Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
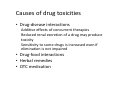
Managing toxicity, side effects and adherence. Maren Koros CHIVA 2015 Definitions • What are side effects? • Side effects Side effects are unwanted symptoms caused by medical treatment. • Can a side effect be therapeutic? Yes It’s an effect, whether therapeutic or adverse, that is secondary to the one intended. Adverse drug reaction. An injury caused by taking medication. Classification based upon dose dependence and predictability – Type A and Type B • Type A - augmentation of the active pharmacologic properties of the drug. Generally less severe and more frequent than Type B reactions. • Type B- the are often unexpected, these can range in severity from nuisance to life threatening. They are usually idiosyncratic. – make many patients unwilling to take drugs on a regular basis, and this lack of compliance represents a major practical limitation of pharmacotherapy. • Adverse drug reactions may be more likely in patients with pre-existing conditions, such as liver or kidney dysfunction, depressed immune function, or pregnancy Minimising Harm • Drug chosen to treat a particular condition should minimise the patient’s susceptibility to adverse effects and where co-morbidities exist have minimal detrimental effects in the patient’s other diseases and treatment. To achieve this, contra-indications, cautions and side-effects, interactions of the drugs should be reviewed regularly. Drug toxicity • Degree to which a drug can cause harm to an individual. These can occur at many different time scales. • Acute toxicity – can occur as a result of a single exposure and within minutes to hours of the exposure • Chronic toxicity – occurs over a prolonged period of time. Case Presentation • 16 year old young man has been on Truvada efavirenz for 7 years. • Weight 70 kgs • Very Compliant, • VL- BDL • FBCs and U&Es unremarkable. • Complaining of sleep disturbances, He is wondering if she can change medication….. What would you do • A. Nothing • B. Encourage him to consider sleep medication • C. Take time to consider medication. • D. Change medication. What would you change to and why • Decision is made to change to Raletegravir 400mg BD. • Review within 8 weeks. • Week 6 – patient develops ear infection sees GP – prescribed Flumetasone/Clioquinol Ear Drops solution bd for 7 days • On day 5 patient develops rash on ear and side of face so stops using ear drops. Cont’d • 2 weeks later the rash is generally widespread, (8 week appt). What do you do? • All treatment withheld. • In the evening, patient attends ED – Temperature, rigors, widespread rash, red angry, some skin peeling – admitted to general ward. Diagnosis cellulitis - Gen med ward for 5 days treated with I.V. flucloxacillin. - Then discharged. • All parameters return to baseline. • What ARVs would you restart? Cont • Truvada + Raltegravir restarted. • 1 week post re-challenge – patient is admitted via ED, - rash skin, peeling, pyrexia. • 24 hrs later blistering occurs in the mouth and lips and skin condition worsens. • Diagnosis SJS/TENS • Patient is admitted to ITU –turbulent recovery requiring skin grafting. • What would you have done different. Microsoft Word Document Causes of drug toxicities • Drug-disease interactions Additive effects of concurrent therapies Reduced renal excretion of a drug may produce toxicity Sensitivity to some drugs is increased even if elimination is not impaired • Drug-food interactions • Herbal remedies • OTC medication Management and prevention • In children who have severe or life-threatening toxicity, all antiretroviral drugs should be stopped immediately. Once symptoms of toxicity have resolved, antiretroviral therapy should be resumed with substitution of a different antiretroviral drug or drugs for the offending agent(s) • When modifying therapy because of toxicity or intolerance to a specific drug in children with virologic suppression, changing one drug in a multidrug regimen is permissible; if possible, an agent with a different toxicity and side-effect profile should be chosen . • The toxicity and the medication presumed responsible should be documented in the medical record and the caregiver and patient advised of the drug-related toxicity. • Dose reduction is not a recommended option for management of ARV toxicity, except for those few antiretroviral drugs for which a therapeutic range of plasma concentrations detected by therapeutic drug monitoring correlates with toxicity . Manamement • Identification and management of Side effects/ Toxicity can be complex and usually requires a multi disciplinary approach. • More importantly requires patient education to alert them SE which are serious and what to do about these reactions. • Traffic light system (or an app) can be used to create a selection of SE and whom to report to and discuss when these occur. Reporting • The MHRA recommends that all ADRs that are serious, medically significant, or results in harm should be reported. • https://yellowcard.mhra.gov.uk/ • Patients and healthcare workers can report • Associated with newer drugs and vaccines ( black triangle) should be reported. References • http://www.nhs.uk/chq/pages/997.aspx?cate goryid=73&subcategoryid=108 • (https://www.blackwellpublishing.com/content/BPL_Images/ Content_store/Sample_chapter/0632045868/cobertsample.p dfunpredictable or idiosyncratic.) • http://downloads.lww.com/wolterskluwer_vit alstream_com/samplecontent/9780781783552_Golan/samples/929 00_CH5.pdf • Fauci, Anthony S., et al. Harrison's Principles of Internal Medicine. 17th ed. United States: McGraw-Hill Professional, 2008 • BNF C • BNF • https://aidsinfo.nih.gov/guidelines/html/2/pe diatric-arv-guidelines/368/overview