Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sumy State University
Internal Medicine Department
Methodological Instructions
for the 4th course students, 8 semester
Module 2
“Pulmonology, Haematology”
Prepared by Orlovsky A. V., assistant, D.Ph,
Murenets N. A., postgraduate
Sumy - 2009
Methodological Instruction to Lesson № 1.
Propedeutics in pulmonology.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
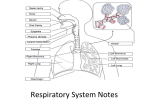
1. Structure of the bronchial tree.
2. Determination of the lungs border.
3. Structure of the respiratory segment (part) of the lung.
4. Comparative percussion of the lungs.
5. Blood supply of the lung.
6. Cough, its characteristics.
7. Structure of the bronchial mucous. Concept of bronchial clearance.
8. Rales and their characteristics.
9. Physiology of respiration.
10.What is vocal fremites and method of its indication?
11.Show the spirogram schematically. What is the purpose of the spirogram?
12.Name kinds of dispnoea.
13.What is forced expiration volume in 1 second (FEV1), forced vital capacity
(FVC)?
14.Comparative percussion of the lungs.
15.What is this pneumotachometry?
16.Name main symptoms of respiratory diseases.
17.Name main groups of drugs in patients with respiratory diseases.
References.
1. Propedeutics to Internal medicine Part 1 Diagnostics/O. M.
Kovalyova, T. V. Ashcheulova. – Vinnytsya. – 2006. – P.60 - 138.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002.
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 2.
Chronic obstructive pulmonary disease (COPD).
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. Give the definition of COPD.
2. Etyology of COPD. Give external and internal risk factors of COPD.
3. Pathogenesis of COPD. What reflects airflow limitation.
4. Pathology of COPD.
5. Clinical symptoms of COPD.
6. Name co-morbidities in patients with COPD.
7. Physical findings of patients with COPD.
8. X-Ray findings of patients with COPD.
9. Studing of external respiration functions. Spyrometry.
10.Clinical and functional monitoring.
11.Give the classification of COPD.
12.Name main treatment principles of patients with COPD.
13.Name drug, which are used in treatment of patients with COPD.
14.Name the phaemacotherapy for patienta with COPD depending on the level
of gravity of the disease.
15.Role of glucocorticosteroids in treatment of patients with COPD.
16.Name the other pharmacological treatment of patients with COPD.
17.Rehabilitation of patients with COPD.
18.Name the reasons exacerbations of COPD.
19.Algorithm of managing exacerbation of COPD in the outpatient setting.
20.Name the indications for hospitalisation in case of exacerbation of COPD.
21.Name the indications to antibacterial therapy. What is influenced on
choosing antibacterial therapy.
22.Name antibacterial therapy of patients with COPD.
Examples of tests
1.
What is the most important cause of COPD?
a. exposure to dusty or polluted air
b. alpha1- antitrypsin deficiency
c. cigarette smoking
d. familial predisposition
e. low birth weight
2. Chronic cough, which characterised COPD, is:
a. cough precedes dyspnea
b. cough is parallel to dyspnea
c. cough after marked dyspnea
d. there are no defined law
e. cough may be absent
3. Inhalation β2- agonists of short – term action are the following drugs, except:
a. Salbutamol
b.
c.
Fenoterol
Terbutalin
d. Salmeterol
4. The main symptoms of the COPD are:
a. abdominal pain and diarrhea,vomiting
b. cough
c. headache
d. constipation
e. sneezing
5. Differential diagnosis of the COPD with:
a. Asthma
b. Peritonitis
c. Piothorax
d .appendicitis
e.myocardial infarction
6. The Symptoms and Signs of the COPD are:
A. constipation
B. bloody vomiting
C. frequent headache
D. chronic cough and sputum production
E. sneezing
Answers to the self-assessment:
1-c, 2-a, 3-d, 4-b, 5-a, 6-d
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 27 - 37 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002. – 508-513 p.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 10, section 2, Chapter 254.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Chronic obstructive pulmonary disease is the internationally preferred term encompassing
chronic bronchitis and emphysema.
By definition COPD is a chronic, slowly progressive disorder characterised by airflow
obstruction (FEV1 < 80% predicted and FEV1/VC ratio <70%) which does not change markedly over
several months. The impairment of lung function is largely fixed but may be partially reversible by
bronchodilator therapy.
Historically, the term 'chronic ronchitis' was used to define any patient who coughed up sputum
on most days of at least 3 consecutive months for more than 2 successive years (provided other causes
of cough had been excluded) and 'emphysema' referred to the pathological process of a permanent
destructive enlargement of the airspaces distal to the terminal bronchioles. Although 'pure' forms of
these two conditions do exist, there is considerable overlap in the vast majority of patients.
The death rate from COPD currently exceeds 25 000/year (> 20-fold higher than asthma) in
England and Wales and this condition accounts for over 10% of all hospital medical dmissions in the
United Kingdom.
Etiology
The single most important cause of COPD is cigarette smoking although in developing countries
exposure to smoke from biomass and solid fuel fires is also important. Smoking is thought to have its
effect by inducing persistent airway inflammation and causing a direct imbalance in
oxidant/antioxidant capacity and proteinase/antiproteinase load in the lungs. Individual susceptibility
to smoking is, however, very wide, with only 15% of smokers likely to develop clinically significant
COPD.
Recent studies have also emphasised the strong familial risks associated with the development of
COPD. A small additional contribution to the severity of COPD has been reported in patients exposed
to dusty or polluted air.
An association also exists between low birth weight, bronchial hyper-responsiveness and the
development of COPD.
Alpha1-antitrypsin deficiency can cause emphysema in non-smokers but this risk is increased
dramatically in enzyme-deficient patients who smoke.
Stopping smoking slows the average rate of the decline in FEV1 from 50-70 ml/year to 30
ml/year (i.e. equal to non-smokers). Interestingly, there is no evidence that acute exacerbations or drug
therapy affect the rate of decline of the FEV1.
Pathology
The pathologic findings include hypoplasia and hypertrophy of the submucosal bronchial
mucous glands, hyperplasia of bronchiolar goblet cells, squamous metaplasia of bronchial mucosal
cells, chronic and acute inflammatory infiltrates in the bronchial submucosa, profuse inflammatory
exudates in the lumens of bronchi and bronchioles, and denudation of bronchial mucosa.
Airflow limitation reflects both mechanical obstruction in the small airways and loss of
pulmonary elastic recoil. Loss of alveolar attachments around such airways makes them more liable to
collapse during expiration.
Clinical Findings
Initially, cough with sputum production, often in the morning, may be the only symptom.
Gradually the cough and sputum production increase and symptoms of dyspnea on exertion develop.
As the disease progresses, the patient's course is usually marked by recurrent episodes of acute
respiratory failure resulting from infectious exacerbations of the bronchitis. Clinically, these are
marked by increased cough, change in sputum from clear and mucoid to purulent, fever, dyspnea, and
varying degrees of respiratory distress. Respiratory failure often ensues, with both elevated PaCO2 and
diminished PaO2. These episodes are often reversible at first with appropriate antibiotics,
bronchodilators, and respiratory therapy.
Signs and symptoms of cor pulmonale are frequent in chronic bronchitis and are exacerbated
along with episodes of acute respiratory failure.
The course of the disease is one of gradual increase in frequency and severity of episodes of acute
infection and respiratory failure, eventually resulting in intubation and the need for almost constant
ventilatory assistance. Death usually occurs during an episode of respiratory failure.
Depending on the stage in which the patient is examined, the physical findings may vary. During
relatively quiescent periods, the only finding may be increased anteroposterior diameter of the chest,
hyperresonance to percussion, prolonged expiratory phase, rales, mainly low and medium-pitched, are
audible in most patients, and wheezing. Later, the patient may manifest the signs and symptoms of
pulmonary hypertension and right ventricular failure, ie, increased second heart sound, pedal edema,
hepatomegaly, and ascites. These patients commonly have a plethoric appearance resulting from
secondary polycythemia.
If examined during an acute attack, the patient will be in respiratory distress, as evidenced by
tachypnea and use of accessory muscles of respiration, in addition to the signs described above. Cough
is often prominent, and cyanosis during acute attacks is not uncommon.
X-Ray Findings
Chest x-rays show evidence of pulmonary overinflation, with increased anteropostenor diameter,
flattened diaphragms, and increased retrosternal air space. There are often prominent and increased
bronchial markings at the lung bases, seen as parallel or tapering shadows ("tram lines"), which reflect
the increased thickness of the bronchial wall. Bullae of varying sizes may be seen primarily in the
upper lung fields rather than the lung bases.
Studying of external respiration functions
Spirometry is obligatory when diagnosing COPD. It’s also necessary for estimating the level of
gravity and for periodical monitoring to assess disease progression.
For patients with mild and moderate COPD slight decrease of both forced expiration volume
during the first second (FEV1) and forced vital capacity of the lungs (FVCL) is characteristic. The
value of FEV1 after introducing bronchial spasmolytic < 80% on the background of the ratio
FEV1/FVCL < 70% proves the presence of limitation of respiratory tracts which is not fully reversible.
If there is no possibility for a spirometric research, then forced expiration lasting more than 6 seconds
is a rough but useful decrease detection-predictor of the ratio FEV1/FVCL < 50%.
With disease progression bronchial obstruction grows, total bronchial resistance (Rtot) rises,
expiratory lungs hyperinflation appears and increases, air traps develop in the lungs, which results
from resilient lung return loss and respiratory tracts collapse, the structure of total lung capacity (TLC)
is redistributed. In order to give an integrated assessment of these indices it’s necessary to carry out a
more profound and informative research – total bodyplethysmography. In difficult diagnostic cases
diffuse capacity of the lungs, which reveals gas exchange disturbances, is measured to make a decision
concerning operative intervention.
To carry out the monitoring of COPD progression, to assess the efficacy of prescribed medicines
in certain patients annual spirometry is carried out. Thus, in healthy people annual decrease of FEV 1 is
< 30ml, in patients with COPD it’s 30-60ml and more.
Arterial blood gases measuring is carried out in patients with FEV1 < 40% of the due, or if
clinical presentations of lung insufficiency, right heart portions insufficiency are observed.
Clinical and functional monitoring
Frequency of visits to a doctor depends on the gravity of COPD and grows with increase of
disease gravity. Visits can be planned and unplanned (e.g. if the state worsens or undesirable therapy
manifestations, exacerbations are observed, etc.). During every visit noxious agents influence, the
status of smoking are estimated; also disease progression and appearance of aftereffects; efficacy of
earlier prescribed medicines is assessed, if necessary – medication dosing is changed, undesirable
therapy manifestations are detected; anamnesis of exacerbation is studied (frequency, gravity are
estimated, the causative agent is identified, if possible); also concomitant pathology; compliance of the
sick man and skills in handling inhaler are checked. Spirometric examination is carried out
periodically (usually once a year or when significant aggravation of symptoms or complications are
observed).
Classification of COPD.
There are 4 stages of COPD according to the levels of gravity of the disease which are singled
out after results of examination of the patient during clinically stable period in case there is no
exacerbation. Intensity of clinical signs of the disease and of functional characteristics of
broncoobstructive syndrome are taken into consideration. COPD stage (levels of gravity) signs
Stage and level Signs of COPD
of gravity of COPD
1. mild
2. moderate
- FEV1/FVCL < 70%
- FEV1 ≥ 80% of the due
- usually but not always chronic cough, expectorations
- FEV1/FVCL < 70%
- 50% ≤ FEV1 < 80% of the due
- Symptoms are aggravating, exertional dyspnea and dyspnea after complications
appear
3. severe
- FEV1/FVCL < 70%
- 30% ≤ FEV1 < 80% of the due
- Dyspnea intensifies, repeated exacerbations, which worsen patients’ lives
4. very severe
- FEV1/FVCL < 70%*, FEV1 < 30% of the due, or FEV1 < 30% of the due in the
presence of chronic lung insufficiency
- Further aggravation of symptoms, life quality is considerably worsened,
exacerbations may threaten life
Notice.
*In case of very severe COPD and significant decrease of FVCL ratio FEV1/FVCL increases and
loses diagnostic value.
Treatment of patient with COPD
Main treatment principles of patients with COPD are: gradual treatment intensity grows
depending on the gravity level of the disease; regularity, constancy of basic therapy corresponding to
the gravity level of the disease; variability of individual drug response denotes the necessity of
attentive and regular monitoring of clinicofunctional characteristics of the disease.
