Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Chronic Renal failure
Chronic renal failure (CRF) is the progressive loss of kidney function. The kidneys
attempt to compensate for renal damage by hyperfiltration (excessive straining of
the blood) within the remaining functional nephrons (filtering units that consist of a
glomerulus and corresponding tubule). Over time, hyperfiltration causes further loss
of function.
Chronic loss of function causes generalized wasting (shrinking in size) and
progressive scarring within all parts of the kidneys. In time, overall scarring obscures
the site of the initial damage. Yet, it is not until over 70% of the normal combined
function of both kidneys is lost that most patients begin to experience symptoms of
kidney failure.
Types
Chronic renal failure (CRF) can be classified by the site (location) of primary
damage:
Pre-renal CRF
Post-renal CRF (obstructive uropathy)
Renal CRF
CRF Causes
The cause for CRF sometimes can be determined by a detailed medical history, a
comprehensive physical examination, and laboratory studies. More often than not,
determining the cause of CRF is difficult if not impossible. Even a kidney biopsy may
be inconclusive, because all forms of kidney failure eventually progress to diffuse
scarring and look the same on kidney biopsy. The most common causes for CRF are
diabetes and high blood pressure (hypertension.)
Kidney disorders, including chronic renal failure, are common in patients who have
multiple myeloma (cancer that begins in a type of white blood cell called plasma
cells). Several different factors are related to renal disease associated with multiple
myeloma. Myeloma cells produce large numbers of proteins in the urine (called
proteinuria). These proteins often form deposits in the kidneys (condition called
amyloidosis) and cause kidney failure. In addition, multiple myeloma increases the
risk for hypercalcemia (high levels of calcium in the blood) and anemia (low levels of
red blood cells) and results in high blood levels of uric acid, which also increase the
risk for chronic renal failure.
Pre-Renal CRF
Some medical conditions cause continuous hypoperfusion (low blood flow) of the
kidneys, leading to kidney atrophy (shrinking), loss of nephron function, and chronic
renal failure (CRF). These conditions include poor cardiac function, chronic liver
failure, and atherosclerosis ("hardening") of the renal arteries. Each of these
conditions can induce ischemic nephropathy.
Post-Renal CRF
Interference with the normal flow of urine can produce backpressure within the
kidneys, can damage nephrons, and lead to obstructive uropathy, a disease of the
urinary tract. Abnormalities that may hamper urine flow and cause post-renal CRF
include the following:
Bladder outlet obstruction due to an enlarged prostate gland or bladder
stone
Neurogenic bladder, an overdistended bladder caused by impaired
communicator nerve fibers from the bladder to the spinal cord
Kidney stones in both ureters, the tubes that pass urine from each kidney to
the bladder
Obstruction of the tubules,the end channels of the renal nephrons
Retroperitoneal fibrosis, the formation of fiberlike tissue behind the
peritoneum, the membrane that lines the abdominal cavity
Vesicoureteral reflux (VUR), the backward flow of urine from the bladder
into a ureter
Renal CRF
Chronic renal failure caused by changes within the kidneys, is called renal CRF, and
is broadly categorized as follows:
Diabetic nephropathy, kidney disease associated with diabetes; the most
common cause of CRF
Hypertension nephrosclerosis, a condition that occurs with increased
frequency in African Americans; the second leading cause of CRF
Chronic glomerular nephritis, a condition caused by diseases that affect
the glomeruli and bring about progressive dysfunction
Chronic interstitial nephritis, a condition caused by disorders that
ultimately lead to progressive scarring of the interstitium
Renal vascular CRF, large vessel abnormalities such as renal artery stenosis
(narrowing of the large arteries that supply the kidneys)
CRF Signs and Symptoms
Chronic renal failure (CRF) usually produces symptoms when renal function — which
is measured as the glomerular filtration rate (GFR) — falls below 30 milliliters per
minute (< 30 mL/min). This is approximately 30% of the normal value.
When the glomerular filtration rate (GFR) slows to below 30 mL/min, signs of uremia
(high blood level of protein by-products, such as urea) may become noticeable.
When the GFR falls below 15 mL/min most people become increasingly symptomatic.
Uremic symptoms can affect every organ system, most noticeably the following:
Neurological system–cognitive impairment, personality change, asterixis
(motor disturbance that affects groups of muscles), seizures (rare)
Gastrointestinal system–nausea, vomiting, food distaste (often described
as bland, metallic, "like cardboard")
Blood-forming system–anemia due to erythropoetin deficiency, easy
bruising and bleeding due to abnormal platelets
Pulmonary system–fluid in the lungs, with breathing difficulties
Cardiovascular system –chest pain due to inflammation of the sac
surrounding the heart (pericarditis) and pericardial effusion (fluid
accumulation around the heart)
Skin –generalized itching
CRF Diagnosis
Chronic renal failure (CRF) is diagnosed by the observation of a combination of
symptoms and elevated blood urea nitrogen (BUN) and creatinine (Cr) levels.
