Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
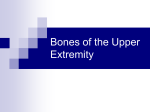
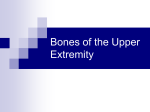
This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Snapping Scapula Syndrome Meredith A. Lazar, Young W. Kwon and Andrew S. Rokito J Bone Joint Surg Am. 2009;91:2251-2262. doi:10.2106/JBJS.H.01347 This information is current as of April 5, 2010 FREE Spanish Translation http://www.ejbjs.org/cgi/content/full/91/9/2251/DC1 Reprints and Permissions Click here to order reprints or request permission to use material from this article, or locate the article citation on jbjs.org and click on the [Reprints and Permissions] link. Publisher Information The Journal of Bone and Joint Surgery 20 Pickering Street, Needham, MA 02492-3157 www.jbjs.org 2251 C OPYRIGHT 2009 BY T HE J OURNAL OF B ONE AND J OINT S URGERY, I NCORPORATED Current Concepts Review Snapping Scapula Syndrome By Meredith A. Lazar, MD, Young W. Kwon, MD, PhD, and Andrew S. Rokito, MD ä Snapping scapula syndrome arises from either a soft-tissue or a skeletal anomaly within the scapulothoracic space that creates a cracking sound during scapulothoracic motion that patients associate with pain. ä Nonoperative measures consisting of supervised physical therapy, anti-inflammatory medications, and therapeutic injections are the mainstay of treatment. ä Open, arthroscopic, and combined operative approaches have been described for the treatment of refractory cases, with good overall outcomes in many relatively small case series. However, the optimal operative approach has yet to be determined. Snapping scapula syndrome, also known as scapulothoracic crepitus or bursitis, was first described in 1867 by Boinet1. The severity of the sounds associated with this syndrome were stratified by Mauclaire in 1904 as froissement (rustling), frottement (rubbing), or craquement (cracking), the latter of which was used to denote a sound so loud it must be pathological2. The sound is produced by a tactile-acoustic phenomenon occurring as a consequence of an anomalous tissue between the thoracic wall and the scapula. While most patients deem these sounds as a peculiar irregularity that does not produce symptoms, some report a clear correlation between the sounds and pain3. With an increasing knowledge base and advancing surgical technology, the available treatment modalities for such patients are continuing to evolve. This review will discuss the current approach to the diagnosis and treatment of patients with snapping scapula syndrome. Anatomy and Function of the Scapulothoracic Joint The scapula is a large, flat, triangular bone that lies along the posterior surface of the thoracic cage between the second and seventh ribs. It has two surfaces (ventral and dorsal), three borders (superior, axillary, and vertebral), and three angles (superomedial, inferomedial, and lateral)4. The scapula, in its static resting position, lies approximately 5 cm lateral to the spine on the posterior aspect of the thorax, is angled 30 to 40 in relation to the coronal plane, and is tipped anteriorly 10 to 20 with respect to the sagittal plane5. The scapula is part of the superior shoulder suspensory complex, which provides attachments to the axial skeleton. Its only skeletal connections are the acromi- oclavicular and coracoclavicular ligaments. Consequently, the scapula relies primarily on the surrounding muscles for support and stability. The contour of the scapula may vary, and, in one anatomic study, abnormalities were consistently found at the superomedial and inferior poles of the scapula6. The articulation between the scapula and the thoracic cage is one of the most incongruent in the human body. The scapulothoracic pseudojoint has three layers: superficial, intermediate, and deep7. Each layer consists of muscles and bursae. The superficial layer comprises the trapezius and latissimus dorsi muscles (Fig. 1). This layer can be associated with a well-circumscribed inferior angle bursa, measuring 1.9 · 2.4 cm on the average, located between the inferomedial angle of the scapula and the superficial fibers of the latissimus dorsi muscle7. The intermediate layer consists of the rhomboid major, rhomboid minor, and levator scapulae muscles. The trapezial bursa lies between the trapezius muscle and the base of the scapular spine and averages 4.3 · 2.7 cm in size. This bursa is particularly important as it provides a smooth surface over which the scapula rotates. In the intermediate layer, along with the trapezial bursa, is the spinal accessory nerve, which crosses the superior border of the scapula approximately 2.7 cm lateral to its superomedial angle as it enters the interval between the superomedial angle and the trapezius muscle just lateral to the levator scapulae muscle7. The dorsal scapular nerve is also in this vicinity as it enters the scapulothoracic region and travels deep to or through the levator scapulae parallel to the medial border of Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. Neither they nor a member of their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated. J Bone Joint Surg Am. 2009;91:2251-62 d doi:10.2106/JBJS.H.01347 2252 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d Fig. 1 Posterior view of the superficial layer of the scapulothoracic joint. The borders and angles of the scapula are identified, as are the spinal accessory nerve, the dorsal scapular nerve, and the suprascapular nerve. the scapula before innervating the rhomboid muscles8. The transverse cervical artery is divided by the levator scapulae muscle into the dorsal scapular artery and a branch that runs with the spinal accessory nerve9. The suprascapular nerve is also in proximity as it travels obliquely across the superomedial angle and superior border of the scapula and courses toward the suprascapular notch10. These structures are all at risk during operative treatment of scapulothoracic bursitis and must be carefully avoided during dissection9. The deep layer consists of the serratus anterior and subscapularis muscles and contains two discrete major bursae (Figs. 2-A and 2-B). The scapulothoracic, or supraserratus, bursa is located between the serratus anterior muscle and the thoracic cage and averages 9 · 7.4 cm in size. The subscapularis, or infraserratus, bursa is located between the serratus anterior and subscapularis muscles, is inconsistently present, and averages 5.3 · 5.3 cm7. The scapula plays a crucial role in the function of the upper extremity by providing a stable base for glenohumeral motion. In addition, the scapula glides against the thoracic wall to augment shoulder motion. Scapular motion is required to maintain optimal muscle length-tension relationships and alignment of the glenohumeral joint during elevation of the upper