines IFN-g, IL-12, and TNF-a have also been shown to be protective against Cryptosporidium infection in laboratory models [24]. CD4⫹ T cells appear to be the source of IFN-g in the adaptive immune response, and these cells have been shown to limit experimental infection [23]. Innate immune mechanisms may also be important in resistance to Cryptosporidium infection, because mice FOOD SAFETY • CID 2003:36 (1 April) • 905 Figure 1. Cryptosporidium parvum oocysts in feces visualized by a Kinyoun modified acid-fast stain (A) and immunofluorescence with use of a monoclonal antibody (Cellabs) to the oocyst wall (B). that lack adaptive immune cells are initially resistant to infection. Furthermore, mutations of the mannose-binding lectin gene, a component of the complement cascade, were associated with an increased risk of cryptosporidiosis in patients with AIDS [24]. Therefore, it seems that, although adaptive immunity is necessary for the resolution of cryptosporidiosis, innate immune mechanisms may be important in resistance to infection. CLINICAL MANIFESTATIONS Essentially all humans are susceptible to Cryptosporidium infection, although people with serological evidence of previous infection seem to be more resistant [25]. The parasite is highly infectious, with an ID50 ranging from 9 to 1042 oocysts, depending on the isolate [11]. The presentation is highly variable but is typically characterized by watery diarrhea. The diarrhea is often accompanied by abdominal pain and occasionally systemic symptoms such as fever, malaise, nausea, vomiting, and loss of appetite. The symptoms begin ∼5 days after the ingestion of oocysts but can begin up to 2 weeks later. The duration of illness in immunocompetent hosts is variable, lasting from several days to 5 weeks [26]. It is worth noting that many exposed patients are asymptomatic. In a study of experimental infection in humans, one-third of the subjects who ingested oocysts had no diarrhea [27]. Although the disease is self-limited in most patients, in several other situations, cryptosporidiosis can cause significant morbidity and death. Before the widespread use of HAART, cryptosporidiosis was a relatively common opportunistic infection in patients with advanced HIV infection. The risk of acquiring cryptosporidiosis was correlated with lower numbers of CD4⫹ T cells (⭐200 cells/mm3) [7]. In patients with advanced HIV infection, the illness has a highly variable presentation. In a cohort of HIV-infected patients studied in Baltimore during 1985–1995, four patterns were described: transient infection, intermittent relapsing infection, cholera-like infection, 906 • CID 2003:36 (1 April) • FOOD SAFETY and chronic infection [28]. Another well-described manifestation of Cryptosporidium infection in patients with AIDS is cholangitis, which is seen more often with more-severe immunosuppression, defined as a CD4⫹ T cell count of ⭐50 cells/ mm3. These patients have a poor prognosis and often present without the typical symptoms of abdominal pain [21]. Gastric cryptosporidiosis and pancreatitis have also been described in patients with AIDS. Other causes of immunodeficiency mentioned above have also been associated with these more recalcitrant forms of cryptosporidiosis [7]. Although Cryptosporidium infection does not have a predilection for any particular age group, it is common among children in developed and underdeveloped nations. Several published reports have shown that cryptosporidiosis may have devastating long-term effects in children in poorer countries. In Brazil, cryptosporidiosis and persistent diarrhea among children have been correlated with subsequent impairments in physical fitness and diminished cognitive function [29]. Sadly, it appears that these children with persistent diarrhea are caught in a vicious cycle of malnutrition, placing them at risk for further diarrheal illness, which in turn leads to progressively worse nutritional status [30]. DIAGNOSIS Cryptosporidiosis can be diagnosed via invasive or noninvasive techniques. Intestinal analysis via biopsy with demonstration of intracellular forms of