The following abnormalities found in the blood may signal CRF:
Anemia (low red blood cell count)
High level of parathyroid hormone
Hypocalcemia (low blood level of calcium)
Hyperphosphatemia (high blood level of phosphate)
Hyperkalemia (high blood level of potassium)
Hyponatremia (low blood level of sodium)
Low blood level of bicarbonate
Low plasma pH (blood acidity)
Whether renal failure is acute or chronic usually can be distinguished by comparing
prior test results (e.g., from the past several months or years). It is difficult to make
the distinction without previous test results.
Ultrasound may show that the kidneys are small in size and echogenic (a sign of
renal scarring), signs that supports a diagnosis of CRF. For unclear reasons patients
with diabetic nephropathy often have preservation of kidney size despite CRF. They
do however, typically have increased echogenicity.
Treatment
Once CRF has been diagnosed, the physician attempts to determine the cause and, if
possible, plan a specific treatment. Nonspecific treatments are implemented to delay
or possibly arrest the progressive loss of kidney function.
Control hypertension (high blood pressure)—Target systolic blood pressure (BP) is
120 to 135 mm Hg; target diastolic BP is 70 to 80 mm Hg. Antihypertensive
medication from the ACE class is preferable because of protective effects on the
kidneys.
Restrict dietary protein—Dietary protein is broken down into amino acids and
absorbed from the stomach into the blood. The amino acids are taken from the
bloodstream and used to build muscle and perform other essential functions. Excess
amino acids are further broken down into carbohydrates and nitrogen-containing
waste that is eliminated by the kidneys. Amino acid disposal further burdens the
kidneys, and is believed to speed the progression of CRF. This process is like forcing
a damaged machine to work harder, causing it to break down sooner than expected.
Affected patients must be cautious not to overdo protein restriction, because it can
lead to malnutrition and muscle wasting. Moderate protein restriction for a CRF
patient is about 0.6 to 0.8 gm/kg/day, which is effectively achieved by following the
advice of a dietician.
Manage pre-end-stage renal disease (pre-ESRD)—Treatment for pre-ESRD
should begin once the glomerular filtration rate (GFR) falls below 30 milliliters per
minute (< 30 mL/min). Pre-ESRD management includes the identification and
treatment of anemia (low red blood cell count). When the GFR drops below 30
mL/min, anemia often develops because the kidneys produce an inadequate amount
of erythropoetin (EPO). This hormone is made by the kidneys and travels to the bone
marrow, where it stimulates red blood cell production. Anemic patients are
candidates for EPO (Procrit®) injections to maintain their hematocrit (volume
percent of red blood cells in whole blood) between 30% and 36%.
Identify and Treat Secondary Hyperparathyroidism—With the loss of kidney
function, phosphate accumulates in the blood. Excess phosphate in the blood reduces
levels of blood calcium, and low blood calcium levels trigger the parathyroid gland
(located in the neck) to release more parathyroid hormone (PTH). PTH then dissolves
bone tissue to release stored calcium and raise the level of calcium in the blood. This
chronic cycle of events is called secondary hyperthyroidism.
The net result of this condition is the development of metabolic bone disease (renal
osteodystrophy). These patients are at risk for bone fractures, bone and muscle
pain, which can sometimes be accompanied by severe itching, and cardiovascular
complications. Severe itching is thought to be in part due to the elevated circulating
PTH level itself.
Patients with secondary hyperthyroidism should limit their intake of foods that are
high in phosphate (e.g., dairy products, colas). Many patients must take medication
with meals that binds the phosphate (phosphate-binders) and prevents it from being
absorbed into the blood and allows it to be excreted in the stool (feces). In general,
calcium based salts (e.g., TUMS, Oscal)have been the phosphate-binders prescribed.
A new organic based phophate-binder called renagel has recently become available
and, although it is more expensive, it has many advantages over the calcium based
phosphate-binders.
Most patients also require a potent vitamin D supplement (e.g., calcitrol, hexitrol),
which helps to suppress excess PTH production. The final metabolic step in the
synthesis of vitamin D occurs normally in the kidney and there is often a deficiency
of this vitamin in these patients.
Cinacalcet hydrochloride (e.g., Sensipar™) may be used alone or in combination with
Vitamin D supplements or phosphate-binders to treat patients with secondary
hyperparathyroidism who are on dialysis. Sensipar tablets should be taken with food
and the dosage varies, depending on calcium and phosphate levels in the blood.
Side effects include nausea, vomiting, and diarrhea.
Preparation for renal replacement therapy (RRT)
Early preparation is important. The health care team educates the patient about the
different procedures involved in RRT, which include the following:
Hemodialysis—removal of toxic elements from the blood, which is filtered
through a membrane while circulated outside of the body
Peritoneal dialysis—filtration through the lining membrane of the abdominal
cavity; fluid is instilled into the peritoneal space, then drained
kidney transplantation
It is important to place an arteriovenous fistula (AVF)—a passage between an artery
and a vein that provides a suitable blood vessel for repeated dialysis—at least 3
months prior to beginning hemodialysis, because an AVF requires 3 months to
mature before it can be used.