When treating COPD, preference is given to inhalation way of introducing medicines – bronchial
spasmolytics, inhalation corticosteroids, combined medicines. Efficacy of this route of administration
depends significantly on the patient’s mastering inhalation technique. When indicating high
medication dosing and to improve inhalation technique it’s recommended to use spacers of big
volume. Usage of nebuliser gives the opportunity to take high doses of medicines and to get
therapeutic responses in short periods of time and at the same time to supply oxygen to the circuit (if
necessary).
Bronchial spasmolytics improve patency of airways, improve emptying of lungs, reducing
hyperinflation, ameliorate physical endurance; play the main role in the symptomatic treatment of
patients with COPD. They are prescribed both as basic therapy and to remove some acute symptoms;
inhalation forms of bronchial spasmolytics are of higher value.
Inhalation ß2-agonists of short-term action (salbutamol, fenoterol) have comparatively fast
beginning of broncholytic action, which depends on the dosing and lasts for 4-6 hours.
Inhalation ß2- agonists of prolonged action (salmeterol, formoterol fumarat) cause stronger
and more stable effect during 12 hours and more, and have some anti-inflammatory action.
Inhalation cholinergic antagonists of short-term action (ipratropium bromid) are
characterized by dosing-depending effect with slower beginning and action lasting longer than that of
ß2- agonists of short-term action.
Inhalation cholinergic antagonists of long-term action (tiotropium bromid) cause stable
significantly stronger broncholytic action than ipratropium, lasting for 24 hours and longer, have some
anti-inflammatory action.
Protracted usage of bronchial spasmolytics of prolonged action (ß2-agonist or cholinergic
antagonist) or their combination depending on COPD gravity; positively influences respiratory
function (improves patency of airways, reduces hyperinflation of the lungs, optimizes the structure of
total lung capacity); significantly reduces dyspnea – especially aggravating symptom in patients with
COPD; increases exercise tolerance; improves patients’ health in general and their quality of living;
decreases the quantity of exacerbations and cases of hospitalization.
Thus, regular treatment with inhalation bronchial spasmolytics of prolonged action is more
effective and convenient than therapy with bronchial spasmolytics of short-term action, but it’s more
costly.
Xanthines have small broncholytic action and are potentially toxic.
At the same time besides possible additional bronchodilation Xanthines cause some antiinflammatory action, increase respiratory muscle strength. Xanthines are bronchial spasmolytics of the
second choice and may be added to earlier prescribed bronchial spasmolytics of the first choice (ß 2agonists and/or cholinergic antagonists) in cases of severe and very severe COPD in order to increase
therapeutic efficacy.
Glucocorticosteroids. The role of GCS in cases of COPD is less marked than in bronchial
asthma. In the basic therapy of COPD inhalation GCS are prescribed according to specific indications.
Oral GCSs are recommended only in cases of COPD exacerbation.
Protracted administration of oral GCS in the basic therapy is not recommended regarding the
absence of obvious advantage, undesirable systemic consequences and side action of such therapy
(steroid myopathy, muscle weakness, deterioration of functional abilities, lung insufficiency…).
Inhalation GCSs are prescribed in long basic therapy for COPD (in patients at the 3rd, 4th stages
of the disease, when FEV1 < 50% of the due, often exacerbations taking place 3 times or more for the
past 3 years). At the same time the frequency of acute exacerbations and cases of hospitalization
decrease, general level of health and living quality of the patients improve, death rate caused by all
reasons in case of COPD reduces.
Combination of inhalation GCS and ß2- agonists of the prolonged action is more effective than
each component apart.
The chart of pharmacotherapy for patients with COLD depending on the level of gravity of
the disease.
mild
1 stage. 2 stage.
3 stage.
4 stage. very severe
moderate
severe
Avoid risk factors, stop smoking, influenza virus vaccine
Bronchial spasmolytics of short-term action should be prescribed
1 or 2 bronchial spasmolytics of prolonged action should be added according to
plan + rehabilitation
GCS inhalation, by frequent exacerbations, must be included
In case of chronic lung insufficiency (CLI) O2therapy must be added. The possibility of operative
intervention should be regarded.
Other pharmacological treatment: anti-inflammatory medicines of nonsteroid action (fenspirid
hydrochlorude) are prescribed by moderate exacerbation and are included into basic therapy during 25- months after COPD exacerbation. Influenza virus vaccine can decrease severity of the exacerbation
and reduce death rate among people with COPD.
Antioxidants: acetilcystein reduces the quantity of exacerbations. It’s recommended to prescribe
it to patients with frequent exacerbations, history of long-term smoking.
Antibiotics are indicatede in case of the proved infectious exacerbation of COPD.
Rehabilitation of patient with COPD
Rehabilitation must be prolonged, including physical training, consultations as for nourishment,
teaching and support of sick people.
Oxygenotherapy. Decision on the necessity of oxygenotherapy for patients with COPD is made
after taking into consideration disease gravity level, clinic symptoms manifestation, adequacy and
efficacy of basic therapy, level of lung insufficiency and of blood oxygen balance.
Surgical treatment. Bullectomy, if there are emphysematous bullae causes decrease of dyspnea
and improvement of external respiration function (ERF). Before operative intervention it’s necessary
to study ERF, gas exchange and come to a conclusion as for its indication and safety.
Exacerbation of COPD
Exacerbations of COPD are divided into infectious and noninfectious. Most exacerbations are
provoked by infectious agents, environmental pollution growth, inappropriate basic therapy,
oxygenotherapy.
Algorithm of managing exacerbation in the outpatient setting
- to initiate or intensify broncholytic therapy (bigger dosing and more often administration,
combination of different bronchial spasmolytics (ß2-agonists, cholinergic antagonists), usage of
nebuliser or spacer;
- prescribing antibiotics in case of infectious exacerbation;
- repeated estimation of the patient’s condition;
- if symptoms and signs of exacerbation are improving prescribed treatment must be continued, after
exacerbation is gone basic treatment must be revised;
- if symptomatic improving is not observed then oral GCS (30-40mg prednisolone during 10 days)
must be introduced;
- repeated estimation of the patient’s condition;
- if the patient’s condition is better, when exacerbation is gone basic treatment must be revised;
- if symptoms and signs of exacerbation are worsening the patient must be taken to a hospital.
Indications for hospitalisation in case exacerbation of COPD
-
considerable worsening of symptoms intensity (e. g. sudden onset of dyspnea at rest);
complicated clinical course without exacerbation;
presence of new physical signs (cyanosis, peripheral oedemata);
feeble response to initial treatment for exacerbation;
marked concomitant diseases;
onset of arrhythmia bouts;
worsening of consciousness;
uncertain diagnostics, lack of possibility to verify the diagnosis reliably;
elderly age;
unfavourable living conditions.
It’s first of all pus increase in sputum that indicates infectious exacerbation. Also dyspnea
intensifies and sputum amount grows.
Choosing antibacterial therapy it’s necessary to take into consideration such criteria as the age of
the patient, exacerbation frequency for the last year, presence of concomitant pathology and level of
FEV1 value.
In patients younger than 65 with COPD frequency less than 4 times a year, without concomitant
diseases and FEV1 more than 50% of the proper value the main causative agents are H. influenzae,
S. pneumoniae, M. catarrhalis and atypical microorganisms. As the antibiotic of choice
aminopenicillin (amoxicillin) or macrolide is recommended, or respiratory fluoroquinolone for oral
administration which is prescribed when ß-lactams and macrolides are not effective, or there is allergic
response.
In patients olderer than 65 with COPD frequency 4 times a year or more, with concomitant
diseases and FEV1 ranging from 30 to 50% of the proper value the main causative agents are H.
influenzae, representatives of Enterobacteriaceae, and also S. pneumoniae. That’s why as the medicine
of choice protected aminopenicillin or cephalosporin of the second generation, or respiratory
fluoroquinolone for oral administration is recommended.
When FEV1 is less than 30% of the proper value, antibacterial therapy is often (more than 4
times a year) and it’s necessary to take corticosteroids constantly, the reason of COPD exacerbation
may be P. aeruginosea. Hence parenteral administration of fluoroquinolone of the second generation
(ciprofloxacin) or respiratory fluoroquinolone of laevofloxacin – in high dosing, or ß-lactam with anti
blue pus action in combination with aminoglycoside is recommended.
Regardless the fact that COPD is a progressing disease correctly chosen and therapy prescribed
in time and rehabilitation can significantly slow down broncoobstructive progression, reduce
frequency and gravity of exacerbations, prevent development of exacerbation and systemic aftereffect,
improve level of life.
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 3.
Bronchial Asthma.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. Give the definition of bronchial asthma.
2. Name essential of diagnosis.
3. Name clinical symptoms of bronchial asthma.
4. What induces development the symptoms of bronchial asthma.
5. What characterizes the acute attack of bronchial asthma?
6. Name the criteria of respiratory function violence.
7. Give the clinical picture of classic allergic (atopic) bronchial asthma.
8. How is the studying of bronchi hyperreactivity carried out?
9. List the diagnostic tests, which are made at ambulatory-polyclinic stage.
10.Give the classification of bronchial asthma.
11.What is intermitting bronchial asthma?
12. What is mild persistent bronchial asthma?
13. What is permanent bronchial asthma of moderate severity?
14. What is severe permanent bronchial asthma?
15. For what purpose is conception “bronchial asthma control” introduced?
16. What is controlled course of bronchial asthma?
17. What is partially controlled course of bronchial asthma?
18. What is non-controlled course of bronchial asthma?
19. Laboratory findings in patient of bronchial asthma.
20. X-Ray findings in patient of bronchial asthma.
21.Name ways of medications introductions which use in treatment of patients
with bronchial asthma.
22.Which is the main way of medications introductions which use in treatment
of patients with bronchial asthma?
23.Name controlling medicines.
24.When can we prescribe glucocorticosteroids of system action?
25.Name glucocorticosteroids of system action.
26.How will we decrease the dosage of prednisolon?
27.Name inhalation glucocorticosteroids.
28.Name side effects of system and inhalation glucocorticosteroids.
29.Name preventive measures of inhalation glucocorticosteroids side effects.
30.What can you say about steps 1, 2, 3, 4 in treatment of patients with
bronchial asthma?
31.What is steroid-sparring therapy?
32.Name steps for achievement and keeping up the control of bronchial asthma.
33.What can you say about cromons, methylxantines, leucotrien-modificator?
34.What can you say about β2-agonists of prolonged action and short-term
action?
35.What can you say about symptomatic therapy?
36.What will you do if control of the disease is achieved for a period of 3
months?
37.What is the duration of controlling theropy?
38.What is bronchial asthma exacerbation and it stages?
39.Where may be treated patients with mild and moderate severity and severe
bronchial asthma?
40.Name treatment the ambulatory stage.
41.What is complete response on therapy?
42.What will you do if the patient gives non-complete response?
43.Name treatment of patients with severe exacerbation of bronchial asthma.
Examples of tests
1.
A.
B.
C.
D.
E.
2.
A.
B.
C.
D.
E.
3.
A.
B.
C.
D.
E.
Clinical symptoms of bronchial asthma are usually connected with spread but various
bronchiobstruction which is:
partially reversible by bronchodilator therapy
the impairment of lung function is largely fixed
reversible spontaneously or under treatment
non-reversible under treatment
non-reversible spontaneously
Clinical symptoms of bronchial asthma are, except:
cough with purulent sputum
episodic breathlessness with laboured exhalation
cough with expectoration of tenacious mucoid sputum more at night and physical loading
episodic wheezes in lungs
repeated chest constraint
Laboratory findings are characterized by, except:
sputum is characteristically tenacious and mucoid
sputum is characteristically purulent
sputum contains "plugs" and "spirals"
eosinophils are seen microscopically
arterial hypoxemia may be present
Answers to the self-assessment:
1- c, 2-a, 3-b
1. Real-life situation:
Patient K., 42 years old, was admitted to the hospital with complaints on bad cough, breath insufficiency,
pain in the right lower part of ribcage that increases while deep breathing. It is known from anamnesis
that K. has been working in coal industry for 26 years. Chronic pneumonia was diagnosed in this patient 5
years ago. What methods of examination can prove the absence of pleurisy in this patient?