extremity11. Biomechanical analyses of normal scapular motion have revealed that the scapula can simultaneously rotate and translate along three axes to support glenohumeral motion12. The ratio of glenohumeral to scapulothoracic movement (GH/ST ratio) in various planes has been extensively studied and has been shown to be approximately 2:1 in both forward flexion and abduction. However, among the various planes, the GH/ST ratio has been found to vary in a nonlinear fashion depending on the position of the arm relative to the scapula. Several studies have shown the GH/ST ratio to range from 1.25 to 3.2, with the ratio in forward flexion being slightly higher on average than the ratio in abduction11,13,14. Specific rehabilitation protocols for stretching and strengthening the pectoral muscles, scapular retractors and elevators, and glenohumeral abductors and external rotators can increase the GH/ST ratio, which promotes scapular stability and improves glenohumeral motion15. Pathophysiology of Scapulothoracic Bursitis Scapulothoracic bursitis may occur following a single traumatic insult or as a result of a series of repetitive motions of the scapulothoracic joint16-18. In most cases, the bursitis is believed to be caused by abnormal motion between the anterior surface of the scapula and the thoracic cage. In 1933, Milch and Burman re- 2253 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d Fig. 2-A Fig. 2-B Anterior (Fig. 2-A) and cross-sectional (Fig. 2-B) views of the deep bursae in the scapulothoracic joint: the scapulothoracic and subscapularis bursae. 2254 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d ported on a small series of patients with scapulothoracic bursitis and suggested that the pain was caused by an abnormal forward curvature of the superomedial angle of the scapula due to various skeletal or soft-tissue abnormalities19. Scapulothoracic crepitus may be produced by an unusual shape of the scapula19. In a cadaver study, bending of >35 was noted in 8.6% (sixty) of 700 specimens6. Approximately 6% of scapulae demonstrate a hook-shaped prominence, known as the Luschka tubercle, at their superomedial angle6. This tubercle may enlarge and articulate with the thoracic cage, resulting in painful crepitus6. However, a clear causal relationship between this morphology and the presence of scapulothoracic bursitis has not been demonstrated. Osteochondroma is the most prevalent benign tumor of the scapula and has been implicated as a common cause of snapping scapula syndrome20-22. An extensive review of the literature identified eighty-nine cases of snapping scapula syndrome, with osteochondroma being the cause in 16% (fourteen)21. Other, less common, skeletal causes of scapulothoracic crepitus include skeletal exostoses and other osseous tumors, especially if they arise from the ventral surface of the scapula, and fracture malunion of either the ribs or the scapula23,24. The scapula is the second most frequent location of chondrosarcoma, which must be considered in the differential diagnosis of lesions in the scapulothoracic space25. Scapulothoracic bursitis may also occur following loss of dynamic control of scapular motion 26 . Abnormal scapular motion can be caused by muscle overuse, muscle imbalance following nerve injury, or pathological conditions of the glenohumeral joint27. Scapular dyskinesis has been observed in patients with known glenohumeral joint pathology and in specific series has been reported of fourteen of twenty-two patients with shoulder instability 28, seven of seven patients with impingement28, and fifteen of fifteen patients with rotator cuff abnormalities29,30 . Muscle atrophy secondary to nerve injury, trauma, or prior operative treatment can lead to diminished soft-tissue interposition between the scapula and the thoracic cage, resulting in scapulothoracic crepitus and pain5. When soft-tissue interposition is diminished, the scapula tilts, and thus a normally shaped scapula can appear to have an abnormally curved shape and dig into the chest wall31. The superomedial angle of the scapula then impinges along the chest wall during scapulothoracic motion and creates inflammation in the scapulothoracic space. Atrophy of the serratus anterior following injury to the long thoracic nerve as well as subscapularis atrophy in patients with thoracic outlet syndrome have also been implicated as etiologies of scapulothoracic crepitus32. Normal scapular motion along the thoracic cage is particularly important to athletes, and a history of overuse during activities such as swimming, pitching, weight training, gymnastics, and football has been implicated in the onset of symptoms5,33. A phenomenon described in pitchers known as SICK (scapular malposition, inferior medial border prominence, coracoid pain and malposition, and dyskinesis of scapular movement) has recently been recognized as an overuse mus- cular fatigue syndrome that has many of the same features as scapulothoracic bursitis34. Other causes of scapulothoracic bursitis include prior operative treatment that violated the periscapular musculature32. For example, in one series, snapping scapula syndrome developed in fifteen of 100 patients in whom thoracic outlet syndrome had been treated with resection of the first rib32. We have observed scapulothoracic bursitis in women who have undergone cosmetic breast procedures that involved subserratus exploration with implant placement. Clinical Presentation History Patients with snapping scapula syndrome who seek medical treatment primarily report activity-related pain and crepitus. These symptoms may have an insidious onset, occur after a change in activity pattern, or be associated with trauma21. The clinician should identify possible precipitating factors and question the patient regarding the duration and severity of the symptoms. In addition, symptoms such as shoulder girdle or neck pain and weakness should be documented. Other relevant elements of the history include hand dominance, occupation, and activity level, which may help to reveal causative factors. Crepitus associated with a soft-tissue lesion or muscle imbalance is typically softer than that associated with a skeletal lesion35. In addition, skeletal lesions may initially present with subtle findings such as a painless, enlarging mass that does not cause crepitus and that can be misdiagnosed as scapulothoracic bursitis36,37. In the absence of an identifiable lesion, the clinician must inquire about the frequency, level, and character of sports activities because those who engage in repetitive throwing, swimming, gymnastics, or weight-lifting are particularly susceptible to the development of scapular dyskinesis or bursitis34. Physical Examination The spine must first be inspected for any excessive curvature as this will create an