The health care team can address the patient's fears and anxieties about treatment
and can clarify the financial, emotional, and social concerns of RRT.
Prognosis
CRF is often insidious in its onset and progression. The rate of progression is variable
but usually renal function steadily declines resulting in end-stage renal disease
(ESRD).
Acute glomerulonephritis
(AGN) is active inflammation in the glomeruli. Each kidney is composed of about 1
million microscopic filtering "screens" known as glomeruli that selectively remove
uremic waste products. The inflammatory process usually begins with an infection or
injury (e.g., burn, trauma), then the protective immune system fights off the
infection, scar tissue forms, and the process is complete.
There are many diseases that cause an active inflammation within the glomeruli.
Some of these diseases are systemic (i.e., other parts of the body are involved at the
same time) and some occur solely in the glomeruli. When there is active
inflammation within the kidney, scar tissue may replace normal, functional kidney
tissue and cause irreversible renal impairment.
The severity and extent of glomerular damage—focal (confined) or diffuse
(widespread)—determines how the disease is manifested. Glomerular damage can
appear as subacute renal failure, progressive chronic renal failure (CRF); or simply a
urinary abnormality such as hematuria (blood in the urine) or proteinuria (excess
protein in the urine).
Causes
In diffuse glomerulonephritis (GN), all of the glomeruli are aggressively attacked,
leading to acute renal failure (ARF). Disorders that attack several organs and cause
diffuse GN are referred to as secondary causes. Secondary causes of diffuse GN
include the following:
Cryoglobulinemia
Goodpasteur’s syndrome (membranous antiglomerular basement membrane
disease)
Lupus nephritis
Schönlein-Henoch purpura
Vasculitis (e.g., Wegener's granulomatosis, periarteritis nodosa)
Primary diseases that solely affect the kidneys and cause AGN, include the following:
Immunoglobulin A nephropathy (IgA nephropathy, Berger’s disease)
Membranoproliferative nephritis (type of kidney inflammation)
Postinfectious GN (GN that results after an infection)
Signs and Symptoms
Patients who have secondary causes of AGN often exhibit these symptoms:
Cough with blood-tinged sputum
Fever
Joint or muscle pain
Rash
Diagnosis
Patients with acute glomerulonephritis (AGN) have an active urinary sediment. This
means that signs of active kidney inflammation can be detected when the urine is
examined under the microscope. Such signs include red blood cells, white blood cells,
proteinuria (blood proteins in the urine), and "casts" of cells that have leaked
through the glomeruli and have reached the tubule, where they develop into
cylindrical forms.A kidney biopsy is essential to establish a diagnosis of AGN,
determine the cause, and create an effective treatment plan.
TreatmentThe
goal of treatment is to stop the ongoing inflammation and lessen the degree of
scarring that ensues. Depending on the diagnosis, there are different treatment
strategies. Often the treatment warrants a regimen of immunosuppressive drugs to
limit the immune system’s activity. This decreases the degree of inflammation and
subsequent irreversible scarring.
Acute Interstitial Nephritis
The interstitium is the tissue that surrounds and imbeds the glomeruli (microscopic
"filtering screens") and tubules (long tubes that connect with each glomerulus and
channel urine) within the kidneys. Acute interstitial nephritis (AIN) is rapidly
developing inflammation that occurs within the interstitium. It can produce a variety
of clinical symptoms, depending upon the severity and extent of kidney involvement.
Causes
Most AIN is caused by an acute allergic reaction to a medication, including antibiotics
and nonsteroidal anti-inflammatory drugs (NSAIDs) such as:
Ibuprofen
Cephatholin
Cimetidine
Cyclosporine
Methicillin
Penicillins
AIN is also linked with certain infections and diseases such as Legionella
pneumophila, collagen vascular diseases (e.g., sarcoidosis), streptococcal infections,
and transplant rejection.
Signs and Symptoms
Indicators of AIN include a recent history of infection or the start of a new
medication. Symptoms often include fever, rash, and generalized aches and pains.
Diagnosis
The definitive diagnosis of AIN requires a kidney biopsy, which reveals inflammation
of the renal interstitium. Urinalysis (analysis of the urine) often reveals eosinophils—
specialized white blood cells that are seen in allergic reactions. Often one can detect
increased eosinophils in the blood in patients with AIN. AIN sometimes is diagnosed
by means of a gallium scan (nuclear medicine imaging method; a radiologist injects
the patient with gallium-67, which will accumulate in areas of infection or malignancy
and can be viewed with a special camera).
Treatment
All medication(s) believed to be responsible for the inflammation must be
discontinued. If there is significant renal impairment, treatment with steroids
typically is required for 2 to 3 months. Stronger immunosuppressive agents may be
needed if there is no response to the steroids. Each case of AIN must be reviewed by
a nephrologist (kidney specialist).
Acute Tubular Necrosis
Each glomerulus (microscopic "filtering screen") has a tubule that transports urine to
the ureters (see anatomy) and metabolically alters the urine and its chemicals.