Answer. X-ray examination
2.Patient 17 years old, complain of сough, recurrent attacks of dyspnea, t – 37.0-37.2C. Beginning of
disease she ties to pneumonia (three years ago). In childhood often had respiratory infection diseases,
such us bronchitis, pneumonia. In lungs- musical rales, in blood- eosinophillia. X-ray Findings: Chest
films show no abnormalities. What disease has this patient?
.
Answer: Bronchial asthma
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 41 - 60 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002. – 513-521 p.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 10, section 2, Chapter 240.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Bronchial asthma (BA) – chronic inflammatory disease of upper respiratory tracts,
caused by considerable amount of inflammatory cells and mediators. Chronic inflammation
combines with bronchi hyperreactiveness what show up in relapsing symptoms of whistling
breathing, breathlessness, chest constraint, cough, especially at night and in the early morning.
That episodes are usually connected with spread, but variation bronchiobstruction, which is
reversible spontaneously or under treatment.
If a patient has clinical and functional symptoms, the diagnosis of BA will be made BA.
Essentials of Diagnosis:
1. Recurrent acute attacks of dyspnea, cough, and mucoid sputum, usually accompanied by
wheezing.
2. Prolonged expiration with generalized wheezing and musical rales.
3. Bronchial obstruction reversible by drugs.
Clinical symptoms:
episodic breathlessness with laboured exhalation.
cough with expectoration of tenacious mucoid sputum more at night and physical loading.
episodic wheezes in lungs.
repeated chest constraint
Symptoms are especially severe at night and in the morning and awake a patient; develop
or become worse at: physical loading, viral infection, antigens influence, smoking, external
temperature overfall, aerosols action, intake of some medicines (nonsteroidal anti-inflammatory
drugs, β-blockers).
Circadian and circannual (seasonal) symptoms variation is characteristic.
Classic allergic (atopic) asthma usually begins in childhood and becomes progressively
more severe throughout life, although spontaneous remissions may occur in adulthood. Hay
fever often accompanies atopic asthma.
The acute attack is characterized by dyspnea usually associated with expiratory wheezing
that may be heard without a stethoscope. Cough may be present but is usually not the
predominant symptom. There is a small group of patients with asthma in whom paroxysmal
cough may be the predominant symptom.
When asthtna becomes prolonged, with severe intractable wheezing, it is known as status
asthmaticus.
-
Criteria of respiratory function violence.
- decrease of peak volume in 1 second (FEV 1.0) 80% of proper.
- expressed reversibility of bronchial obstruction – increasing of PVES and FEV 1.0 12% (or
200 ml) by results of pharmacological test with short action β-agonist.
- daily variation PVES and FEV 1.0 20%.
Medical aid at ambulatory – polyclinic stage list and volume.
Diagnostic tests:
1. External breathing function (EBF), (PVES and FEV 1.0)
2. Allergologic tests (allergologic anamnesis – allergic rhinitis, atopic dermatitis presence at
patient or BA or atopic diseases at his family members; positive skin tests with allergens
general and specific 1gE level increasing.
3. Studying of bronchi hyperreactivity is carried out at patients with clinical symptoms,
which are characteristic for BA but at absence of characteristic EBF violations; is
estimated by results of provocative tests with histamines metacholine, physical loading.
Classification
BA is classified by rate of course severity by complex analysis of bronchi obstruction
clinical and functional symptoms. Answer on treatment in the period between attacks. Functional
indexes changes estimation for disease severity determination is conducted in period without
expiratory breathlessness episodes. BA classification according to rate of severity is especially
important at solution of a question of disease management at patient’s condition primary
examination
Intermitting (episodic), persistent (permanent stable) (mild, moderate severity, severe)
course are distinguished.
Intermitting BA: symptoms (episodes of cough whistling breathing, breathlessness) are
transitory, arise rarely than 1 time a week during at least 3 months; exacerbations of short
duration, night symptoms arise not more frequently than 2 times a month. Between exacerbations
symptoms are absent, normal indexes of EBF: PVES or FEV 1.0 ≥80% of proper; daily variation
PVES and FEV < 20%.
Mild persistent BA: symptoms arise at least 1 time a week, but more rarely than 1 time a
day during more than 3 months. Symptoms of exacerbation may disturb activity and sleep;
presence of chronic symptoms, which requires symptomatic treatment almost every day; night
asthma symptoms arise more than 2 times a month, PVES or FEV 1.0 ≥ 80% of proper; daily
variation of PVES or FEV 1.0 20-30%.
Permanent BA of moderate severity: everyday symptoms; exacerbations disturb activity
and sleep; night symptoms of asthma arise more than 1 time a week; necessity of short action β2
agonists every day intake, PVES or FEV 1.0 >30%.
Severe permanent BA: presence of variable to a considerable extent, prolonged
symptoms; frequent night symptoms, limiting of activity, severe exacerbations in spite of
treatment, which is conducted, proper decease control is absent: prolonged, daily symptoms are
constantly present; frequently night symptoms, frequently severe exacerbations; conditioned by
BA limiting of physical activity. PVES or FEV 1.0 <60% of proper; PVES or FEV 1.0 daily
variation >30%. Achievement of the BA control may be impossible.
For the purpose of determination of the possible best results of treatment, answer the
questions how the patient must react on prescribed treatment, conception “BA control” is
introduced.
They distinguish: controlled course absence or minimal (≤ 2 times a week) daily
symptoms, absence of activity limiting, night symptoms, absence or minimal (≤2/week)
necessity in bronchial spasmolytic to relieve symptoms, normal PVES index, exacerbations
absence;
Partly control (any symptom may occur in any week) non controlled course (≥3 symptoms
of partly control are present at any week);
Control lever and extend of treatment at the present moment determinate the choice of
proper tactic of further treatment.
.
Laboratory Findings:
The sputum is characteristically tenacious and mucoid, containing "plugs" and "spirals."
Eosinophils are seen microscopically. The differential blood count may show eosinophilia. In
severe, acute bronchospasm, arterial hypoxemia may be present as a result of disturbed perfusion
/ventilation relationships, alveolar hypoventilation, or functional right-to-left shunts.
X-Ray Findings: Chest films usually show no abnormalities. Reversible hyperexpansion
may occur in severe paroxysms, or hyperexpansion may persist in long-standing cases.
Transient, migratory pulmonary infiltrations may be present. Severe attacks are sometimes
complicated by pneumothorax.
Pharmacotherapy of patients with BA.
BA patients medical treatment is conducted with use of different ways of medicines
introductions: inhalation, oral, parenteral.
Inhalations, which provide expressed local action of medicines in lung don’t cause their
undesirable system action, enable an opportunity to accelerate positive treatment effect using
lesser doses of medicines has the greatest advantages.
Controlling medicines.
Are taking every day, to the basis, for a long term, to achieve and keep up the control of
persistent BA.
Include: inhalation glucocorticosteroids (GCS) (first choice), system GCS, cromones,
leucotriens modificators, prolonged action bronchial spasmolitics (inhalation prolonged action
β2-agonists), oral prolonged action β2-agonists, prolonged action xantines) and system steroid –
sparring therapy.
System action GCS (oral) may be prescribed as basis control therapy at some severe BA
patients but their using must be limited because of risk of considerable side effects development.
Oral GCS long-term therapy is worth prescribing just in cases of non-efficiency of other
methods of BA treatment, including inhalation steroids in high doses in combination with
bronchi spasmolytics of prolonged action and continuing just then, when relieving of clinical
symptoms, bronchial obstruction and frequency of severe exacerbations occurring is a success.
Short action medicines (prednisolone, methilprednisolone) are recommended for intake;
daily supporting dose should be taken in in the morning, and if it is possible should be changed
to intermitting therapy.
It is advisable to take minimal efficient doses of system GCS, and if it is possible to
decrease their dose or to stop taking them, pass to high doses of inhalation GCS (2000 mkg/day),
combination of the last and prolonged action bronchi spasmolitics.
Cromones may be used as controlling therapy at mild persistent BA, although their effect
is considerably lesser in comparison with taking inhalation GCS.
Xantines have relatively low bronchi spasmolytic effect and risk of side effect if are used
in high doses. Xantines are characterized by some anti-inflammatory action if low doses are
prescribed in prolonged BA treatment.
Prolonged action β2-agonists (salmeterole, formoterole fumaratis) have prolonged
(duration more then 12 hours) bronchi spasmolytic effect and some anti-inflammatory action.
The mentioned medicines are prescribed additionally (instead of inhalation GCS doses
increasing), when basis therapy with standard doses of inhalation GCS is not enough to achieve
control of the disease.
Using of combinations (fluticasone propionatis+ salmeteroli, budesonide + formoterole
fumoratis) makes possible achievement of high level control of disease at most moderate
severity, severe persistent BA patients. Fixed combination budesonide + formoterole fumaratis,
in favour of rapid beginning of its action (beginning of the salmeterole’s action – in 4-3 minutes
after inhalation) may be taken “When needed”.
Symptomatic therapy:
“first aid” preparations are used to relieve attacks of acute bronchi spasm and other BA
symptoms: first of all short action β2-agonists (salbutamole sulfatis, fenoterole hydrobromide);
additionally – short action anticholinergic drug (fenoterole hydrobromide + ipratropium
bromide; salbutamole sulfatis + ipratropii bromide).
Stepped method of BA patients pharmacotherapy
Step №1 – Intermitted BA
Treatment – symptomatic when it is needed: inhalation short action β2-agonists when it is
needed (at presence of symptoms) – first choice prophylactic intake before physical loading or
possible allergen influence. Other bronchi spasmolytics:
Inhalation short action anticholinergic drugs, oral β2-agonists of short action, short action
xantines – have more slow beginning and/or higher risk of side effects development.
Step№2 – mild persistent BA.
Treatment – symptomatic plus one controlling preparation: every day regular treatment by
antiinflammatory drugs to achieve control of the BA. Preference is given to inhalation GCS
prescribing in low doses. Daily dose may be prescribed at one intake a day for some of them.
Alternative controlling medicines cromones leucothienes modificators are less efficient in
comparison with inhalation GCS; prolonged action xantines – have mild antiinflammatory effect;
using is connected with considerable side effect.
Step№3 – Moderate severity persistent BA.
Treatment: symptomatic therapy plus one or two controlling medicines.
Everyday regular treatment by antiinflammatory preparations to achieve and keep up
control of BA. Combined taking in of inhalation GCS in low doses and prolonged inhalation β2agonists, as in separate introducing apparitions, so in fixed combinations is recommended.
Fixed combination of inhalations and prolonged inhalation β2-agonist in one medicinal
preparation is usually better (comfortable way of introduction, usually better pharmacological
indexes). It is necessary to remember, that prolonged β2-agonists as a monotherapy, without
inhalation GCS are not prescribed!
Another choice is to prescribe average or high doses of inhalation GCS.
Another choice – combination of inhalation GCS in low doses with leucotriens
modificators or with prolonged action xantines (higher risk of side effects development).
Step№4 – Severe persistent BA
Treatment: symptomatic therapy plus one or more controlling medicines. Combined
intaking of inhalation GCS in average – high daily doses with inhalation prolonged β2-agonists
(it may be in one preparation) has the advantages.
If efficiency is not enough leucohienes modificators and/or prolonged xantines may be
prescribed. If it is necessary at severe non-controlled BA with everyday limiting of activity and
frequent exacerbations oral GCS are prescribed supplementary in minimal doses which allow to
achieve effect.
When high doses of inhalation GCS are prescribed after oral GCS, monitoring of
adrenocortical insufficiency symptoms is necessary.
At severe BA with high 1gE level prescribing of recombinant human anti 1gE antibodies is
effective.
At low GCS clinic-functional effect, their expressed system side effects, absence of effect
of other medicines.
Sparring therapy is prescribed with using of immunesuppressors (methotrexat, cyclosporine
A, preparations of gold).
At that their efficiency is estimated in test course. Although, that treatment has low
effectiveness, and side effects, which may by more severe, in comparison with side effects of
steroids.
Steroid-sparring therapy may be used only if its advantage in BA treatment is proved.
Patient should be informed about risk and advantages of the treatment, and the therapy should be
conducted under observation of specialists, which have experience of such therapy and
monitoring of the patient’s general condition. It is necessary to remember, resistant to treatment
persistent BA may be the precursor of non-diagnosed, dangerous for life diseases (system
vasculitis) which require for proper treatment schemes.