the parasite is specific, but the diagnosis may be missed, because most common sites of infection are less accessible endoscopically. The “gold standard” and perhaps most widely used test for the detection of Cryptosporidium oocysts in stool remains the modified acid-fast or Kinyoun stain (figure 1A). The test should be specifically requested, because it will not be performed as part of a routine examination for ova and parasites. Interpretation of the stained smear requires experience, because other organisms in the stool may stain acid fast. Several immunofluorescent assays (figure 1B) and EIA kits have become commercially available and show promising sensitivity and specificity. These tests use antibodies against Cryptosporidium antigens to detect the parasite in stool specimens. One of these kits, the ColorPAC Cryptosporidium/Giardia rapid assay (Becton-Dickinson), was recently recalled because of a cluster of false-positive results [31]. PCR-based techniques also accurately detect the parasite in environmental samples and stool specimens but have yet to be standardized for routine clinical use and are not yet commercially available. 3. 4. 5. 6. 7. THERAPY 8. There is no effective antimicrobial agent for treatment of cryptosporidiosis in humans, and, consequently, the US Food and Drug Administration has not approved a medication for this purpose. Paromomycin and, recently, nitazoxanide have been reported to have some clinical efficacy. The results of clinical trials of these 2 drugs have been mixed. Azithromycin in combination with paromomycin appeared to have a demonstrable effect in one uncontrolled trial involving patients with AIDS who have cryptosporidiosis. Finally, resolution of cryptosporidiosis has been demonstrated after reconstitution of the immune system when HAART is used to treat advanced HIV infection [21]. PREVENTION Patients with underlying immune system weaknesses are at risk for the more severe complications of Cryptosporidium infection, as mentioned above. In the absence of effective, specific therapy against infection with this parasite, preventative measures are of great importance among this patient population. Such measures include extensive hand washing, avoiding direct contact with stool from animals or humans, avoiding the accidental ingestion of water used in recreational activities, and taking measures to ensure the safety of the drinking water. It should be noted that the quality of the local drinking water is regionally and seasonally variable. Local public health and municipal water authorities can provide specific information about the safety of the water supply. Cryptosporidium species can be removed from drinking water by either boiling for 1 min or by filtering the water through a filter with a pore size of !1 mm. These recommendations are well summarized on the Centers for Disease Control and Prevention’s Web site (http://www.cdc.gov/ncidod/dpd/ parasites/cryptosporidiosis/factsht_crypto_prevent_ci.htm#12). 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. References 1. Tyzzer EE. A sporozoon found in the peptic glands of the common mouse. Proc Soc Exp Biol Med 1907; 5:12–3. 2. Nime FA, Burek JD, Page DL, Holscher MA, Yardley JH. Acute en- 25. terocolitis in a human being infected with the protozoan Cryptosporidium. Gastroenterology 1976; 70:592–8. MacKenzie WR, Schell WL, Blair KA, et al. Massive outbreak of waterborne cryptosporidium infection in Milwaukee, Wisconsin: recurrence of illness and risk of secondary transmission. Clin Infect Dis 1995; 21:57–62. Guerrant RL. Cryptosporidiosis: an emerging, highly infectious threat. Emerg Infect Dis 1997; 3:51–7. Fayer R, Morgan U, Upton SJ. Epidemiology of Cryptosporidium: transmission, detection and identification. Int J Parasitol 2000; 30:1305–22. Griffiths JK. Human cryptosporidiosis: epidemiology, transmission, clinical disease, treatment, and diagnosis. Adv Parasitol 1998; 40:37–85. Hunter PR, Nichols G. Epidemiology and clinical features of Cryptosporidium infection in immunocompromised patients. Clin Microbiol Rev 2002; 15:145–54. Peng MM, Xiao