Because the tubules are exceedingly metabolically active, they are very dependent
on the oxygen that supplies the tubular cells. They are often described as being
nearly oxygen starved because they work so hard. Close to 200 liters of fluid is
filtered across the glomeruli, and the tubules reabsorb 99% (198 liters) of the fluid in
a selective manner.
Acute tubular necrosis (ATN) is the death of tubular cells, which may result when
tubular cells do not get enough oxygen (ischemic ATN) or when they have been
exposed to a toxic drug or molecule (nephrotoxic ATN). Fortunately, new tubular
cells usually replace those that have died. Indeed, the tubular cells of the kidneys
undergo a continuous cycle of cell death and renewal, much like the cells of the skin.
Causes
In the hospital setting, ATN is the most common cause of acute renal failure (ARF).
Hospital patients often have acute medical problems that limit the oxygen supplied to
the tubules or that cause tubular hypoperfusion (decreased blood flow).
Certain medical and surgical situations are associated with a high risk for developing
ischemic ATN:
Hypotension (low blood pressure)
Obstetric (birth-related) complications
Obstructive jaundice (yellow-tinged skin caused by blocked flow of bile
Prolonged prerenal state
Sepsis (infection in the blood or tissues)
Surgery (e.g., open heart surgery, repair of abdominal aortic aneurysm)
Some medications and clinical materials can cause nephrotoxic ATN:
Aminoglycosides (antibacterial antibiotics such as streptomycin and
gentamicin)
Amphotericin B (antibiotic used to treat some forms of meningitis and
systemic fungal infections)
Cisplatin (anticancer agent used to treat late-stage ovarian and testicular
cancers)
Radioisotopic contrast media (agent used in certain imaging studies)
Exposure to certain molecules also may cause nephrotoxic ATN. For example, when a
person suffers significant muscle trauma, such as during a crush injury, the muscle
enzyme creatinine phosphokinase (CPK) leaks into the blood. Myoglobulin is the
protein that leaks into the blood and ultimately causes ATN. Measurement of CPK is a
marker of myoglobulin released by muscle cells. If enough CPK spills into the blood
and is filtered through the glomeruli, it can damage the tubules, causing nephrotoxic
ATN.
Signs and Symptoms
Acute tubular necrosis (ATN) typically does not produce specific signs or symptoms.
Diagnosis
Diagnosis often is supported by a positive history of risk factors. Yet the physician
must rule out other reasons for acute renal failure, such as prerenal, postrenal, and
renal ARF. Distinguishing ATN from prerenal ARF can be extremely difficult. Urine
chemistry and microscopic examination of the urine help to confirm the diagnosis.
ATN does not rapidly improve following the administration of large-volume
intravenous fluid.
Treatment
Management relies on aggressive treatment of the factors that precipitated ATN. One
exception is the treatment of ATN associated with the breakdown of muscle fibers
caused by a crush injury. Aggressive, forced diuresis (i.e., an increased excretion of
urine) may improve the condition.
Patients at high risk for developing ARF from contrast induced ATN should be treated
with intravenous (IV) fluids prior to contrast exposure to prevent the ATN. There has
been a recent report suggesting that pretreatment of these patients with a
medication called mucomyst may also help to prevent ARF in patients undergoing IV
contrast exposure.
Prognosis
Because tubular cells have the capacity to replace themselves, the overall prognosis
for ATN is quite good if the cause is corrected. Once the precipitating factor has been
treated and removed, ATN usually resolves within 7 to 21 days. On occasion, the
kidneys may not completely recover or (rarely) may never recover, despite the
resolution of other medical problems. This situation usually indicates that there is
preexisting, unidentified renal dysfunction.
Anemia
Anemia is characterized by an insufficient number of red blood cells (RBCs). RBCs
carry oxygen from the lungs to tissues throughout the body. All cells require oxygen
to function.
Red blood cells originate in bone marrow as erythroblasts (a "blast" is a primitive cell
that develops into a mature cell). Hemoglobin (Hb), a protein that binds to oxygen,
is the main component of red blood cells. Once RBCs become filled with hemoglobin
they enter the bloodstream as erythrocytes. Healthy hemoglobin holds the oxygen
molecules with a precise degree of force. If it binds oxygen molecules in the lungs
too loosely, it cannot hold onto them and carry them away. If it binds them too
tightly, it cannot release them to tissues.
Red blood cell production is stimulated by the hormone erythropoietin (EPO), which
is produced in the kidneys. If the kidneys fail to produce adequate EPO, anemia
develops.
Blood Transfusion
Hospitals use blood supplied by blood banks (companies that collect, prepare, and
store blood for medical and emergency uses). Blood banks type blood and test the
compatibility of donor and recipient blood before transfusion (called cross-matching).
Blood types are A, B, AB, and O. Whether the type is positive or negative depends on
whether the Rh factor is present on the person's red blood cells.