Steps for achievement and keeping up of the control of the BA
Step 1
Step 2
Step3
Asthma-classes
Control of the environment (surrounding)
Short action β2-agonists when it is needed
Controlling
To choose 1
To choose 1
therapy
Inhalation GCS Inhalation GCS
in low doses
in low doses +
prolonged β2agonists
Leucotrienes
modificators
Step 4
Step 5
To add 1 or To add 1 or
more
both
average or high
oral GCS
doses of
(minimal dose)
inhalation GCS +
prolonged β2agonists
leucotrienes
Anti-IgE
modificators
Average or high
doses of
inhalation GCS
Inhalation GCS
prolonged
in low doses +
xantines
leucotrienes
modificators
Inhalation GCS
in low doses +
prolonged
xantines
If control of disease motion is achieved for a period of 3 months, using scheme which
corresponds with the determined at patient control step, it is possible to reduce supporting
therapy, to use treatment of lower step, that allows to determine minimal necessary to keep up
control volume of treatment.
If proper control at clinical symptoms is not achieved using prescribed treatment, you
should use the next higher classification step of the scheme, at first having insured oneself that
patient fulfilled right doctor’s prescription.
It is necessary to inform a patient about early symptoms of BA exacerbation, teach him to
control his condition, to conduct peakflowmetry. To form rules of behavior, which may prevent
undesirable outcomes of their violation.
Treatment efficiency criteria: disease control achievement.
Treatment duration: basic therapy is conducted unceasing.
BA exacerbation
BA exacerbation – episodes of progressive laboured breathing, cough, whistling
breathing, chest constraint, or combination of this symptoms, is characterized by decrease of air
slow at exhalation (PVES, FEV 1.0).
4 stage of exacerbation are distinguished: mild moderate severity, severe and danger of
respiratory standstill. Mild and moderate severity disease may be treated in the out patient
setting.
If the patient gives response on increasing of treatment intensity, there is no necessity in
treatment at emergency department. The patient remains under physician control. Teaching of
the patient is recommending therapy reconsideration. Severe exacerbations potentially are
dangerous for patient’s life, their treatment demands medical monitoring, such patients must be
treated in the hospital.
It is necessary to monitor clinical symptoms, objective sighs, stabilization or returning to
functional index (PVES, FEV 1.0) best for patient.
Initial therapy at ambulatory stage: increase of inhalation β2-agonists dose: 2-4 inhalations
every 20 minutes during the first hour.
After that dose taking into attention patient’s individual response and severity of
exacerbation must be reconsidered.
Intaking of dosed inhalator or using spacer or nebulization
If the patient gives complete response on bronchi spasmolytic therapy (PVES increases
>80% or proper or best for the patient and last to 3-4 hours) it is not needed to introduce other
medicines.
At noncomplete response: to continue inhalation β2-agonists taking 6-10 inhalations every
1-2 hours;
to add oral GCS (0,5-1 mg/kp of prednisolone or equivalent doses of other oral GCS for 24
hours).
Inhalation cholinolitics:
It is possible to take combined form inhalation cholinolitics plus β2-agonists; consult a
doctor)
At low effect:
To continue taking of inhalation β2-agonists – to 10 inhalations (better using spacer) or
complete doses with less then 1 hour interval nebulization; to add inhalation cholinolitics, it is
possible to use combined forms: inhalation cholinolitics + inhalation β2-agonists to add oral
GCS, to take an immediate medical advice, call an ambulance.
Severe exacerbations are dangerous for patient’s life and should be treated at emergency
department
Ininial treatment:
- Oxygenetherapy
- Inhalation β2-agonists of short action constantly during 1 hour (nebulization is
recommended);
- System GCS
Secondary estimation with therapy correction is 1 hour: if exacerbation corresponds to
moderate severe stage:
- Oxygenetherapy
- Inhalation β2-agonists + cholinolitics
- system GCS
Next estimation in 1-2 hours:
At good effect: during 1-2 hours after the last manipulation patient may be discharged.
At home: - to continue treatment by β2-agonists;
- Oral GCS are recommended in most cases;
- Combined inhalators are recommended;
- Teaching of the patient (how to take medicines reconsideration or individual treatment
plan, active medical observation)
At non complete response:
- Oxygenetherapy
- Inhalation β2-agonists + cholinolitics
- system GCS
- Intravenous xantines
- Monitoring of: PVES, O2 saturation in arterial blood (SaO2), Pulse.
If therapy is not effective during 1-2 hours:
Treatment in the intensive care department:
- Oxygenetherapy
- Inhalation β2-agonists + cholinolitics
- intravenous GCS
- Parenteral β2-agonists
- Intravenous xantines
- Intubation and artificial pulmonary ventilation
Prognosis :
Most patients with asthma adjust well to the necessity for continued medical treatment
throughout life Inadequate control or persistent aggravation by unmodified environmental
conditions favors the development of incapacitating or even life threatening complications
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 4.
Pneumonia.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. Give the definition of community-acquired pneumonia.
2. Give the classification of community-acquired pneumonia.
3. Give the main causative agents of community-acquired and nosocomial
pneumonia.
4. Give the pathogenesis of lobar pneumonia.
5. Clinical manifestation of pneumonia.
6. What are the changes of the laboratory induces in pneumonia.
7. Radiological examination of the patient with pneumonia.
8. Characteristic of the first and second group of patients with communityacquired pneumonia.
9. Antibiotic treatment of the first and second group of patients with
community-acquired pneumonia.
10.Characteristic of the third and fourth group of patients with communityacquired pneumonia.
11.Antibiotic treatment of the third and fourth group of patients with
community-acquired pneumonia.
12.Give the classification of pneumonia by gravity.
13.Name small and big criteria’s of severe gravity pneumonia.
14.Give the definition and diagnostic criteria’s of nosocomial pneumonia.
Table of antibacterial drugs.
Drugs
Aminipenicillins
Amoxicillin
Amoxicillin/clavulanic acid
Route of
introduction
orally
i.v.,
orally,
orally
Ampicillin/sulbactam
i.v., i.m.
Cefalosporins of the II generation
Cefamandol
i.v., i.m.
Cefoxitin
i.v., i.m.
Cefuroxim
i.v., i.m.
Cefuroxim axethyl
orally
Cefaclor
orally
Cefalosporins of the III generation
Cefoperazon
i.v., i.m.
Cefotaxim
i.v., i.m.
Ceftriaxon
i.v., i.m.
Dosing regimen
0,5-1 г 8 hourly
1,2 г 8-12 hourly
0,625 г 8 hourly
0,625 г 12 hourly
1,5-3 г 6-8 hourly
1-2 г 6 hourly
1-2 г 4-8 hourly
0,75-1,5 г 8-12 hourly
0,5 г 12 hourly
0,5 г 8 hourly
1-2 г 8-12 hourly
1-2 г 8-12 hourly
1-2 г 24 hourly
Ceftazidim
i.v., i.m.
Cefalosporins of the IV generation
Cefepime
i.v.
Cefpirome
i.v.
Carbapenems
Meropenem
i.v., i.m.
Imipenem/celastatin
i.v.
Monobactams
Aztreonam
i.v., i.m.
Aminoglucozydes
Hentamycin
i.v.
Tombremycin
i.v.
Netylmycin
i.v.
Amicacin
i.v.
Macrolids
Azithromycin
orally
Clarithromycin
orally
Midecamycin
orally
Spiramycin
i.v., orally
Fluoroquinolines ІІ generation
Ciprofloxacin
i.v.,
orally
Ofloxacin
i.v., orally
Fluoroquinolines ІІI generation
Levofloxacin
i.v., orally
Fluoroquinolines ІV generation
Moxifloxacin
orally
Tetraciclin
Doxiciclin
orally
Drugs of other groups
Vankomycin
i.v.
Rifampicin
i.v.,
orally
Clindamycin
i.v., i.m., orally
2 г 8 hourly
2 г 12 hourly
2 г 12 hourly
1 г 8 hourly
0,5 г 6 hourly
2 г 8 hourly
3-5 мг/кг 24 hourly
5 мг/кг 24 hourly
4-6 мг/кг 24 hourly
15 мг/кг 24 hourly
0,5 г 24 hourly 3 days
0,5 г 12 hourly
0,4 г 8 hourly
1 500 000 – 3 000 000 IU 8-12 hourly
0,4 г 12 hourly
0,5 г 12 hourly
0,4 г 12 hourly
0,5 г 12-24 hourly
0,4 г 24 hourly
0,2 г 24 hourly
1 г 12 hourly
0,5 г 12 hourly
0,6-0,9 г 24 hourly
0,45-0,6 6-8 hourly
Real-life situation:
1. The patient 35 years old, had sudden onset, complains on fever, high temperature, headache, dry
cough. He caught a cold during fishing and got all these complains at one moment. At examination:
body temperature 39.9C, hyperemia of the cheeks, a light cyanosis of the lips, the skin is pale,
humid, hurried breathing – 32/min, superficial. The expansion of the right lung is limited, there is
dullness to percussion on the right side, bronchial breathing, moist rales. Heart sounds are weak,
tachycardia- 96/min, rhythmical, blood pressure – 110/60. The others systems without any changes.
Laboratory findings: Le – 17.1, Hb – 120, e – 3.8, ESR- 46 mm/h. The X-ray findings: confluent
consolidation of the lobe. On the 3 day from the onset of disease the patient had haemoptysis.
1. Your diagnosis.
2. What diseases it is necessary to differentiate with?
3. Treatment.
Answer.
1. Left-sided lobar severe community-acquired pneumonia
2. Pyogenic Lung disease
3. Antibiotics (amoxiclav 625 mg x 3 times a day), expectorants, broncholytics
2. A patient, 38 years old, admitted to the clinic with the following complaints: anorexia, general
weakness, weight loss, sweating, cough of pus, sometimes – blood spitting, the sputum brought up is foul
– smelling.
The man fall ill 2 weeks ago, when appeared productive cough, fatigue and fever. During several days
he did not apply to a doctor. His general state became worth to the end of the 1st week, when appeared
general excessive sweating, weakness, the temperature elevated between 390 C in the evening and 37,50 C
in the morning, the cough strengthened.
The patient‘s state was heavy a few days. Two days before the man entered to the clinic he had had a
troublesome cough with a blood-streaked sputum with a putrefactive smell (the amount of sputum was
more than 250 ml), after that his general state improved.
Visual examination: general state is satisfactory, the temperature is 37,60 C. The pulse is 80 per
minute, rhythmical. Respiration is 20 per minute. The heart is without peculiarities.
Questions:
1. What signs of the disease we should reveal with the help of palpation, percussion and auscultation of
the lungs?
2. X-ray findings of the disease?
3. Your diagnosis?
4. Your treatment?
Answers:
1. Palpation data: strengthened vocal fremitus to the right, lower the scapula. Percussion data: dull
percussion sound. Auscultation data: weakened vesicular respiration and moist fine and coarse
bubbling rales in the place of dull sound.
2. X-ray findings: a “basket” symptom.
3. Acute bronchopneumonia complicated with acute abscess of the right lung, recurrent stage (rupture of
the abscess into the bronchi).
4. Intensive antibacterial therapy, detoxication therapy.
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 10 - 17 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002. – 501-508 p.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 10, section 2, Chapter 251.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Pneumonia is an acute infectious – inflammatory lung disease with involvement of all
structural elements of lung tissues, obligatory including alveolars with development of exudation
in them.
Classification
As the setting in which a pneumonia develops has such major implications for the likely
organisms involved and hence dictates the immediate choice of antibiotics, pneumonias are now
classified as:
1.community-acquired pneumonia
2.nasocomial pneumonia
3.aspiration pneumonia
4.pneumonia in immunocompromised patient
By gravity of the disease pneumonia is classified into mild, medium gravity and severe.
Besides depending on severity the following pneumonias are discerned: mild, moderate and
severe. But even now there are no precise criteria as for distinguishing between mild and
moderate pneumonias. As the amount of diagnostic and therapeutic measures for pneumonias of
these stages of severity are almost the same it’s reasonable to unite them in the same group –
moderate pneumonia.
The following definition of severe pneumonia should be used. Severe pneumonia is a
disease of a special form of various etiologies which show themselves through severe
intoxication syndrome, hemodynamic changes, marked respiratory compromise and/or signs of
severe sepsis or septic shock, and is characterized by unfavourable prognosis and demands
intensive care.