abnormal contour about the thoracic cage, which in turn will directly alter scapular motion30. In one series, six of nine patients diagnosed with snapping scapula syndrome demonstrated kyphosis of the upper thoracic spine with no history of Scheuermann adolescent kyphoscoliosis38. Other postural conditions that have been associated with scapulothoracic dysfunction include a forward-tilted head, rounded shoulders, abducted and forward-tipped scapulae, and suboccipital extension. Patients should also be assessed for sources of referred pain, including cervical radiculopathy, neurological injuries, and pathological changes in the glenohumeral joint39. The shoulder girdle should then be inspected for any scapular asymmetry. This can be subtle and its identification can require careful assessment. In the presence of scapular dysfunction resulting from a nerve injury, patients have difficulty abducting the arm and may compensate by shifting the entire trunk in order to perform tasks that require arm abduction25. The position of the scapula should be documented during both ascending and descending shoulder motions as well as during scapular protraction, retraction, and rotation34. 2255 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d Fig. 3 This patient with an osteochondroma on the right scapula demonstrates scapular asymmetry with maximum internal rotation. Palpation of the periscapular region may reveal focal tenderness at the medial scapular border over the superomedial and/or inferomedial bursae. Adduction and internal rotation of the shoulder allow these borders to be accessed for easier palpation5. Patients often know how to reproduce the snapping by elevating and depressing the shoulder, and when they do so the crepitus can be localized from the undersurface of the scapula25. The active and passive ranges of motion of the shoulder should be carefully examined for any limitations. The strength of the scapular musculature, specifically the trapezius, rhomboids, levator scapulae, serratus anterior, and latissimus dorsi muscles, should also be assessed30. The trapezius muscle strength is evaluated by having the patient shrug the shoulders against resistance. The rhomboids and levator scapulae can be tested by having the patient place the hands on the hips and push the elbows backward against resistance. The serratus anterior is assessed by having the patient press against a wall with an outstretched arm while the examiner palpates the scapula for winging. The latissimus dorsi is tested with downward and backward pressure of the arm against resistance while the examiner palpates the inferomedial angle of the scapula. However, static manual muscle testing may not be sufficiently sensitive to detect subtle weakness in these muscles. It is thus critically important to characterize the dynamic motion of the scapula28. Scapular motion can be characterized by the position of the inferomedial or superomedial angle and by the plane in which it rotates—coronal or sagittal12. In the presence of a lesion, so-called clunking may be observed when the arm is abducted from 90 to 18020. Pseudo-winging of the scapula can be observed if a skeletal lesion pushes against the thorax to displace the scapula away from the body (Fig. 3)40. Weakness in the major scapular stabilizers (serratus anterior, trapezius, and rhomboid muscles) may present as different patterns of scapular winging. An injury of the long thoracic nerve causing atrophy of the serratus anterior results in lateral scapular winging. Injury to the spinal accessory nerve that results in trapezius atrophy may cause the shoulder to droop or rotate forward more medially and is often more subtle than the winging associated with dysfunction of the serratus anterior. Scapular winging becomes more evident with motion and stress testing. To evaluate for scapular winging, the examiner should observe the scapula and palpate the inferomedial angle during elevation. The scapula should also be observed while the patient pushes against a wall or performs a push-up, as these maneuvers accentuate the asymmetric movement of the scapula25. If a neurological injury is suspected, electrodiagnostic studies (electromyography and/or measurement of nerve conduction velocities) can be performed to determine whether the results correlate with those of the clinical examination41. Posterior capsular tightness may also be present, especially in throwing athletes. Evaluating external and internal rotation of both shoulders with the humerus at 90 in the coronal plane is useful to assess capsular tightness42. The upper trapezius and the pectoralis minor are other common sites of myofascial tightness. Hypertonia in athletes with shoulder pain can also contribute to scapular dyskinesis43. Imaging Imaging modalities used in the evaluation of snapping scapula syndrome include plain radiographs, computed tomography, magnetic resonance imaging, and ultrasonography. Standard radiographs of the scapula include a true anteroposterior view (with the scapula lying flat against the cassette or the beam tilted to account for the scapular angle), a tangential transscapular (or Y) view (with the beam pointed in line with the spine of the scapula), and an axillary lateral view (to assess the glenohumeral joint). These projections help identify skeletal irregularities such as osteochondromas, a Luschka tubercle, rib abnormalities, or alterations at the superomedial or inferomedial angle of the scapula (Fig. 4)6. Lesions that arise from the ventral surface of the scapula are particularly apparent in the scapulothoracic space on the Y view, as are sagittal plane deformities at the superomedial or inferomedial angle. Unfortunately, these lesions are not always readily visible on radiographs, and fluoroscopy has been suggested as an adjunctive tool to dynamically visualize the grating or snapping of the scapula23. Several case reports have documented the utility of cineradiography to identify skeletal lesions in patients with scapulothoracic crepitus44. The efficacy of computed tomography scanning for the routine evaluation of scapulothoracic crepitus has remained controversial. While a retrospective study did demonstrate high intraobserver and interobserver agreement with regard to the assessment of computed tomography scans for scapular crepitus, the interpretations of these scans did not correlate well with the clinical findings45. Therefore, the authors suggested that the routine use of computed tomography was not justified for patients with the clinical diagnosis of scapulothoracic crepitus45. Similarly, a more recent study demon- 2256 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d tion47. Thus far, however, the use of ultrasound for diagnosis or treatment of scapulothoracic crepitus appears to be infrequent