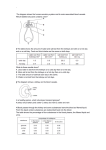
All types can receive O negative blood, but may not be compatible with other types:
Recipients with A+ blood type can receive A+, A-, O+ and O- blood types
Recipients with B+ blood type can receive B+, B-, O+ and O- blood types
Recipients with AB+ blood type can receive AB+, AB-, O+ and O- blood types.
Recipients with O+ blood type can receive O+ and O- blood types
Recipients with A- blood type can receive A- and O- blood types
Recipients with B- blood type can receive B- and O- blood types
Recipients with AB- blood type can receive AB- and O- blood types.
Recipients with O- blood type can receive O- blood type.
Blood products commonly transfused in intensive care units (ICUs) include
red blood cells (RBCs) – contain hemoglobin, which carries oxygen to all
tissues;
plasma – straw-colored fluid that carries the blood cells, enzymes, and
hormones throughout the body; and
platelets – cell-like bodies that control bleeding.
Blood banks also test blood for anemia and pathogens (disease-causing bacteria and
viruses), including hepatitis viruses B and C, human immunodeficiency virus (HIV),
and Treponema pallidum (bacterium that causes syphilis).
Despite the many regulations in place to assure the safety of blood supplies,
transfusions are not risk free. Possible complications of blood transfusions include
allergic reaction (caused by an allergen in the donor blood) and
hemolytic transfusion reaction (caused by incompatible blood).
Managing patients in ICU requires strategies to minimize blood loss and increase
production of blood in bone marrow. Limiting laboratory testing and phlebotomy
(drawing blood) are important components of blood management.
Other Treatment
Injectable EPO (e.g., PROCRIT®, EPOGEN®) is an alternative to blood transfusion to
treat critically ill patients with anemia. Exogenous EPO is identical to the natural
hormone in its role of stimulating the bone marrow to produce red blood cells. EPO
has been used safely in many clinical settings, including chronic renal failure,
oncology, and surgery. In the ICU, use of EPO has been shown to reduce the amount
of blood transfused by almost 50%, at the same time significantly increasing
hemoglobin levels.
Diabetic nephropathy
Diabetic nephropathy is kidney disease that develops as a result of diabetes mellitus
(DM). DM, also called simply diabetes, affects approximately 5% of the U.S.
population. This disease damages many organs, including the eyes, nerves, blood
vessels, heart, and kidneys. DM is the most common cause of kidney failure in the
United States and accounts for over one-third of all patients who are on dialysis.
Diabetes mellitus (DM)
Diabetes mellitus is a disorder in which the body is unable to metabolize
carbohydrates (e.g., food starches, sugars, cellulose) properly. The disease is
characterized by excessive amounts of sugar in the blood (hyperglycemia) and urine;
inadequate production and/or utilization of insulin; and by thirst, hunger, and loss of
weight.
Diabetics who require daily insulin shots to maintain life have insulin-dependent
diabetes mellitus, or DM 1. In this type of diabetes, the pancreas secretes little or
no insulin and the blood sugar level remains high, unless treated. DM 1 usually
occurs in children and young adults and is often called juvenile onset diabetes. Onset
of the disease is abrupt. The patient becomes very sick and requires immediate
insulin therapy. Approximately 1 million people in the United States have DM 1.
Non-insulin-dependent diabetes, or DM 2, differs from DM 1 in that the main
problem is a peripheral resistance to the action of the insulin. DM 2 usually occurs in
adults over the age of 40 who are overweight and have a family history of the
disease. Some patients can manage their diabetes with weight loss and changes in
their diet. Others require medication, and many with DM 2 eventually require insulin.
Onset is gradual, and patients may be sick for quite some time without knowing it.
Nearly 95% of diabetics are diagnosed with DM 2.
Signs and Symptoms
Approximately 25% to 40% of patients with DM 1 ultimately develop diabetic
nephropathy (DN), which progresses through about five predictable stages.
Stage 1 (very early diabetes)—Increased demand upon the kidneys is indicated by
an above-normal glomerular filtration rate (GFR).
Stage 2 (developing diabetes)—The GFR remains elevated or has returned to
normal, but glomerular damage has progressed to significant microalbuminuria
(small but above-normal level of the protein albumin in the urine). Patients in stage
2 excrete more than 30 mg of albumin in the urine over a 24-hour period. Significant
microalbuminuria will progress to end-stage renal disease (ESRD). Therefore, all
diabetes patients should be screened for microalbuminuria on a routine (yearly)
basis.
Stage 3 (overt, or dipstick-positive diabetes)—Glomerular damage has progressed
to clinical albuminuria. The urine is "dipstick positive," containing more than 300 mg
of albumin in a 24-hour period. Hypertension (high blood pressure) typically
develops during stage 3.
Stage 4 (late-stage diabetes)—Glomerular damage continues, with increasing
amounts of protein albumin in the urine. The kidneys' filtering ability has begun to
decline steadily, and blood urea nitrogen (BUN) and creatinine (Cr) has begun to
increase. The glomerular filtration rate (GFR) decreases about 10% annually. Almost
all patients have hypertension at stage 4.