It’s recommended to distinguish “small” and “large” criteria of severe pneumonia.
“Small” criteria of severe pneumonia:
- respiratory rate 30/min and more;
- impairment of consciousness;
- SaO2 is less than 90% (according to pulsometry), partial pressure of oxygen in the arterial
blood (further PaO2) is lower than 60mm of mercury column;
- systolic arterial pressure is lower than 90 mm of mercury column;
- bilateral or multiple lesion of lungs, destruction cavities and pleural effusion.
“Large” criteria of severe pneumonia:
- necessity of an artificial ventilation;
- rapid aggravating of focal-infiltrative changes in the lungs – increasing amount of
infiltration by more than 50% during the following two days;
- septic shock or necessity of introduction of vasopressor medicines for four hours or more;
- acute renal insufficiency (urine amount is less than 80 ml in 4 hours or kreatinine level in
blood serum is higher than 0,18m mole/l or urea nitrogen concentration is higher than 7 mmole/l
(urea nitrogen = urine (mmole/l) / 2,14) if there’s no chronic renal insufficiency.
Severe course of pneumonia is confirmed by detection of at least two “small” or one
“large” criterion. Each of them increases considerably the probability of fatal outcome. In such
cases urgent hospitalization to the department of anesthesiology and intensive care is
recommended.
Etiology
Community-acquired pneumonias may be induced by specific organisms, such as:
Streptococcus pneumonia, Haemophilus influenza, Mycoplasma pneumonia, Chlamydia
pneumonia, Legionella pneumonia, Klebsiella pneumonia, Staphylococcus aureus, Chlamydia
psittaci, Coxiella burnetti.
Nosocomial pneumonia may be induced by such organisms as: Staphylococcus aureus,
Pseudomonas aeruginosa, Klebsiella pneumonia, Escherichia coli, Proteus mirabilis,
Haemophilus influenza, Enterobacter, Peptostreptococcus, Fusobacterium, Bacteroides.
Other risk factors include exposure to cold, stress, fatigue, cigarettes smoke, alcohol and
also old age, recent influenza infection, preexisting lung disease, heart failure with disordered
lesser circulation, exposure to occupational and domestic hazard malnutrition, depression of
cerebral functions by drugs.
Pathogenesis
Aspiration Of Organisms That Colonize The Oropharynx is the most common
mechanism for the production of pneumonia. These pathogens include Streptococcus
pneumoniae, Streptococcus pyogenes, Mycoplasma pneumonia, Haemophilus influenzae, and
Moraxella catarrhalis. Nasogastric tubes can facilitate the transfer of gastric bacteria to the
pharynx.
About 50 percent of healthy adults aspirate oropharygeal secretions into the lower
respiratory tract during sleep. Aspiration occurs more frequently and may be more pronounced in
individuals with an impaired level of consciousness (eg. Alchogolics, drug abusers, and patients
who have had seizures, strokes, or general anesthesia), neurologic dysfunction of the oropharynx
and swallowing disorders or mechanical impediments (eg. Nasogastric or endotracheal tubes).
Inhalation Of Infectius Aerosols Deposition of inhaled particles within the respiratory
tract is determined primarily by particle diameter. Particles that are more than 10 um in diameter
are deposited mostly in the nose and upper airways. Particles that are less than 3 to 5 um in
diameter (also called airbone droplet nuclei) and that contain one or perhaps two microorganisms
fail to settle out by gravity but rather remain suspended in the atmosphere for long periods unless
removed by ventilation or by filtration in the lungs of the individual breathing the contaminated
air. These infectious aerosols are small enough to bypass host defenses in the upper respiratory
tract and airways. More particles are deposited in small bronchioles and alveoli as particle size
decreases below 5 um. One inhaled particle of appropriate size may be sufficient to reach the
alveolus and initiate infection. The etiologies of pneumonia typically acquired by inhalation of
infectious aerosols include tuberculosis, influenza, legionellosis, psittacosis, histoplasmosis and
Q fever.
Hematogenous Disemination From An Extrapulmonary Site Infection, usually with
Staphylococcus aureus, disseminates hematogenously to the lungs in patients (such as
intravenous drug abusers) who have either right- or left-sided bacterial endocarditis and in
patients with intravenous catheter infections. Fusobacterium infections of the retropharyngeal
tissues (retropharyngeal abscess and jugular venous thrombophlebitis) also disseminate to the
lungs.
Essentials of Diagnosis
1.Sudden onset of shaking chills, fever, chest pain, and cough with rust-colored sputum.
2.X-rays show infiltration, often lobar in distribution, but sometimes patchy.
3.Pneumococci are present in the sputum and often in the blood.
4.Leukocytosis.
Clinical manifestation
The “typical” pneumonia syndrome is characterized by the sudden onset of fever with
shaking chills, cough productive of purulent or even “rusty” sputum and in some cases pleuritic
chest pain, exaggerated by respiration but sometimes referred to the shoulder, abdomen, or flank.
The patient appears severely ill, with marked tachypnea (30-40/min) but no orthopnea.
Respirations are grunting, nares flaring, and the patient often lies on the affected side in an
attempt to splint the chest. Herpes simplex facial lesions are often present.
Initially, chest excursion is diminished on the involved side, intensified vocal fremitus and
bronchophony over the involved area. Percussion sound is shortening over the involved area.
The character of respiration can change in a different manner. Respiration can be weak
with elongated expiration and initial crepitation can appear during the initial stage of croupous
pneumonia.
At the hepatization stage bronchial respiration and moist consonating fine-bubbling rales
develop with increasing dullness of the percussion sound.
When resolution begins, numerous coars crepitations are heard, indicating liquefaction of
the alveolar exudates. Respiration becomes harsh with lessening of dullness. A pleural friction
rub may be present.
These distinct changes in the physical findings are absent in bronchopneumonia. Harsh
respiration and moist consonating fine-bubbling rales are the common symptoms of
bronchopneumonia. Sometimes (eg. In central periradicular pneumonia) the physical signs are
very scarce and pneumonia can only be revealed by x-ray examination.
Radiological examination
In lobar pneumonia, the chest radiograph shows a homogeneous opacity localised to the
affected lobe or segment; this usually appears within 12-18 hours of the onset of the illness.
Radiological examination is also particularly helpful if a complication such as pleural effusion,
intrapulmonary abscess formation or empyema is suspected. Hilar lymphadenopathy is
occasionally seen in mycoplasma pneumonia, and lung cavities are more frequently observed in
patients with staphylococcal or pneumococcal serotype 3 pneumonia.
General blood tests
Acuity of inflammation can be determined by the acute phase blood indices and their
dynamics (high leucocyte count, neutrophilic shift, accelerated ESR, high content of α2 globulins
and fibrinogen, appearance of C reactive protein, high sialic acid content). Bacterial pneumonia
is characterized by a high neutrophilic count with the shift to the left; ESR is high and it
increases with the spread and severity of the process. Leucopenia is the specific feature of viral
pneumonia. In micoplasmal pneumonia and ornitosis leucopenia combines with very high ESR.
Microbiological investigations
Sputum must be examined by Gram’s stain, by culture and by antimicrobical sensitivity
testing. Typical sputum from pneumococcal pneumonia contains many red and white cells and
many pneumococci. If sputum cannot be obtained, an attempt should be made to aspirate
secretions or washings from the trachea or lower respiratory tract either by bronchoscopy or by
inserting a needle through the cricothyroid membrane.
Identification of the etiologic microorganism is of primary importance, since this is the key
to appropriate antimicrobial therapy. However, because of the serious nature of the infection,
antimicrobial therapy generally needs to be started immediately, often before laboratory
confirmation of the causative agent. The specific microbial etiology remains elusive in about
one-third of cases, eg. When no sputum is available for examination, blood cultures are sterile,
and there is no pleural fluid.
Serologic studies are sometimes helpful to diagnose mycoplasma, chlamydia, legionella
and viral infection. But serologic confirmation requires weeks because of the late formation of
specific antibody.
Groups of patients with pneumonia
Taking into consideration certain known limits of traditional methods of etiological
diagnosis of pneumonia it’s reasonable to divide patients into separate groups. We can
distinguish the most probable causative agents and their probable response to antimicrobial drugs
with respect to each of them.
All grown-up patients with pneumonia are suggested to be divided into four groups.
The first group – patients with moderate pneumonia, who don’t need hospitalization,
without concomitant pathology and other modifying factors. The most frequent causative agent
among such patients is S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae (as a rule
among smokers) and respiratory viruses. In 30 – 50% of cases the causative agent is not detected
at all, that’s why it’s not reasonable to carry out conventional microbiological diagnostics.
Epidemiologic investigation findings (general disease incidence among a set group of young
people provoked by S. pneumoniae or M. pneumoniae) can be of value.
The second group – patients with moderate pneumonia, who don’t need hospitalization,
with concomitant pathology (chronic obstructive lung disease, renal or cardiac insufficiency,
cerebrovascular disease, tumour, diabetes mellitus, chronic hepatic disease of various etiology,
mental insanity, alcoholism) and/or other modifying factors. Pneumonia causative agents in these
cases are S. pneumoniae (including antibiotic resistant strain), H. influenzae, S, aureus, M.
catarrhalis. The possibility of gram-negative infection – family Enterobacteriacaea (E. colli,
Klebsiella spp.) also should be taken into consideration, especially among elderly people. It’s
also necessary to foreseethe the possibility of an anaerobic infection in the presence of
pneumonia in cases when patients dont have sanitized mouth cavities and there are clinicoanamnestic data about neural disease and/or deglutition disoders. Routine microbiological
diagnostics of these patients is also of little effectiveness and scarcely influences the choice of
antibiotics. In approximately 20% of cases in this group hospitalization may appear necessary
because of the lack of treatment effect among outpatients and/or exacerbation/decompensation of
concomitant diseases.
The third group – there belong patients with moderate pneumonia who need
administration to the therapeutics department according to medical indications (presence of
unfavourable prognostic factors). Pneumonia in cases of this group may be brought up by S.
pneumoniae, H. influenzae, atypical causative agents, gram-negative enterobacteria. A “mixed”
infection (i. e. combination of atypical bacterial an typical causative agents) is often detected
among 10-30% of patients of the 3rd group. Such difference in detection rate of causative agents
is explained by peculiarities of microbiological diagnostic methods, which are used by different
researchers.
The fourth group – patients with severe pneumonia who require hospitalization to
reanimation department. The spectrum of microbal flora of such patients includes S.
pneumoniae, Legionella spp., H. influenzae, gram-negative enterobacteria, S. aureus and M.
pneumonia (quite seldom). If there are modifying factors P. aeruginosa may be a causative agent.
Antibacterial therapy of pneumonia.
The diagnosis - pneumonia – is an indisputable indication for prescription of antibiotics,
which constitute the basis of treatment of such patients. Antibacterial treatment must be started
immediately after a diagnosis is made, especially for those patients with pneumonia who need
hospitalization. It’s absolutely inadmissible to waste time with prescribing antibiotics for patients
with severe disease because of absence of bacterioscopy and sputum smear findings. As
postponing of the 1st dose injection for four hours calls forth mortality risk among such patients
considerably.
An adequate clinical effect among patients of the 1st group is possible after peroral
administration of an antibacterial drug (monotherapy!). As a drug of choice amoxicillin or
macrolide (azithromycin, clarithromycin, midecamycin, spyramycin) is recommended. If the
drug of choice can’t be taken by the patient an alternative medicine – respiratory phtorchynolone
of the 3-4 generation is prescribed. In case when amoxicillin is ineffective after 48-72 hour
treatment macrolide or doxycyclyne is chosen as a medicine of the second series. This is
explained by their high activity towards atypical causative agents, which can be the most
probable reason of fail of treatment with ampicillin. In case of ineffective initial antibiotic
therapy with macrolide drugs of the second series can be amoxicillin or phtorchynolone of the 34 generation. The possible reasons of ineffective treatment with macrolide can be the presence of
pneumococcal strains resistant to this group of antibiotics or a disease brought up by gramnegative causative agents.