and published data are mostly limited to case reports47,48. Fig. 4 Tangential radiograph of a scapular osteochondroma (arrow), demonstrating how these lesions may encroach on the scapulothoracic space and cause bursitis. strated fairly poor correlation between findings on computed tomography scans and clinical symptoms46. The authors of that study also noted that computed tomography scans, especially three-dimensional reconstructions, were reliable in detecting abnormalities and incongruities between the scapula and the thoracic cage in multiple planes, suggesting that these images may be important adjuncts to plain radiographs for the planning of operative treatment of scapulothoracic crepitus. Given these findings, we believe that a computed tomography scan would be a useful adjunct to plain radiographs if a bone or cartilage lesion is visible and requires further characterization for preoperative planning (Fig. 5). Magnetic resonance imaging is better than computed tomography scans for identifying and characterizing soft-tissue masses. Higuchi et al. reported their experience with using magnetic resonance imaging to evaluate scapulothoracic bursitis and found it to be more useful than computed tomography scans for assessing fluid-filled bursal tissue as well as for distinguishing scapulothoracic bursitis from elastofibroma36. They and other authors37 concluded that magnetic resonance imaging is a valuable tool for assessing these so-called pseudotumors in the scapulothoracic bursa. Ultrasound has also been used to identify and treat scapulothoracic pathology. Specifically, by identifying the bursal tissue dynamically, it can be used for image-guided injec- Nonoperative Treatment The majority of patients with scapulothoracic crepitus or bursitis can be managed successfully without operative treatment. An operation is required only for patients who have a clearly identifiable osseous or soft-tissue mass. Nonoperative treatment options include physical therapy, anti-inflammatory medications, and corticosteroid injections49. The goals of rehabilitation for patients with snapping scapula syndrome are improving muscle strength and balance, addressing postural conditions (such as excessive thoracic kyphosis), and core strengthening30,34,50. It is believed that poor posture with the head and shoulders tipped forward causes the posterior scapular stabilizers to weaken relative to the anterior pectoral muscles, which leads to imbalances that may change the scapular resting position and decrease scapular elevation15. Kibler and McMullen identified three stages of rehabilitation based on a program in which the shoulder is considered to be part of a kinetic chain system30. The kinetic chain model depicts the body as a system of interdependent parts that work in a proximal-to-distal sequence to impart a desired action at the distal segment. In kinetic chain shoulder rehabilitation, the lower limbs and the trunk are integrated into most of the exercises, which reinforces normal movement patterns from the outset43. Arm elevation requires full scapular retraction, which is incumbent on spine and hip extension to accommodate scapular motion. Therefore, shoulder function is dependent on thoracic spinal control, which must be reestablished with physical therapy prior to strengthening individual shoulder muscles43. Lower scapular stabilization can be Fig. 5 Three-dimensional computed tomography reconstruction in the coronal plane, demonstrating an osteochondroma (arrow) along the anterior surface of the scapula. 2257 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d facilitated through contraction of the contralateral gluteus maximus muscles through the thoracolumbar fascia, which connects to the latissimus dorsi muscle. Efficient shoulder motion and muscle activation occur in this proximal-to distal sequence, which is the basis for the ten-week rehabilitation protocol. The program progresses in a stepwise fashion from the acute phase (zero to three weeks), to the recovery phase (three to eight weeks), and finally to the maintenance phase (six to ten weeks) with specific exercises prescribed at each interval, bearing in mind that function, rather than time, determines a patient’s overall progress with this protocol30. In the acute phase, the goal of rehabilitation is to reduce pain. Consequently, those movements and positions associated with discomfort are limited. Trunk flexion and rotation exercises are performed so that scapular motion can be achieved without moving the arm, which may be painful. Patients are instructed to perform so-called safe co-contractions, in which the hand is supported so that the gravitational force on the arm is eliminated and pain is minimized51. Abnormal scapular motion has been attributed to excessive activation of the upper trapezius muscle combined with decreased control of the lower trapezius and the serratus anterior muscle. To restore muscle control and balanced coactivation, exercises that selectively recruit weaker muscles over hyperactive muscles are recommended52. Stretching maneuvers are performed in conjunction with closed-kinetic-chain exercises, in which the hand is relatively fixed (such as in modified push-ups) and which require less muscle activation than open-chain exercises (dumbbell press and machine-rowing)30,51. In the recovery phase of rehabilitation, strengthening is performed with motion, which is dependent on the proper posture that has already been established in the acute phase. Closedkinetic-chain exercises are advanced and should be performed in multiple planes and levels of elevation to reproduce scapular motion in its varied positions. Cools et al. performed an electromyographic study to elucidate which shoulder girdle exercises selectively activate middle and lower portions of the trapezius and serratus anterior muscles over the upper trapezius muscle to restore balance to the scapulothoracic musculature52. Side-lying forward flexion, side-lying external rotation, and prone horizontal abduction with external rotation all had favorable upperto-lower trapezius-muscle recruitment ratios (Figs. 6-A, 6-B, and 6-C). These arm elevation and rotation exercises should be added and weights should be increased as tolerated by the patient during this recovery phase of rehabilitation. Exercises are also performed to continue to strengthen the kinetic chain. Core strength endurance training helps to facilitate dynamic postural control for prolonged periods of time5. The maintenance phase begins once good scapular control and motion have been achieved. Plyometric (dynamic stretch-shortening) exercises such as tossing a medicine ball and open-chain exercises such as the walking lunge with a shoulder dumbbell press are advanced and integrated. Performance of strengthening exercises