Stage 5 (end-stage renal disease, ESRD)—GFR has fallen to approximately 10
milliliters per minute (<10 mL/min) and renal replacement therapy (i.e.,
hemodialysis, peritoneal dialysis, kidney transplantation) is needed.
Progression through these five stages is rather predictable because the onset of DM
1 can be identified, and most patients are free from age-related medical problems.
An estimated 5% to 15% of DM 2 cases also progress through the five stages of
diabetic nephropathy (DN), but the timeline is not as clear. Some patients advance
through the stages very quickly.
Diagnosis
Early screening for microalbuminuria is essential for all patients with diabetes.
Aggressive intervention can delay and possibly stop progression through the stages
of diabetic nephropathy (DN). Patients often seek medical attention only after having
progressed to stage 3 or 4. Those who have reached stage 3 should be referred to a
nephrologist (kidney specialist). The nephrologist monitors ongoing management and
conducts further diagnostic studies to exclude nondiabetic causes for protein in the
urine (proteinuria).
Treatment
Treatment for diabetic nephropathy attempts to manage and slow the progression of
the disease.
Aggressive blood pressure control is by far the most important factor in
protecting kidney function, regardless of the stage of DN. The goal of treatment is:
120–130 mm Hg systolic blood pressure and
70–80 mm Hg diastolic blood pressure.
Angiotensin-converting enzyme (ACE) inhibitors protect the kidneys more effectively
than other high blood pressure medications. A new class of blood pressure
medications known as angiotensin-receptor blockers (ARBs) may offer comparable
protection. Patients who cannot tolerate ACE inhibitors may use an ARB (e.g.,
losartan, valsartan). Maximum doses of an ACE along with an ARB may provide
additional renal protection in people who can tolerate the medications. Both ACE
inhibitors and ARBs can cause hyperkalemia (abnormally high level of potassium in
the blood) in patients with chronic renal failure.
Strict blood sugar control is important in the protection of kidney function.
Intensive blood sugar regulation requires frequent monitoring and commitment.
Dietary protein restriction is minimally protective. A high-protein diet (e.g., the
Atkins diet) can further damage the kidneys in people with diabetic nephropathy
and/or chronic renal failure (CRF). Protein restriction must be cautiously
implemented because of the risk for malnutrition. In general, dietary protein intake
should be limited to 0.6 to 0.8 grams per kilogram (0.02–0.028 oz/lb) of body
weight each day.
Renal Replacement Therapy
Once patients with DN progress to stage 5 (end-stage renal disease, ESRD), renal
replacement therapy (RRT) is implemented. The RRT options for DN patients include
the following:
Hemodialysis, removal of the blood's waste products through filtration
outside of the body
Peritoneal dialysis, filtration through the membrane lining the abdominal
cavity; fluid is instilled into the peritoneal space, and then drained
Kidney transplantation
Patients with DM 1 are possible candidates for combined kidney and pancreas
transplantation. A healthy insulin-producing pancreas eliminates the diabetes and the
potential for developing diabetic nephropathy.
Electrolyte Imbalance
Electrolytes are salts that conduct electricity and are found in the body fluid, tissue,
and blood. Examples are chloride, calcium, magnesium, sodium, and potassium.
Sodium (Na+) is concentrated in the extracellular fluid (ECF) and potassium (K+)
is concentrated in the intracellular fluid (ICF). Proper balance is essential for muscle
coordination, heart function, fluid absorption and excretion, nerve function, and
concentration.
The kidneys regulate fluid absorption and excretion and maintain a narrow range of
electrolyte fluctuation. Normally, sodium and potassium are filtered and excreted in
the urine and feces according to the body's needs. Too much or too little sodium or
potassium, caused by poor diet, dehydration, medication, and disease, results in an
imbalance. Too much sodium is called hypernatremia; too little is called
hyponatremia. Too much potassium is called hyperkalemia; too little is called
hypokalemia.
Incidence and Prevalence
Hyponatremia is the most common electrolyte imbalance. It is associated with kidney
disease such as nephrotic syndrome and acute renal failure (ARF). Men and women
with healthy kidneys have equal chances of experiencing electrolyte imbalance, and
people with eating disorders such as anorexia and bulimia, which most often affect
women, are at increased risk. Very young people and old people are affected more
often than young adults.
1. Hyponatremia
Causes
Hyponatremia is caused by conditions such as water retention and renal failure that
result in a low sodium level in the blood.
Pseudohyponatremia occurs when too much water is drawn into the blood; it is
commonly seen in people with hypoglycemia (low blood sugar).
Psychogenic polydipsia occurs in people who compulsively drink more than four
gallons of water a day.
Hypovolemic hyponatremia (with low blood volume due to fluid loss) occurs in
dehydrated people who rehydrate (drink a lot of water) too quickly, in patients
taking thiazide diuretics, and after severe vomiting or diarrhea.
Hypervolemic hyponatremia (high blood volume due to fluid retention) occurs in
people with liver cirrhosis, heart disease, or nephrotic syndrome. Edema (swelling)
often develops with fluid retention.