L, Freeman AR, et al. Genetic polymorphism among Cryptosporidium parvum isolates: evidence of two distinct human transmission cycles. Emerg Infect Dis 1997; 3:567–73. Quintero-Betancourt W, Peele ER, Rose JB. Cryptosporidium parvum and Cyclospora cayetanensis: a review of laboratory methods for detection of these waterborne parasites. J Microbiol Methods 2002; 49: 209–24. Rose JB, Huffman DE, Gennaccaro A. Risk and control of waterborne cryptosporidiosis. FEMS Microbiol Rev 2002; 26:113–23. Dillingham R, Lima A, Guerrant R. Cryptosporidiosis: epidemiology and impact. Microbes Infect 2002; 4:1059–66. Quiroz ES, Bern C, MacArthur JR, et al. An outbreak of cryptosporidiosis linked to a foodhandler. J Infect Dis 2000; 181:695–700. Widmer G, Lin L, Kapur V, Feng X, Abrahamsen M. Genomics and genetics of Cryptosporidium parvum: the key to understanding cryptosporidiosis. Microbes Infect 2002; 4:1081–90. Morgan UM, Xiao L, Fayer R, Lal AA, Thompson RC. Variation in Cryptosporidium: towards a taxonomic revision of the genus. Int J Parasitol 1999; 29:1733–51. Strong WB, Gut J, Nelson RG. Cloning and sequence analysis of a highly polymorphic Cryptosporidium parvum gene encoding a 60-kilodalton glycoprotein and characterization of its 15- and 45-kilodalton zoite surface antigen products. Infect Immun 2000; 68:4117–34. Leav BA, Mackay MR, Anyanwu A, et al. Analysis of sequence diversity at the highly polymorphic Cpgp40/15 locus among Cryptosporidium isolates from human immunodeficiency virus–infected children in South Africa. Infect Immun 2002; 70:3881–90. Feng X, Rich SM, Tzipori S, Widmer G. Experimental evidence for genetic recombination in the opportunistic pathogen Cryptosporidium parvum. Mol Biochem Parasitol 2002; 119:55–62. Widmer G, Tzipori S, Fichtenbaum CJ, Griffiths JK. Genotypic and phenotypic characterization of Cryptosporidium parvum isolates from people with AIDS. J Infect Dis 1998; 178:834–40. Xiao L, Bern C, Limor J, et al. Identification of 5 types of Cryptosporidium parasites in children in Lima, Peru. J Infect Dis 2001; 183: 492–7. Lumadue JA, Manabe YC, Moore RD, Belitsos PC, Sears CL, Clark DP. A clinicopathologic analysis of AIDS-related cryptosporidiosis. AIDS 1998; 12:2459–66. Chen XM, Keithly JS, Paya CV, LaRusso NF. Cryptosporidiosis. N Engl J Med 2002; 346:1723–31. Tzipori S, Ward H. Cryptosporidiosis: biology, pathogenesis and disease. Microbes Infect 2002; 4:1047–58. Riggs M. Recent advances in cryptosporidiosis: the immune response. Microbes Infect 2002; 4:1067–80. Lean IS, McDonald V, Pollok RC. The role of cytokines in the pathogenesis of Cryptosporidium infection. Curr Opin Infect Dis 2002; 15: 229–34. Chappell CL, Okhuysen PC, Sterling CR, Wang C, Jakubowski W, Dupont HL. Infectivity of Cryptosporidium parvum in healthy adults with pre-existing anti–C. parvum serum immunoglobulin G. Am J Trop Med Hyg 1999; 60:157–64. FOOD SAFETY • CID 2003:36 (1 April) • 907 26. Jokipii L, Jokipii AM. Timing of symptoms and oocyst excretion in human cryptosporidiosis. N Engl J Med 1986; 315:1643–7. 27. DuPont HL, Chappell CL, Sterling CR, Okhuysen PC, Rose JB, Jakubowski W. The infectivity of Cryptosporidium parvum in healthy volunteers. N Engl J Med 1995; 332:855–9. 28. Manabe YC, Clark DP, Moore RD, et al. Cryptosporidiosis in patients with AIDS: correlates of disease and survival. Clin Infect Dis 1998; 27: 536–42. 29. Guerrant DI, Moore SR, Lima AA, Patrick PD, Schorling JB, Guerrant RL. Association of early childhood diarrhea and cryptosporidiosis with 908 • CID 2003:36 (1 April) • FOOD SAFETY impaired physical fitness and cognitive function 4–7 years later in a poor urban community in northeast Brazil. Am J Trop Med Hyg 1999; 61:707–13. 30. Lima AA, Moore SR, Barboza MS Jr, et al. Persistent diarrhea signals a critical period of increased diarrhea burdens and nutritional shortfalls: a prospective cohort study among children in northeastern Brazil. J Infect Dis 2000; 181:1643–51. 31. Manufacturer’s recall of rapid assay kits based on false positive Cryptosporidium antigen tests—Wisconsin, 2001–2002. MMWR Morb Mortal Wkly Rep 2002; 51:189.