in various planes while loading the glenohumeral joint is also prescribed30. Fig. 6-A Fig. 6-B Fig. 6-c Figs. 6-A, 6-B, and 6-C Exercises that selectively restore trapezial 52 muscle balance . Fig. 6-A Side-lying forward flexion. Fig. 6-B Side-lying external rotation. Fig. 6-C Prone abduction and external rotation. Ciullo reported excellent results in sixty-two of seventytwo patients treated with a combination of diathermy, ultrasound, and iontophoresis along with periscapular and rotator cuff muscle strengthening 53. In another study, Groh et al. found good or excellent results in twenty-two of thirty patients treated with periscapular muscle strengthening50. A corticosteroid and/or local anesthetic can be injected into the scapulothoracic bursa for diagnostic and therapeutic purposes. These injections are best administered with the patient prone and in the so-called chicken-wing position, with the shoulder extended and internally rotated to elevate the medial border of the scapula (Fig. 7)49. Care must be taken to direct the needle parallel to the chest wall as pneumothorax is a potential complication35. The injection should be directed to- 2258 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d clinical benefits of this modality have not been demonstrated, however. Operative Treatment Indications Operative management may be considered for patients who have undergone a prolonged course of nonoperative treatment with little or no improvement16,56-60. Ideally, these patients should be able to localize the pain to the superomedial or inferomedial angle of the scapula. The operative outcome is more reliable if the diagnosis can be confirmed with a preoperative injection of local anesthetic5,55,58. Lehtinen et al. suggested that failure to receive at least temporary relief from an injection should be a relative contraindication to operative management26. Other relative predictors of a poor operative outcome include the ability to voluntarily produce the snapping sound from the scapula, involvement in a Workers’ Compensation claim or litigation, and documented nerve deficits5. Fig. 7 The so-called chicken-wing position elevates and defines the potential space for injection at the superior or inferior (arrow) bursa. ward the superomedial or inferomedial angle of the scapula, depending on the location of the pain and the point of maximal tenderness. Hodler et al. investigated the efficacy and accuracy of injections for the treatment of scapulothoracic bursitis54. In a study of twenty patients who received injections, eighteen reported improvement. The injection site was sterilized, and the skin and needle track were anesthetized with 1% lidocaine. A 22 or 25-gauge 9-cm needle was inserted until the pain was triggered. After location of the bursa under fluoroscopy, lidocaine and contrast medium were injected; this was followed by injection of betamethasone and bupivacaine. The contrast medium was injected as part of the study protocol to assess the accuracy of the injection and identify the presence of a true bursal sac. In seven patients, the contrast medium filled a smooth, well-defined bursal sac. In eight patients, the injection was placed intramuscularly as demonstrated by diffuse spreading of the contrast medium. In the remaining five patients, some of the contrast medium pooled into a well-defined bursa and some spread diffusely. The eighteen successfully treated patients had a significant improvement in the visual analog pain scores that lasted from six hours to fifteen months. The authors concluded that injections are a safe and effective way to treat scapulothoracic bursitis. In addition, even patients without a well-defined bursa may have relief of pain after a localized injection54. Other authors have reported similar efficacy of corticosteroid injections administered to provide temporary relief prior to surgical treatment16,26,55. The use of ultrasound-guided injections is currently under investigation. Its perceived advantage is better visualization of the soft tissues, including adhesions, scarring, and bursal collections, to facilitate more accurate injections47. Clear Open Techniques and Results To our knowledge, the first report of operative treatment for snapping scapula was published in 19503. The procedure was performed with the use of local anesthesia in three patients who were asked to move the shoulder during the operation in order to identify the portion of the scapula responsible for the symptoms so that it could be resected. Subsequent studies have shown good outcomes following open partial scapular resection, usually for treatment of a distinct osseous abnormality 21,23,44,55,59,61. The procedure is typically performed with the patient in either the prone or the lateral decubitus position with the involved extremity draped free. With internal rotation of the shoulder, the medial border of the scapula can be lifted away from the thoracic cavity. The location of the skin incision is vertical, is in line with the medial border of the scapula, and is centered either superiorly or inferiorly depending on the site of the primary pathological findings. For operative dissection of the superomedial angle of the scapula (Fig. 8), the trapezius muscle may be split in line with its fibers over the scapular spine to expose the underlying structures. During this portion of the procedure, it is imperative to protect the spinal accessory nerve, which crosses the superior border of the scapula just lateral to the superomedial angle—i.e., between the superomedial angle and the trapezius muscle just lateral to the levator scapulae7. The levator scapulae and rhomboid muscles can be released subperiosteally as needed to expose the anteromedial border of the scapula. Care must be taken when the rhomboids are detached to avoid injury to the dorsal scapular nerve, which is approximately 2 cm medial to the medial scapular edge26. Finally, the involved osseous anomaly and/or the inflamed bursae can be isolated and resected. With this approach, the rhomboids are detached subperiosteally in order to preserve the short Sharpey fibers of the tendinous insertions, which may be reattached through drill holes to their appropriate position55. Although postoperative regimens may vary, most authors have recommended a period of immobili- 2259 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d Fig. 8 Technique for open resection of the superomedial angle of the scapula. a: A longitudinal incision is made along the medial scapular edge, and subcutaneous undermining exposes the trapezius muscle, which is split and elevated in line with its fibers over the medial aspect of the scapula. b: The rhomboid and levator muscles are detached from the medial and superior edge to expose the superomedial edge of the scapula. c: The