Euvolemic hyponatremia (decrease in total body water) occurs in people with
hypothyroidism, adrenal gland disorder, and disorders that increase the release of
the antidiuretic hormone (ADH), such as tuberculosis, pneumonia, and brain trauma.
Signs and Symptoms
Symptoms of hyponatremia are related to the severity and the rate at which the
conditions develop. The first symptoms are fatigue, weakness, nausea, and
headache. More severe cases cause confusion, seizure, coma, and death.
Treatment
The goal of treatment is to restore electrolyte balance for proper hydration and use
of total body fluid. Sodium deficiency must be corrected slowly because drastic
change in sodium level can cause brain cell shrinkage and central pontine
myelinolysis (damage to the pons region of the brain). Methods include:
Fluid and water restriction
Intravenous (IV) saline solution of 3% sodium
Salt tablets
Conivaptan (Vaprisol®) has been approved by the U.S. Food and Drug
Administration (FDA) to treat hypervolemic hyponatremia and euvolemic
hyponatremia in some hospitalized adults. Vaprisol is administered intravenously
(i.e., into a vein). Blood sodium levels should be closely monitored in patients who
receive this medication. Side effects include injection site reactions, headache,
thirst, and low potassium levels.
2. Hypernatremia
Hypernatremia is high sodium in the blood that occurs with excessive fluid loss.
When fluid is lost and not replaced, sodium is not adequately excreted from the
body.
The following are causes:
Diabetes insipidus (caused by deficiency of or insensitivity to ADH)
Diarrhea
Diuretic medication
Excessive salt intake
Excessive vomiting
Heavy respiration (e.g., exercise, exertion)
Severe burn
Sweating
It is associated with the same symptoms as hyponatremia, and also causes the
following:
Delerium
Irritability
Muscle twitching
Hypernatremia commonly affects older hospitalized people, 50% of whom have
underlying diseases that, when combined with excessive sodium and fluid loss, are
fatal.
Treatment
Treating hypernatremia involves slowly replenishing water loss, usually over 48
hours, through drinking or intravenous (IV) solution. In cases of diabetes, the
imbalance is treated with adequate water intake and nonsteroidal anti-inflammatory
drugs or with synthesized hormones (e.g., desmopressin) that aid in fluid retention
and decrease urination.
Some drugs used to treat electrolyte imbalance may be unsafe for pregnant women
and should not be taken before consulting a physician.
3. Hypokalemia
An abnormally low level of potassium (K+) is called hypokalemia. The adrenal gland
makes a hormone (aldosterone) that signals the kidneys to excrete or conserve
potassium, based on the body's needs. In hypokalemia, the adrenal gland retains the
hormone and the kidneys conserve potassium when more is needed.
Causes
The most common cause of potassium depletion is diuretic medication that
increases urination. Diuretics are prescribed for medical conditions and are used in
weight-loss programs. Other causes include:
Diarrhea
Dietary deficiency
Excessive sweating
Magnesium deficiency (causes overexcretion of fluid)
Signs and Symptoms
Symptoms of deficiency include cardiac arrhythmia, muscle pain, general discomfort or
irritability, weakness, and paralysis.
Diagnosis
Diagnosis may require urinalysis and blood tests to determine the amount of
potassium being excreted by the kidneys.
Treatment
Treatment involves potassium supplements, proper diet, and intravenous (IV)
solution. The best way to maintain an adequate potassium level is to eat foods such
as sweet potatoes, bananas, avocados, spinach, and oranges. Patients taking diuretic
medication are also given potassium supplements. Potassium is given slowly to avoid
hyperkalemia.
4. Hyperkalemia
An abnormally high level of potassium is called hyperkalemia. Potassium is released
into the blood when cells are damaged.
Causes
Conditions that cause hyperkalemia include:
Burns
Chemotherapy
Hemolysis (red blood cell destruction caused by infection or burn)
Rhabdomyolysis (destruction of skeletal muscle; associated with acute tubule
necrosis, or ATN)
Strenuous exercise (rarely)
Urinary excretion of potassium can be impaired by the following:
Acute renal failure (ARF)
Chronic renal failure (CRF)
Impaired aldosterone release or production
Medications that decrease potassium excretion:
o
Amiloride (diuretic)
o
Bactrim® (antibiotic)
o
Cyclosporine (immunosuppressive)
Signs and Symptoms
Hyperkalemia affects the heart and causes electrocardiogram (EKG) changes,
ventricular fibrillation, and cardiac arrest. Other symptoms include tingling in the
extremities, weakness, and numbness.
Treatment
Treatment of low-grade hyperkalemia may involve diuretics and calcium given
intravenously to promote potassium excretion. Insulin is given with glucose to help
cell absorption of potassium, and albuterol may be added to increase absorption.
Drugs that bind to potassium, such as Kayexalate®, force potassium into the
intestine to be excreted.
Some drugs used to treat electrolyte imbalance may be unsafe for pregnant women
and should not be taken without consulting a physician.