Among patients of the 2nd group marked clinical effect can also be reached by peroral
administration of an antibiotic. But as the probability of gram-negative organisms etiological role
increases (including those which have some mechanisms of antibiotic resistance development)
protected aminopenicilline (amoxicillin/clavulanic acid) or cephalosporin of the 2nd generation
(cefuroxim axetyle) should be used as a medicine of choice. phtorchynolone of the 3-4
generation can be used as an alternative therapy. If the medicine can’t be taken orally parenteral
cephalosporin antibiotic of the 3 generation (more preferable is ceftriaxone intramuscularly
which can be take once a day) is given. Among the patients of the 2nd group the effectiveness
absence of treatment with medicines of choice may be connected with the fact that pneumonia
etiopathogens are represented by atypical causative agents. That’s why at the 2nd stage of the
antibiotic therapy macrolide should be added to β-lactam or monotherapy with phtorchynolone
of the 3-4 generation is prescribed instead of this combination.
Patients of the 1st and 2nd groups who are hospitalized because of social conditions are
prescribed the corresponding peroral antibacterial therapy.
Patients who are taken to hospital according to medical indications are suspected to have a
severe clinical course of pneumonia. That’s why it’s more reasonable to start therapy with
prescription of antibiotics – parenteral introduction (intramuscularly, intravenously). In 3-4 days
after getting positive clinical effect (body temperature normalization, intoxication intensity
diminution and other disease symptoms decrease) a change for oral introduction of antibiotics is
possible, till completion of a full course of an antibacterial therapy (stage therapy – see below).
It’s necessary to apply combined antibiotic therapy using protected aminopenicillin
(amoxicillin / clavulanic acid, ampicilin/sulbactam) – oral administration or цефалоспорин of
the 2-3 generation (цефуроксима аксетил, цефотаксим, цефтриаксон) in combination with
macrolide for patients of the 3rd group taken to the therapeutics department. If there is no
digestive tract disturbance macrolide is administered orally. If the medicine of choice can’t be
taken by the patient phtorchynolone of the 3-4 generation (monotherapy) should be prescribed.
Among patients of this the efficacy absence during the treatment with the medicine of
choice may be connected with the fact that gram-negative bacteria producing β-lactamase of a
wide action spectrum which are inactivators of these groups of antibiotics are the causative agent
of pneumonia. Thus at the 2nd stage of the antibacterial therapy should be continued with
phtorchynolone of the 3-4 generation or carbapenem.
Patients of the 4th group should be immediately prescribed antibacterial therapy as its
postponing even for four hours increases mortality risk among such patients.
The following medicines should be prescribed intravenously for the treatment of the 4th
group patients having risk factors of contamination with P. aeruginosa: antipseudoponas
cephalosporin 3-4 generation (ceftazidin, cefoperazon, cefepim) in combination with
aminoglycocide and levofloxacine or ciprofloxacine. Cefaropim active towards morbus
caeruleus (ceftazidim, cefoperazone, cefepim) is offered as an alternative therapy in connection
with aminoglycocide and macrolide.
The estimation of antimicrobial treatment efficacy of the first series medicine must be
obligatory carried out in 48 hours after the beginning of treatment (repeated inspection of the
patient). Phone contact with the patient is also recommended on the second day of treatment.
Main efficacy criteria during this time should be intoxication intensity decrease and body
temperature dropping, absence of respiratory compromise signs. If these signs weren’t present at
the beginning of the treatment one should take into consideration his general condition and
general clinical blood count (leucocytes amount, erythrocyte sedimentation rate). The prescribed
antimicrobial therapy is continued if there is positive dynamics of the named data. If high fever
and intoxication or symptomatology aggravate then treatment must be regarded as ineffective,
the antibacterial drug must be replaced by an antibiotic of the second series and appropriateness
of hospitalization must be considered once again.
For patients with moderate pneumonia antibacterial therapy may be finished after the
temperature has been normal for 3-5 days. In such cases treatment course makes up as a rule 710 days. If clinical or epidemiological findings indicate mycoplasmal or clamydia etiology of
pneumonia the course of antimicrobial treatment makes in general 10-14 days. If positive
efficacy is reached then change of an antibiotic during this time is not reasonable.
If patients with staphylococcal pneumonia or that caused by gram-negative enterobacteria
are treated then a longer course of antibacterial therapy is recommended – 14- 21 days, if
findings show Legionella etiology of the disease – 21 days.
Ventilation and oxygenation
An adequate airway must be maintained if necessary, by tracheal suction, endotracheal
tube, or tracheostomy. Oxygen must be supplied to any patient with severe pneumonia, cyanosis
with PaO2 below 60, or marked dyspnea; this will also help to prevent pulmonary edema.
Oxygen may be supplied by nasal catheter, soft rubber mask, or oxygen tent. With masks, a 95%
oxygen concentration can be maintained, whereas with nasal tubes or tents the concentration will
reach only 40- 50%. However, masks are difficult to tolerate because of cough and
expectoration. Oxygen must be humidified to prevent drying of secretions.
Symptomatic therapy
If cough interferes with sleep and rest, it may be suppressed with codeine phosphate, 0,1g
times a day. Antipyretics are indicated for patients with high body temperature (analgin,
acetylsalicylic acid).
Detoxicating therapy – intravenous administration of rheopolyglucin, haemodes, and
other solutions are indicated for patients with pronounced toxaemia and degradation of
pulmonary infiltration.
Treatment of pleural pain
It is important to relieve pleural pain in order to allow the patient to breathe normally and
cough efficiently. Mild analgesics such as paracetamol are rarely adequate and most patients
require pethidine 50-100 mg or morphine 10-15 mg by intramuscular or intravenous injection.
Opiates, however, must be used with extreme caution in patients with poor respiratory function.
Abdominal distention is usually due to air swallowing in severe dyspnea and is a frequent
problem in patients with pneumonia. Insertion of a rectal tube will usually produce rapid initial
decompression. Gastric dilatation can be relieved by suction through a nasal tube passed into the
stomach.
Cardiac arrhythmias - extrasystoles usually require no treatment. If atrial fibrillation or
flutter develops, rapid failure may be precipitated. Rapid digitalization is usually indicated in
these cases.
Management of toxic delirium - toxic delirium occurs in any severe pneumonia and may
be particularly difficult to manage in alcoholics. Delirium, anxiety, and restlessness during
waking hours may be treated with diazepam, 5 mg, or chlordiazepoxide, 10 mg, or
phenobarbital, 15-30 mg orally 4-6 times daily. Pentobarbital, 0.1 g, or flurazepam (Dalmane),
30 mg, at bedtime helps to ensure adequate rest.
Diet - initially, the dyspneic patient is anorectic, and a liquid diet is preferred. With
improvement, a normal diet will be tolerated. If complications suggest a long illness, a highprotein, high-calorie diet with vitamin supplementation is indicated.
Evaluation of Treatment: With proper selection of antimicrobial drugs, there should be
marked improvement and defervescence in 72 hours or less. If this fails to occur, one must
consider 3 main possibilities: (1) the presence of a serious complication such as empyema,
pulmonary suppuration associated with bronchial obstruction, endocarditis, or meningitis; (2)
infection by an organism other than the pneumococcus and resistant to the drug used; and (3)
possible drug fever or other associated disease. If there is much pleural fluid, it must be aspirated
promptly, smeared, and cultured to detect infection or empyema that requires drainage. If an
organism other than the pneumococcus is shown to be the probable agent, treatment must be
directed against it.
Complications
Complications of pneumococcal pneumonia occur with the following approximate
frequencies: sterile pleural effusion (4-8%), empyema (0.5-2%), endocarditis and meningitis
(0.1-0.3%), and pericarditis (0.1%). Other complications such as pneumococcal arthritis or lung
abscess are even more rare. Fibrous organization of the pneumonia (in place of resolution)
occurs sometimes but rarely causes disability. All pleural fluid collections must be aspirated and
examined by smear and culture to permit early treatment of empyema.
Prognosis
Untreated pneumococcal pneumonia has a mortality rate of 20-40%. The following are
unfavorable prognostic signs: age over 50 years, presence of underlying disease (eg, heart
failure, cirrhosis), pregnancy, bacteremia, marked proteinuria, absence of leukocytosis,
pulmonary edema, and shock.
With early and adequate antimicrobial treatment, the fatality rate is about 5-8% but in
bacteremic pneumonia it is 17-25%. Most fatalities occur in the age groups under 2 years and
over 50 years. In untreated, uncomplicated cases, resolution by crisis (or more gradually) occurs
7-10 days after onset.
Prevention
A polyvalent vaccine containing polysaccharides from the 14 pneumococcus types that
most frequently cause infection (1,2, 3,4,6, 8, 9, 12,14,19, 23,25, 51, and 56) is available in the
USA. It has given significant protection against disease in persons at high risk: persons with
sickle cell disease, splenectomized children, persons with chronic bronchopulmonary, cardiac, or
renal disease, and elderly or debilitated persons. A single dose of 0.5 mL is given
intramuscularly and may cause local erythema, soreness, or fever. It should not be given during
pregnancy. Children at high risk can receive vaccine at age 6 months and again at 2 years. In
addition, prophylactic penicillin may be required. Regrettably, some children under 2 years of
age and some patients with myeloma or lymphoma have a poor antibody response to the vaccine.
In adults, the need for revaccination is not established.
Nosocomial pneumonia – is a disease, characterized by the appearance of new
radiological focal-infiltrative changes in the lungs in 48 hours or more after hospitalization
together with clinical symptomatology, which confirms its infectious nature (new wave of fever,
purulent sputum or purulent eliminations from the tracheo-bronhial tree, leukocytosis etc.),
excluding infections in the incubation period at the moment of hospitalization.
Diagnostic criteria of nosocomial pneumonia include:
- appearance of new radiological focal-infiltrative changes in the lungs
- two of given below signs:
1) body temperature is higher than 38,3°C;
2) bronchial hypersecretion;
3) PaO2/FiO2 (FiO2 – oxygen fraction in the exhalant air) is less then 240;
4) cough, tachypnea, local crepitation, moist rales, bronchial respiration;
5) leukocytes amount in the blood is smaller than 4,0 × 109/ l or more than 12,0 × 109/ l,
stab shift is more than 10%;
6) purulent sputum/bronchial secretion (more than 25 polymorphonuclear leukocytes in
the field of vision during microscopy with small magnification, × 100).
Diagnos – nosocomial pneumonia – is an undisputable indication for prescribing
antibiotics, which represent the main treatment in such patients. It’s necessary to start
antibacterial treatment immediately after the case is diagnosed. It’s absolutely unacceptable to
delay immediate antibiotic prescription for patients with severe disease course because of the
bacterioscopy and smear results. Such delay of the first antibiotic dose for four hours causes
considerable increase of mortality level among such patients.
Prepared by: Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 5.
Pleuritis.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
5. Name definition of pleuritis.
6. Essential of diagnosis in patients with pleural effusion.
7. Name major types of pleural effusion.
8. Name differences between transudates and exudates.
9. Name causes of pleural fluid transudates.
10.Name causes of pleural fluid exudates.
11.Clinical symptoms in patients with dry pleuritis.
12.Clinical symptoms in patients with pleural effusion.
13.Which diagnostic investigations will you prescribe to patients with
pleuritis?
14.How will you confirm the diagnosis pleuritis?
15.Name treatment in patients with pleuritis.
16.Name prognosis in patients with pleuritis.
Examples of tests
1. What is one of the causes of pleurisy?
a) appendicitis
b) ectopy of aorta
c) myocardial infarction
d) atherosclerosis
e) heart insufficiency
2. What referration of the pain is typical for irritation of the central portion of the diaphragmatic
pleura?
a) Middle part of abdomen
b) Neck and shoulder
c) Head
d) arm
e) leg
3. The most typical symptoms of pleurisy are:
a) Pleuritic pain, shallow breathing, coughing
b) Pleuritic pain, dizziness, tachicardia
c) High temperature, vomiting, obstipation
d) Law temperature, sweating
e) Pleuritic pain, vomiting, sneezing
4. Diseases that can simulate pleuritis are:
a) Chronicle hepatitis
b) Pericarditis
c) Thyroiditis
d) Pancreatitis
e) Ischemic stroke
5. What method of diagnostics is the most helpful
inflammatory abdominal disease?
a) General blood analyses
b) Computer tomography
c) X-ray
d) Termography
e) Ultrasonography
6. What drugs are used in treatment of pleurisy?
a) Sedatives
b) Antibiotics
c) b-blockers
d) antidepressants
e) vitamins
in differentiating of pluerisy with acute
Answers to tests:
1.
2.
3.
4.
5.