rotator cuff muscles are elevated in the subperiosteal plane so that the bone is exposed completely. d: The exposed portion of bone is removed. e: The muscles are then reattached through bone tunnels to their anatomic insertion on the scapula. (Reprinted, with permission, from: Lehtinen JT, Macy JC, Cassinelli E, Warner JJ. The painful scapulothoracic articulation: surgical management. Clin Orthop Relat Res. 2004;423:99-105.) zation in a sling for up to four weeks to allow the muscles to heal to the bone, followed by exercises for restoration of the range of motion and for strengthening26,27,33,55,56. Open treatment for scapulothoracic crepitus and bursitis has resulted in good-to-excellent outcomes in the majority of patients18,33,56,62. McCluskey and Bigliani treated nine patients with refractory scapulothoracic bursitis at the supraserratus bursa with isolated open bursectomy 56. Fibrotic bursal tissue between the serratus anterior muscle and the thoracic cavity was excised. They reported six excellent and two good results. The remaining patient experienced a spinal accessory nerve deficit that required a tendon transfer, and only a fair outcome was achieved. More recently, Nicholson and Duckworth reported on seventeen patients in whom scapulothoracic pain had been treated with an open operative technique55. All of their patients had a satisfactory outcome after an average duration of followup of 2.5 years. In addition to removal of bursal tissue, the superomedial angle of the scapula was resected in five patients. The authors noted that open osseous resection was able to address other abnormalities about the area as well as provide easy access to the trapezial bursa55. In this and other series in which removal of a portion of the superomedial angle was reported, gross and histological examination showed the resected bone to be essentially normal18,44,55,59. Like resection for the treatment of supraserratus bursitis, operative treatment of inferomedial scapulothoracic bursitis has yielded satisfactory outcomes. In a small series of four professional baseball pitchers, Sisto and Jobe performed an open bursectomy at the inferior angle of the scapula33. Histological evaluation of the resected tissue revealed evidence of chronic inflammation. All patients experienced complete or nearly complete relief of symptoms and were able to return to baseball at their previous level of competition. Arthroscopic Techniques and Results Although technically demanding, arthroscopic surgery for snapping scapula syndrome offers several theoretical advantages over open operative treatment. These include minimizing dissection and preserving muscle attachments, thereby eliminating the need for postoperative immobilization and potentially shortening the rehabilitation period58. Other advantages include an improved cosmetic appearance and potentially decreased hospital stays. The patient is usually positioned prone with the arm extended and internally rotated to accentuate the medial border of the scapula49. Some authors have recommended the lateral decubitus position as it allows concurrent evaluation of the glenohumeral joint10. Once the patient is positioned, the osseous landmarks are marked on the skin in anticipation of portal placement (Fig. 9). All standard portals should be established at least 3 cm medial to the medial border of the scapula to avoid injuring the dorsal scapular nerve and vessels. Along the vertical axis, the 2260 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d Fig. 9 Arthroscopic landmarks and portal placement. The superior visualization portal is 3 cm medial to the medial border of the scapula just inferior to the scapular spine, and the inferior working portal is made midway between the spine and the inferomedial angle. superior visualization portal should be placed just inferior to the scapular spine to allow access to both the superomedial and the inferomedial angle of the scapula. Under arthroscopic visualization, the inferior working portal is then created midway between the scapular spine and the inferomedial scapular angle. The instruments should point away from the coracoid process to prevent damage to the suprascapular nerve and vessels, which travel just medial to the base of the coracoid9. The visualization and working portals may be interchanged as needed intraoperatively for improved access to the bursal tissues. Portals placed superior to the scapular spine may result in injury to the dorsal scapular nerve and vessels or the spinal accessory nerve, and should be avoided. If access to the superomedial angle of the scapula from these portals is limited, a second working portal can be created superiorly and laterally. With use of a so-called inside-out technique, this superolateral portal can be located along the superior border of the scapula at a distance that is one-third of the distance between the superomedial angle and the acromion. Cadaver dissection and clinical outcome studies have demonstrated that this portal can be established without excessive risk to the suprascapular nerve and vessels10,17. During the bursectomy, it is important to maintain a proper orientation relative to the thoracic cavity and clearly identify the soft-tissue structures prior to débridement49. In some patients, the bursal tissue is easily identifiable while, in others, the tissue appears to be thickened or fibrotic (Fig. 10). An advantage to arthroscopic débridement is that the periosteal sleeve of the rhomboid attachment is maintained, which avoids the need for muscle reattachment and thus eliminates the necessity for postoperative immobilization26. After the bursectomy is completed, the arm may be moved under direct visualization by the surgeon and if the superomedial angle is deemed prominent a partial scapular resection can be performed. If there is no prominence, the scapulothoracic space may be temporarily deflated by removing all of the arthroscopy fluid. An examination may then be performed with the patient under anesthesia to determine if the superomedial angle of the scapula impinges on deeper structures16. If there is osseous impingement, the scapula can then be skeletonized with a radiofrequency tissue ablator, and the superomedial angle can be resected with use of a high-speed burr. Although the exact extent of bone resection has been debated, most authors have recommended removing 2 to 3 cm of bone from the superomedial corner of the scapula26,44,63. Before the procedure is completed, the scapulothoracic joint should be examined with the patient under anesthesia to ensure that no impinging structures remain. Most reports on the outcomes of arthroscopic surgery for scapulothoracic bursitis and crepitus are small case series with short-term follow-up. In general, however, good-toexcellent results have been reported in the majority of patients. Failures have been attributed mostly to poor patient selection and technical difficulties16,17,53,58. In a recent longer-term follow-up study, thirteen patients underwent arthroscopic scapulothoracic bursectomy with or without bone resection of the superomedial angle16. At a mean of 6.8 years following surgery, all patients still reported Fig. 10 Intraoperative photograph showing arthroscopic débridement of the scapulothoracic bursa. The inflamed bursal tissue is removed from the scapula and débrided from the subscapularis muscle. 