Renal artery stenosis
Renal artery stenosis (RAS) is the narrowing of the lining of the main artery that
supplies the kidney. Depending on the degree of narrowing, patients can develop
hypertension called renal vascular hypertension (RVH). This form of hypertension is
the most common cause of secondary hypertension.
RVH occurs when RAS produces a critical narrowing of the artery that supplies one of
the kidneys. Critical RAS is defined as at least 70% narrowing of the renal artery,
based on angiographic (blood vessel x-ray) evaluation.
Reduced blood flow through the renal artery causes the kidney to release increased
amounts of the hormone renin. Renin, a powerful blood pressure regulator, initiates
a series of chemical events that result in hypertension. Renal vascular hypertension
can be very severe and difficult to control.
The kidney with RAS suffers from the decreased blood flow and often shrinks in size
(atrophies). This process is called ischemic nephropathy. The other kidney is at risk
for developing damage from the hypertension. Often developing hypertensive
nephrosclerosis. The persistent elevated blood pressures in this non-stenotic kidney
can cause progressive scarring (sclerosis) leading to progressive loss of filtering
function in this kidney as well. Both unilateral RAS and bilateral RAS can ultimately
lead to chronic renal failure.
Atherosclerotic Renal Artery Stenosis (AS-RAS) and Fibromuscular
Dysplasia (FMD)
AS-RAS is due to the build-up of cholesterol on the inner lining of the renal artery. It
is exceedingly more common then the unusual case of FMD-RAS.
FMD-RAS
FMD-RAS occurs almost exclusively in women aged 30 to 40 and rarely affects
African Americans or Asians. FMD-RAS is due to an abnormality in the muscular
lining of the renal artery.
FMD-RAS is often not as well detected on MRA as it is on other non-invasive studies
such as, renal scan with ACE-inhibitor challenge, or ultrasound with Doppler
interrogation. FMD responds well to angioplasty and stenting. After plasty long-term
patency of the lesion is typically seen.
Incidence and Prevalence
Renal vascular disease accounts for less than 1% of all hypertension in people who
have moderately increased blood pressure. But in certain high-risk groups, renal
vascular disease may be the cause of 10% to 40 % of all hypertension. FMD RAS
occurs almost exclusively in women aged 30 to 40 and rarely affects African
Americans or Asians.
Risk Factors
Risk factors associated with the development of atherosclerotic RAS include the
following:
Carotid artery disease
Coronary artery disease
Diabetes mellitus
Hypertension (high blood pressure)
Obesity
Age
Peripheral vascular disease (vascular disease in the extremities, e.g., the
legs)
Smoking
There is often a familial history of FMD RAS.
Causes
Most RAS is caused by atherosclerosis or "hardening of the arteries." Atherosclerosis
is the build up of cholesterol deposits, or plaque, in the lining of the arteries.
Signs and Symptoms
Conditions that may indicate atherosclerotic RAS include the following:
Asymmetrical (differently sized and shaped) kidneys seen on ultrasound
History of calf pain when walking—indicates impaired circulation to the legs
Intolerance of specific antihypertensive medications—angiotensin-I (ACE-I)
inhibitors or angiotensin receptor blockers (ARBs)—with a sudden worsening
of renal function
More than three antihypertensive medications needed for blood pressure
control
New onset of hypertension in a patient over 55
Presence of a bruit (sound or murmur heard with a stethoscope) in the
abdomen (e.g., groin), neck, or other area
Sudden worsening of high blood pressure in a patient whose blood pressure
had been well controlled, especially if the patient is over 60
Diagnosis
The diagnostic method used for renal artery stenosis (RAS) is similar to that used for
ischemic nephropathy. The physician may also measure and compare the level of
renin, (blood pressure-regulating hormone released by the kidneys), within the right
to the left renal veins. If the amount of renin that is released by one-side is markedly
higher than the other, this identifies a high renin-releasing kidney consistent with
RAS.
Treatment
Medication (e.g., antihypertensive drugs) may be used to control hypertension (high
blood pressure).
Diuretics, ACE inhibitors, beta blockers, calcium channel blockers, and angiotensin
receptor blockers (ARBs) may be effective. A selective aldosterone inhibitor (e.g.,
eplerenone [Inspra®]) may be used to treat mild RAS.
These medications are discontinued if they cause a decrease in renal function. In
some cases, patients with RAS are resistant to medication for control of blood
pressure.
Angioplasty and stenting may be used to improve blood flow. The goal is to
improve the circulation of blood flow to the kidney and prevent the release of excess
renin, which can help to decrease blood pressure. This helps to prevent atrophy of
the kidney. In general, patients with AS-RAS should have stenting done because
plasty by itself has a very high incidence of re-stenosis.
Surgery to bypass the narrowing may be performed. If the kidney with RAS has
atrophied, a nephrectomy, surgical removal of the kidney, may be advised.
Prognosis
Patients with fibromuscular dysplasia (FMD) RAS often have good, long-term results
with angioplasty, but those with atherosclerotic RAS frequently experience a
recurrence. Even after partial or complete repair of the narrowed blood vessel, most
patients still have hypertension, but require less medication to control it.