6.
C)
B)
A)
B)
C)
B)
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 19 - 27 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002. – 501-508 p.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 10, section 2, Chapter 257.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Pleural Effusion
The pleural space lies between the lung and chest wall and normally contains a very thin layer of
fluid, which serves as a coupling system. A pleural effusion is present when there is an excess
quantity of fluid in the pleural space.
Etiology
Pleural fluid accumulates when pleural fluid formation exceeds pleural fluid absorption.
Normally, fluid enters the pleural space from the capillaries in the parietal pleura and is removed
via the lymphatics situated in the parietal pleura. Fluid can also enter the pleural space from the
interstitial spaces of the lung via the visceral pleura or from the peritoneal cavity via small holes
in the diaphragm. The lymphatics have the capacity to absorb 20 times more fluid than is
normally formed. Accordingly, a pleural effusion may develop when there is excess pleural fluid
formation (from the interstitial spaces of the lung, the parietal pleura, or the peritoneal cavity) or
when there is decreased fluid removal by the lymphatics.
Diagnostic Approach
When a patient is found to have a pleural effusion, an effort should be made to determine the
cause. The first step is to determine whether the effusion is a transudate or an exudate. A
transudative pleural effusion occurs when systemic factors that influence the formation and
absorption of pleural fluid are altered. The leading causes of transudative pleural effusions in the
United States are left ventricular failure and cirrhosis. An exudative pleural effusion occurs when
local factors that influence the formation and absorption of pleural fluid are altered. The leading
causes of exudative pleural effusions are bacterial pneumonia, malignancy, viral infection, and
pulmonary embolism. The primary reason to make this differentiation is that additional
diagnostic procedures are indicated with exudative effusions to define the cause of the local
disease.
Approach to the diagnosis of pleural effusions. CHF, congestive heart failure; CT, computed
tomography; LDH, lactate dehydrogenase; PE, pulmonary embolism; TB, tuberculosis; PF,
pleural fluid.
Transudative and exudative pleural effusions are distinguished by measuring the lactate
dehydrogenase (LDH) and protein levels in the pleural fluid. Exudative pleural effusions meet at
least one of the following criteria, whereas transudative pleural effusions meet none:
1. pleural fluid protein/serum protein >0.5
2. pleural fluid LDH/serum LDH >0.6
3. pleural fluid LDH more than two-thirds normal upper limit for serum
The above criteria misidentify ~25% of transudates as exudates. If one or more of the exudative
criteria are met and the patient is clinically thought to have a condition producing a transudative
effusion, the difference between the protein levels in the serum and the pleural fluid should be
measured. If this gradient is greater than 31 g/L (3.1 g/dL), the exudative categorization by the
above criteria can be ignored because almost all such patients have a transudative pleural
effusion.
If a patient has an exudative pleural effusion, the following tests on the pleural fluid should be
obtained: description of the fluid, glucose level, differential cell count, microbiologic studies,
and cytology.
Effusion Due to Heart Failure
The most common cause of pleural effusion is left ventricular failure. The effusion occurs
because the increased amounts of fluid in the lung interstitial spaces exit in part across the
visceral pleura. This overwhelms the capacity of the lymphatics in the parietal pleura to remove
fluid. Isolated right-sided pleural effusions are more common than left-sided effusions in heart
failure. A diagnostic thoracentesis should be performed if the effusions are not bilateral and
comparable in size, if the patient is febrile, or if the patient has pleuritic chest pain, to verify that
the patient has a transudative effusion. Otherwise the patient is best treated with diuretics. If the
effusion persists despite diuretic therapy, a diagnostic thoracentesis should be performed. A
pleural fluid N-terminal pro-brain natriuretic peptide (NT-proBNP) >1500 pg/mL is virtually
diagnostic of an effusion secondary to congestive heart failure.
Hepatic Hydrothorax
Pleural effusions occur in ~5% of patients with cirrhosis and ascites. The predominant
mechanism is the direct movement of peritoneal fluid through small openings in the diaphragm
into the pleural space. The effusion is usually right-sided and frequently is large enough to
produce severe dyspnea.
Parapneumonic Effusion
Parapneumonic effusions are associated with bacterial pneumonia, lung abscess, or
bronchiectasis and are probably the most common cause of exudative pleural effusion in the
United States. Empyema refers to a grossly purulent effusion.
Patients with aerobic bacterial pneumonia and pleural effusion present with an acute febrile
illness consisting of chest pain, sputum production, and leukocytosis. Patients with anaerobic
infections present with a subacute illness with weight loss, a brisk leukocytosis, mild anemia,
and a history of some factor that predisposes them to aspiration.
The possibility of a parapneumonic effusion should be considered whenever a patient with a
bacterial pneumonia is initially evaluated. The presence of free pleural fluid can be demonstrated
with a lateral decubitus radiograph, computed tomography (CT) of the chest, or ultrasound. If the
free fluid separates the lung from the chest wall by >10 mm, a therapeutic thoracentesis should
be performed. Factors indicating the likely need for a procedure more invasive than a
thoracentesis (in increasing order of importance) include:
1.
2.
3.
4.
5.
loculated pleural fluid
pleural fluid pH < 7.20
pleural fluid glucose < 3.3 mmol/L (<60 mg/dL)
positive Gram stain or culture of the pleural fluid
the presence of gross pus in the pleural space
If the fluid recurs after the initial therapeutic thoracentesis, and if any of the above characteristics
are present, a repeat thoracentesis should be performed. If the fluid cannot be completely
removed with the therapeutic thoracentesis, consideration should be given to inserting a chest
tube and instilling a fibrinolytic (e.g., streptokinase, 250,000 units) or performing thoracoscopy
with the breakdown of adhesions. Decortication should be considered when the above are
ineffective.
Effusion Secondary to Malignancy
Malignant pleural effusions secondary to metastatic disease are the second most common type of
exudative pleural effusion. The three tumors that cause ~75% of all malignant pleural effusions
are lung carcinoma, breast carcinoma, and lymphoma. Most patients complain of dyspnea, which
is frequently out of proportion to the size of the effusion. The pleural fluid is an exudate, and its
glucose level may be reduced if the tumor burden in the pleural space is high.
The diagnosis is usually made via cytology of the pleural fluid. If the initial cytologic
examination is negative, then thoracoscopy is the best next procedure if malignancy is strongly
suspected. At the time of thoracoscopy, a procedure such as pleural abrasion should be
performed to effect a pleurodesis. If thoracoscopy is unavailable, then needle biopsy of the
pleura should be performed.
Patients with a malignant pleural effusion are treated symptomatically for the most part, since the
presence of the effusion indicates disseminated disease and most malignancies associated with
pleural effusion are not curable with chemotherapy. The only symptom that can be attributed to
the effusion itself is dyspnea. If the patient's lifestyle is compromised by dyspnea, and if the
dyspnea is relieved with a therapeutic thoracentesis, then one of the following procedures should
be considered: (1) insertion of a small indwelling catheter; or (2) tube thoracostomy with the
instillation of a sclerosing agent such as doxycycline, 500 mg.
Mesothelioma
Malignant mesotheliomas are primary tumors that arise from the mesothelial cells that line the
pleural cavities; most are related to asbestos exposure. Patients with mesothelioma present with
chest pain and shortness of breath. The chest radiograph reveals a pleural effusion, generalized
pleural thickening, and a shrunken hemithorax. Thoracoscopy or open pleural biopsy is usually
necessary to establish the diagnosis. Chest pain should be treated with opiates and shortness of
breath with oxygen and/or opiates.
Effusion Secondary to Pulmonary Embolization
The diagnosis most commonly overlooked in the differential diagnosis of a patient with an
undiagnosed pleural effusion is pulmonary embolism. Dyspnea is the most common symptom.
The pleural fluid is almost always an exudate. The diagnosis is established by spiral CT scan or
pulmonary arteriography Treatment of the patient with a pleural effusion secondary to
pulmonary embolism is the same as for any patient with pulmonary emboli. If the pleural
effusion increases in size after anticoagulation, the patient probably has recurrent emboli or
another complication such as a hemothorax or a pleural infection.
Tuberculous Pleuritis
In many parts of the world, the most common cause of an exudative pleural effusion is
tuberculosis (TB), but tuberculous effusions are relatively uncommon in the United States.
Tuberculous pleural effusions are usually associated with primary TB and are thought to be due
primarily to a hypersensitivity reaction to tuberculous protein in the pleural space. Patients with
tuberculous pleuritis present with fever, weight loss, dyspnea, and/or pleuritic chest pain. The
pleural fluid is an exudate with predominantly small lymphocytes. The diagnosis is established
by demonstrating high levels of TB markers in the pleural fluid (adenosine deaminase > 40 IU/L,
interferon > 140 pg/mL, or positive polymerase chain reaction (PCR) for tuberculous DNA).
Alternatively, the diagnosis can be established by culture of the pleural fluid, needle biopsy of
the pleura, or thoracoscopy. The recommended treatment of pleural and pulmonary TB is
identical.
Effusion Secondary to Viral Infection
Viral infections are probably responsible for a sizable percentage of undiagnosed exudative
pleural effusions. In many series, no diagnosis is established for ~20% of exudative effusions,
and these effusions resolve spontaneously with no long-term residua. The importance of these
effusions is that one should not be too aggressive in trying to establish a diagnosis for the
undiagnosed effusion, particularly if the patient is improving clinically.
Chylothorax
A chylothorax occurs when the thoracic duct is disrupted and chyle accumulates in the pleural
space. The most common cause of chylothorax is trauma, but it also may result from tumors in
the mediastinum. Patients with chylothorax present with dyspnea, and a large pleural effusion is
present on the chest radiograph. Thoracentesis reveals milky fluid, and biochemical analysis
reveals a triglyceride level that exceeds 1.2 mmol/L (110 mg/dL). Patients with chylothorax and
no obvious trauma should have a lymphangiogram and a mediastinal CT scan to assess the
mediastinum for lymph nodes. The treatment of choice for most chylothoraces is insertion of a
chest tube plus the administration of octreotide. If these modalities fail, a pleuroperitoneal shunt
should be placed unless the patient has chylous ascites. Patients with chylothoraces should not
undergo prolonged tube thoracostomy with chest tube drainage because this will lead to
malnutrition and immunologic incompetence.
Hemothorax
When a diagnostic thoracentesis reveals bloody pleural fluid, a hematocrit should be obtained on
the pleural fluid. If the hematocrit is more than half of that in the peripheral blood, the patient is
considered to have a hemothorax. Most hemothoraces are the result of trauma; other causes
include rupture of a blood vessel or tumor. Most patients with hemothorax should be treated with
tube thoracostomy, which allows continuous quantification of bleeding. If the bleeding emanates
from a laceration of the pleura, apposition of the two pleural surfaces is likely to stop the
bleeding. If the pleural hemorrhage exceeds 200 mL/h, consideration should be given to
thoracoscopy or thoracotomy.
Miscellaneous Causes of Pleural Effusion
There are many other causes of pleural effusion (Table 257-1). Key features of some of
these conditions are as follows: If the pleural fluid amylase level is elevated, the diagnosis of
esophageal rupture or pancreatic disease is likely. If the patient is febrile, has predominantly
polymorphonuclear cells in the pleural fluid, and has no pulmonary parenchymal abnormalities,
an intraabdominal abscess should be considered. The diagnosis of an asbestos pleural effusion is
one of exclusion. Benign ovarian tumors can produce ascites and a pleural effusion (Meigs'
syndrome), as can the ovarian hyperstimulation syndrome. Several drugs can cause pleural
effusion; the associated fluid is usually eosinophilic. Pleural effusions commonly occur
following coronary artery bypass surgery. Effusions occurring within the first weeks are
typically left-sided and bloody, with large numbers of eosinophils, and respond to one or two
therapeutic thoracenteses. Effusions occurring after the first few weeks are typically left-sided
and clear yellow, with predominantly small lymphocytes, and tend to recur. Other medical
manipulations that induce pleural effusions include abdominal surgery; radiation therapy; liver,
lung, or heart transplantation; or the intravascular insertion of central lines.
Pneumothorax
Pneumothorax is the presence of gas in the pleural space. A spontaneous pneumothorax is one
that occurs without antecedent trauma to the thorax. A primary spontaneous pneumothorax
occurs in the absence of underlying lung disease, while a secondary pneumothorax occurs in its
presence. A traumatic pneumothorax results from penetrating or nonpenetrating chest injuries. A
tension pneumothorax is a pneumothorax in which the pressure in the pleural space is positive
throughout the respiratory cycle.