2261 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d some degree of scapulothoracic crepitus. Nine of the thirteen patients, however, reported less pain and improved function. The authors, therefore, suggested that residual scapulothoracic crepitus does not preclude a satisfactory outcome. In addition, they emphasized the importance of patient selection as their four patients with a failure included those with a history of drug abuse, C7 radiculopathy with clear scapular winging, and severe thoracic scoliosis16. Combined Techniques and Results Although the specific indications are still unclear, a combined arthroscopic and open approach may be appropriate for some patients. Bursectomy allows débridement of all inflamed tissue that may be the source of pain, and partial scapular resection (when indicated on the basis of the intraoperative examination) relieves the osseous impingement that contributes to the bursitis. Lehtinen et al. reported on sixteen patients with scapulothoracic bursitis and crepitus who were treated with either an all-arthroscopic procedure, an all-open procedure, or a combined procedure in which the bursectomy was completed in an arthroscopic fashion but bone resection was performed with use of an open approach26. At an average of three years postoperatively, thirteen of the sixteen patients were satisfied with the result and had improved function. With such a limited number of patients, however, it was unclear if any particular approach was superior to the others. In another series, twelve patients were followed after they had undergone a combined arthroscopic bursectomy and mini-open scapular resection57. At a mean of three years, the pain had decreased significantly in ten of the twelve patients. The theoretical advantage of a combined approach is that arthroscopy provides better visualization and access to the bursal tissue for a more complete bursectomy and an open approach provides improved exposure so that the surgeon is better able to judge and then resect the superomedial or inferomedial angle of the scapula when indicated26. In the literature, the recommended amount of bone resection has varied26,44,58,63. It is believed that a more appropriate resection of bone can be performed through an open approach; however, with an open approach, the muscles must be detached from the scapula and then reattached through bone tunnels, thus requiring a more extended postoperative immobilization period and a delay in the initiation of the rehabilitation protocol26,57. In an effort to improve the all-arthroscopic approach, the authors of a recent cadaver study attempted to identify landmarks that would allow the entire procedure to be performed arthroscopically, thereby avoiding the need for the aggressive muscle detachment that is performed with open techniques. However, this approach has not yet been applied to clinical practice63, to our knowledge. Overview Scapulothoracic crepitus or bursitis, also known as snapping scapula syndrome, has been recognized for more than a century. However, the entity is often underappreciated and is probably underdiagnosed. Without a definable skeletal lesion, most radiographic imaging modalities have been shown to be of little value in identifying the pathological entity and directing treatment. Thus, although this entity can be associated with either skeletal or soft-tissue anomalies or lesions, the diagnosis is generally established on the basis of the clinical history and physical examination alone. Nonoperative management with anti-inflammatory medications, supervised physical therapy, and corticosteroid injections is usually successful in alleviating symptoms. Operative intervention can be considered for patients whose symptoms persist and cause substantial disability. Open, arthroscopic, and combined techniques have been reported to have successful outcomes. The literature, however, consists mostly of small case series with varying operative indications and techniques. Further investigation is needed to clearly establish optimal treatment options for this complex condition. n Meredith A. Lazar, MD Young W. Kwon, MD, PhD Andrew S. Rokito, MD Department of Orthopedics, New York University Hospital for Joint Diseases, 301 East 17th Street, 14th Floor, New York, NY 10003. E-mail address for M.A. Lazar: [email protected] References 1. Boinet. Fait clinique. Bull Mem Sec Chir Paris. 1867;8:458. 2. Mauclaire. Craquements sous-capsulaires pathologiques traités par l’interposition musculaire interscapulo-thoracique. Bull Mem Soc Chir Paris. 1904;30:164-8. 3. Milch H. Partial scapulectomy for snapping of the scapula. J Bone Joint Surg Am. 1950;32:561-6. 4. Gray H. Anatomy of the human body. Lewis WH, editor. 20th ed. New York: Bartleby.com; 2000. 5. Manske RC, Reiman MP, Stovak ML. Nonoperative and operative management of snapping scapula. Am J Sports Med. 2004;32:1554-65. 6. Edelson JG. Variations in the anatomy of the scapula with reference to the snapping scapula. Clin Orthop Relat Res. 1996;322:111-5. 7. Williams GR Jr, Shakil M, Klimkiewicz J, Iannotti JP. Anatomy of the scapulothoracic articulation. Clin Orthop Relat Res. 1999;359:237-46. 8. Frank DK, Wenk E, Stern JC, Gottlieb RD, Moscatello AL. A cadaveric study of the motor nerves to the levator scapulae muscle. Otolaryngol Head Neck Surg. 1997;117:671-80. 9. Ruland LJ 3rd, Ruland CM, Matthews LS. Scapulothoracic anatomy for the arthroscopist. Arthroscopy. 1995;11:52-6. 10. Chan BK, Chakrabarti AJ, Bell SN. An alternative portal for scapulothoracic arthroscopy. J Shoulder Elbow Surg. 2002;11:235-8. 11. McClure PW, Michener LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:269-77. 2262 T H E J O U R N A L O F B O N E & J O I N T S U R G E RY J B J S . O R G V O L U M E 9 1-A N U M B E R 9 S E P T E M B E R 2 009 d d SNAPPING SCAPULA SYNDROME d 12. Kibler WB, Uhl TL, Maddux JW, Brooks PV, Zeller B, McMullen J. Qualitative clinical evaluation of scapular dysfunction: a reliability study. J Shoulder Elbow Surg. 2002;11:550-6. 13. Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24:57-65. 14. Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976;58:195-201. 15. Wang CH, McClure P, Pratt NE, Nobilini R. Stretching and strengthening exercises: their effect on three-dimensional scapular kinematics. Arch Phys Med Rehabil. 1999;80:923-9. 16. Pearse EO, Bruguera J, Massoud SN, Sforza G, Copeland SA, Levy O. Arthroscopic management of the painful snapping scapula. Arthroscopy. 2006; 22:755-61. 17. Pavlik A, Ang K, Coghlan J, Bell S. Arthroscopic treatment of painful snapping of the scapula by using a new superior portal. Arthroscopy. 2003;19:608-12. 18. Richards RR, McKee MD. Treatment of painful scapulothoracic crepitus by resection of the superomedial angle of the scapula. A report of three cases. Clin Orthop Relat Res. 1989;247:111-6. 19. Milch H, Burman MS. Snapping scapula and humerus varus. Report of six cases. Arch Surg. 1933;26:570-88. 20. Fukunaga S, Futani H, Yoshiya S. Endoscopically assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J Surg Oncol. 2007;5:37. 21. Carlson HL, Haig AJ, Stewart DC. Snapping scapula syndrome: three case reports and an analysis of the literature. Arch Phys Med Rehabil. 1997;78:506-11. 22. van Riet RP, Van Glabbeek F. Arthroscopic resection of a symptomatic snapping subscapular osteochondroma. Acta Orthop Belg. 2007;73:252-4. 37. Ken O, Hatori M, Kokubun S. The MRI features and treatment of scapulothoracic bursitis: report of four cases. Ups J Med Sci. 2004;109:57-64. 38. Cobey MC. The rolling scapula. Clin Orthop Relat Res. 1968;60:193-4. 39. Neer CS. Shoulder reconstruction. Philadelphia: WB Saunders; 1990. 40. Andrews JR, Wilk KE. The athlete’s shoulder. New York: Churchill Livingstone; 1994. 41. Lehtinen JT, Tetreault P, Warner JJ. Arthroscopic management of painful and stiff scapulothoracic articulation. Arthroscopy. 2003;19:E28. 42. Tyler TF, Nicholas SJ, Roy T, Gleim GW. Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med. 2000;28:668-73. 43. McMullen J, Uhl TL. A kinetic chain approach for shoulder rehabilitation. J Athl Train. 2000;35:329-37. 44. Oizumi N, Suenaga N, Minami A. Snapping scapula caused by abnormal angulation of the superior angle of the scapula. J Shoulder Elbow Surg. 2004; 13:115-8. 45. de Haart M, van der Linden ES, de Vet HC, Arens H, Snoep G. The value of computed tomography in the diagnosis of grating scapula. Skeletal Radiol. 1994;23:357-9. 46. Mozes G, Bickels J, Ovadia D, Dekel S. The use of three-dimensional computed tomography in evaluating snapping scapula syndrome. Orthopedics. 1999;22:1029-33. 47. Saboeiro GR, Sofka CM. Imaging-guided treatment of scapulothoracic bursitis. HSS J. 2007;3:213-5. 48. Huang CC, Ko SF, Ng SH, Lin CC, Huang HY, Yu PC, Lee TY. Scapulothoracic bursitis of the chest wall: sonographic features with pathologic correlation. J Ultrasound Med. 2005;24:1437-40. 23. Parsons TA. The snapping scapula and subscapular exostoses. J Bone Joint Surg Br. 1973;55:345-9. 49. Millett PJ, Pacheco IH, Gobezie R, Warner JJP. Management of recalcitrant scapulothoracic bursitis: endoscopic scapulothoracic bursectomy and scapuloplasty. Tech Shoulder Elbow Surg. 2006;7:200-5. 24. Takahara K, Uchiyama S, Nakagawa H, Kamimura M, Ohashi M, Miyasaka T. Snapping scapula syndrome due to malunion of rib fractures: a case report. J Shoulder Elbow Surg. 2004;13:95-8. 50. Groh GI, Simoni M, AIIen T, Dwyer T, Heckman MM, Rockwood CA Jr. Treatment of snapping scapula with a periscapular muscle strengthening program [abstract]. J Shoulder Elbow Surg. 1996;5(2-Pt 2):S6. 25. Rockwood CA Jr, Matsen FA III, Wirth MA, Lippitt SB. The shoulder. 3rd ed. Philadelphia: Saunders; 2004. 51. Kibler WB, Livingston B. Closed-chain rehabilitation for upper and lower extremities. J Am Acad Orthop Surg. 2001;9:412-21. 26. Lehtinen JT, Macy JC, Cassinelli E, Warner JJ. The painful scapulothoracic articulation: surgical management. Clin Orthop Relat Res. 2004;423:99-105. 52. Cools AM, Geerooms E, Van den Berghe DF, Cambier DC, Witvrouw EE. Isokinetic scapular muscle performance in young elite gymnasts. J Athl Train. 2007;42:458-63. 27. Strizak AM, Cowen MH. The snapping scapula syndrome. A case report. J Bone Joint Surg Am. 1982;64:941-2. 28. Warner JJ, Micheli LJ, Arslanian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moiré topographic analysis. Clin Orthop Relat Res. 1992;285:191-9. 29. Paletta GA Jr, Warner JJ, Warren RF, Deutsch A, Altchek DW. Shoulder kinematics with two-plane x-ray evaluation in patients with anterior instability or rotator cuff tearing. J Shoulder Elbow Surg. 1997;6:516-27. 30. Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003;11:142-51. 31. Matsen FA 3rd, Lippitt SB, Sidles JA, Harryman DT 2nd. Practical evaluation and management of the shoulder. Philadelphia: WB Saunders; 1994. 53. Ciullo JV. Subscapular bursitis: treatment of ‘‘snapping scapula’’ or ‘‘washboard syndrome’’. Arthroscopy. 1992;8:412-3. 54. Hodler J, Gilula LA, Ditsios KT, Yamaguchi K. Fluoroscopically guided scapulothoracic injections. AJR Am J Roentgenol. 2003;181:1232-4. 55. Nicholson GP, Duckworth MA. Scapulothoracic bursectomy for snapping scapula syndrome. J Shoulder Elbow Surg. 2002;11:80-5. 56. McCluskey GM III, Bigliani LU. Surgical management of refractory scapulothoracic bursitis. Orthop Trans. 1991;15:801. 57. Lien SB, Shen PH, Lee CH, Lin LC. The effect of endoscopic bursectomy with mini-open partial scapulectomy on snapping scapula syndrome. J Surg Res. 2008;150:236-420. 32. Wood VE, Verska JM. The snapping scapula in association with the thoracic outlet syndrome. Arch Surg. 1989;124:1335-7. 58. Harper GD, McIlroy S, Bayley JI, Calvert PT. Arthroscopic partial resection of the scapula for snapping scapula: a new technique. J Shoulder Elbow Surg. 1999;8:53-7. 33. Sisto DJ, Jobe FW. The operative treatment of scapulothoracic bursitis in professional pitchers. Am J Sports Med. 1986;14:192-4. 59. Morse BJ, Ebraheim NA, Jackson WT. Partial scapulectomy for snapping scapula syndrome. Orthop Rev. 1993;22:1141-4. 34. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy. 2003;19:641-61. 60. Percy EC, Birbrager D, Pitt MJ. Snapping scapula: a review of the literature and presentation of 14 patients. Can J Surg. 1988;31:248-50. 35. Kuhn JE, Plancher KD, Hawkins RJ. Symptomatic scapulothoracic crepitus and bursitis. J Am Acad Orthop Surg. 1998;6:267-73. 36. Higuchi T, Ogose A, Hotta T, Okamoto K, Kamura T, Sasai K, Hatano H, Morita T. Clinical and imaging features of distended scapulothoracic bursitis: spontaneously regressed pseudotumoral lesion. J Comput Assist Tomogr. 2004;28:223-8. 61. Cameron HU. Snapping scapulae: a report of three cases. Eur J Rheumatol Inflamm. 1984;7:66-7. 62. Arntz CT, Matsen FA 3rd. Partial scapulectomy for disabling scapulo-thoracic snapping. Orthop Trans. 1990;14:252-3. 63. Bell SN, van Riet RP. Safe zone for arthroscopic resection of the superomedial scapular border in the treatment of snapping scapula syndrome. J Shoulder Elbow Surg. 2008;17:647-9.