Primary Spontaneous Pneumothorax
Primary spontaneous pneumothoraces are usually due to rupture of apical pleural blebs, small
cystic spaces that lie within or immediately under the visceral pleura. Primary spontaneous
pneumothoraces occur almost exclusively in smokers, which suggests that these patients have
subclinical lung disease. Approximately one-half of patients with an initial primary spontaneous
pneumothorax will have a recurrence. The initial recommended treatment for primary
spontaneous pneumothorax is simple aspiration. If the lung does not expand with aspiration, or if
the patient has a recurrent pneumothorax, thoracoscopy with stapling of blebs and pleural
abrasion is indicated. Thoracoscopy or thoracotomy with pleural abrasion is almost 100%
successful in preventing recurrences.
Secondary Pneumothorax
Most secondary pneumothoraces are due to chronic obstructive pulmonary disease, but
pneumothoraces have been reported with virtually every lung disease. Pneumothorax in patients
with lung disease is more life-threatening than it is in normal individuals because of the lack of
pulmonary reserve in these patients. Nearly all patients with secondary pneumothorax should be
treated with tube thoracostomy. Most should also be treated with thoracoscopy or thoracotomy
with the stapling of blebs and pleural abrasion. If the patient is not a good operative candidate or
refuses surgery, then pleurodesis should be attempted by the intrapleural injection of a sclerosing
agent such as doxycycline.
Traumatic Pneumothorax
Traumatic pneumothoraces can result from both penetrating and nonpenetrating chest trauma.
Traumatic pneumothoraces should be treated with tube thoracostomy unless they are very small.
If a hemopneumothorax is present, one chest tube should be placed in the superior part of the
hemithorax to evacuate the air, and another should be placed in the inferior part of the
hemithorax to remove the blood. Iatrogenic pneumothorax is a type of traumatic pneumothorax
that is becoming more common. The leading causes are transthoracic needle aspiration,
thoracentesis, and the insertion of central intravenous catheters. Most can be managed with
supplemental oxygen or aspiration, but if these are unsuccessful a tube thoracostomy should be
performed.
Tension Pneumothorax
This condition usually occurs during mechanical ventilation or resuscitative efforts. The positive
pleural pressure is life-threatening both because ventilation is severely compromised and because
the positive pressure is transmitted to the mediastinum, which results in decreased venous return
to the heart and reduced cardiac output. Difficulty in ventilation during resuscitation or high peak
inspiratory pressures during mechanical ventilation strongly suggests the diagnosis. The
diagnosis is made by physical examination showing an enlarged hemithorax with no breath
sounds, hyperresonance to percussion, and shift of the mediastinum to the contralateral side.
Tension pneumothorax must be treated as a medical emergency. If the tension in the pleural
space is not relieved, the patient is likely to die from inadequate cardiac output or marked
hypoxemia. A large-bore needle should be inserted into the pleural space through the second
anterior intercostal space. If large amounts of gas escape from the needle after insertion, the
diagnosis is confirmed. The needle should be left in place until a thoracostomy tube can be
inserted.
Prepared by: Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 6.
Pyogenic lung diseases.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
5. Name essentials of diagnosis of lung abscess.
6. Main causes of lung abscess.
7. Name possible causes when bronchial obstruction may oocur.
8. Name possible microorganisms which may cause an abscess.
9. Clinical findings in patients with lung abscess.
10.When can we say about chronic abscess?
11.Name laboratory findings in patients with lung abscess.
12.When smears and cultures for the tuberculi bacilli are especially
required?
13.Name changes in X-Ray findings/
14.Name differential diagnosis in patients with lung abscess.
15.When can we start treatment in patients with lung abscess.
16.Name treatment in patients with lung abscess.
17.Name complications in patients with lung abscess.
18.Name essential of diagnosis of bronchiectasis.
19.What is bronchiectasis?
20.Name causes of bronchiectasis.
21.When does bronchiectasis often begin?
22.Clinical findings in patients with bronchiectasis.
23.Name laboratory findings in patients with bronchiectasis.
24.Name X-Ray findings in patients with bronchiectasis.
25.What can see in bronchogram?
26.Name the differential diagnosis in patients with bronchiectasis.
27.How can we confirm bronchiectasis?
28.Name complications of bronchiectasis.
29.What is postural drainage?
30.What will you do if respiratory infection is add?
31.Name indications to surgery.
Examples of tests
1.
A.
B.
C.
D.
E.
2.
A.
How can you confirm broncyiectasis?
Bronchographic examination
X-Ray examination
Laboratory findings
Clinical findings
None
Dosing regimen of Amoxicillin|clavulanic acid:
1,0g 8-12 hurly i.v
B.
C.
D.
E.
3.
A.
B.
C.
D.
E.
4.
A.
B.
C.
D.
E.
1,2g 8-12 hurly i.v
1,4g 8-12 hurly i.v
1,6g 8-12 hurly i.v
1,8g 8-12 hurly i.v
Main way of medicine introduction for abscess is:
Orally
Intramuscular
Intravenous
Aerosol
All named above
What does Kartageners syndrom include, except:
Sinusitis
Situs in versus
Bronchiectasis
Osteoporosis
All named above
Answers to tests:
1. A
2. B
3. C
4. D
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 17 - 19 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. – Edinburgh,
2002. – 501-508 p.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 10, section 2, Chapter 252.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/ Robert
Berkow, Andrew J. Fletcher and others. – published by Merck Research
Laboratories, 1999.
Short theoretic material
LUNG ABSCESS
Essentials of Diagnosis
• Development of pulmonary symptoms about 1-2 weeks after possible aspiration, bronchial
obstruction, or previous pneumonia.
• Septic fever and sweats, and periodic sudden expectoration of large amounts of purulent, foulsmelling, or "musty" sputum. Hemoptysis may occur.
• X-ray density with central radiolucency and fluid level.
General Considerations
Lung abscess develops when necrosis and liquefaction occur in an area where necrotizing pneumonia
is present. Symptoms and signs occur 1-2 weeks after the following events: (1) massive-aspiration of
upper respiratory tract secretions and microbial flora, especially during profound suppression of cough
reflex (eg, with alcohol, drugs, unconsciousness, anesthesia, brain trauma); (2) bronchial obstruction (eg,
by atelectasis, foreign body, neoplasm); (3) presence of pneumonias, especially those caused by gram-
negative bacteria or staphylococci; or (4) formation of septic emboli from other foci of infection, or,
during bacteremia, with pulmonary infarcts. Abscess is more commonly in the lower dependent portions
of the lung. The main etiologic organisms are related to the underlying condition, but a dense mixed
anaerobic flora is often prominent, particularly when aspiration has occurred.
Clinical Findings
A. Symptoms and Signs: Onset may be abrupt or gradual. Symptoms include septic fever, sweats,
cough, and chest pain. Cough is often nonproductive at onset. Expectoration of foul-smelling brown or
gray sputum (anaerobic flora) or of purulent sputum without odor (pyogenic organism) may occur
abruptly and in large quantity. Blood-streaked sputum is also common.
Pleural pain, especially with coughing, is common because the abscess is often subpleural.
Weight
loss, anemia, and pulmonary osteoarthropathy may appear when the abscess becomes chronic (8-12
weeks after onset).
Physical findings may be minimal. Consolidation due to pneumonitis surrounding the abscess is the most
frequent finding. Rupture into the pleural space produces signs of fluid or pneumothorax.
B. Laboratory Findings: Sputum cultures are usually inadequate in determining the bacterial cause
of a lung abscess. Transtracheal aspirates should be obtained with the proper technique employed to culture anaerobic organisms in addition to the usual aerobic cultures. Special methods of transporting
specimens are required for anaerobic organisms, and appropriate culture media and methods must be
employed.
Smear and cultures for the tubercle bacilli are required, especially in lesions of the upper lobe and in
chronic abscess.
C. X-Ray Findings: A dense shadow is the initial finding. A central radiolucency, often with a
visible fluid level, appears as surrounding densities subside. Computerized tomography can supply the
detailed localization of the abscess and may also reveal primary lesions (eg, bronchogenic carcinoma)
and provide guidance for contemplated surgery. Various x-ray procedures also permit localization of
pleural involvement to facilitate drainage.
D. Instrumental Examination: Fiberoptic bronchoscopy may help to 'diagnose location and nature
of obstructions (foreign body, tumor), obtain specimens for microbiologic and pathologic examination,
and, occasionally, aid drainage.
Differential Diagnosis
Differentiate from other causes of pulmonary cavitation: tuberculosis, bronchogenic carcinoma,
mycotic infections, and staphylococcal or gram-negative bacterial pneumonia.
Treatment
Postural drainage and bronchoscopy are important to promote drainage of secretions.
A. Acute Abscess: Intensive antibacterial therapy is necessary to prevent further destruction of lung
tissue. While cultures and sensitivity tests are pending, treatment should be started with penicillin G, 2-6
million units daily. In penicillin hypersensitivity clindamycin and chloramphenicol are alternatives. If the
patient improves on antimicrobial drugs (and postural drainage),
the drugs should be continued for 4—8 weeks. If the patient fails to respond significantly to the initial
treatment, laboratory results may suggest other antimicrobials, eg, nafcillin for staphylococci, cefotaxime
for Klebsiella, cefoxitin or metronidazole for mixed anaerobes. Postural drainage is important adjunctive
treatment. Percutaneous catheter drainage has been used successfully in selected cases. Surgical therapy is
indicated mainly for severe hemoptysis and for me infrequent abscesses that fail to respond to
antimicrobial management. Failure of fever to subside after 2 weeks of therapy, abscess diameter of more
than 6 cm, and very thick cavity waits are all factors that lessen the likelihood of success with nonsurgical
treatment alone.
B. Chronic Abscess: After acute systemic manifestations have subsided, the abscess may persist.
Although many patients with chronic lung abscess can be cured with long-term treatment with
antibacterial agents, surgery may occasionally be required.
Complications
Rupture of pus into the pleural space (empyema) causes severe symptoms: increase in fever, marked
pleural pain, and sweating; the patient becomes “toxic" in appearance. Adequate drainage of empyema is
mandatory. In chronic abscess, severe and even fatal hemorrhage may occur. Metastatic brain abscess is a
well-recognized complication, and the infection may seed other organ sites. Bronchiectasis may occur as
a sequela to lung abscess even when the abscess itself is cured.
Prognosis
The prognosis in acute abscess is excellent with prompt and intensive antibiotic therapy. About 80%
of patients are healed within 7-8 weeks. The incidenee of chronic abscess is consequently low; In chronic
cases, surgery is curative.
BRONCHIECTASIS
Essentials of Diagnosis:
• Chronic cough with expectoration of large amounts of purulent sputum; hemoptysis.
• Rales and rhonchi over lower lobes.
• X-ray of chest reveals little; bronchograms show characteristic dilatations.
General Considerations
Bronchiectasis is a dilatation of small and medium-sized bronchi resulting from destruction of
bronchial elastic and muscular elements. It may be, caused by pulmonary infections (eg, pneumonia, pertussis, tuberculosis) or by a bronchial obstruction (eg, foreign bodies or extrinsic pressure). In many
patients, a history of onset following one or more episodes of pulmonary infection, usually in early
childhood, is obtained. However,since infection does not regularly produce significant bronchiectasis,
unknown intrinsic host factors presumably are present. The incidence of
the disease has been reduced by treating pulmonary infections with antibiotics.
Clinical Findings
A. Symptoms and Signs: Most patients with bronchiectasis have a history of chronic cough with
expectoration of large volumes of sputum, especially upon awakening. The sputum has a characteristic
quality of "layering out" into 3 layers upon standing, a frothy top layer, a middle clear layer, and a dense
particulate bottom layer. It is usually purulent in appearance and foul-smelling.
Intermittent hemoptysis, occasionally in dangerous proportions, is often combined with intercurrent
respiratory infections. Symptoms occur most often in patients with idiopathic bronchiectasis (ie,
childhood respiratory infections). However, patients who have bronchiectasis secondary either to
tuberculosis or chronic obstruction may not exhibit characteristic symptoms. Idiopathic bronchiectasis
occurs most frequently in the middle and lower lobes and posttuberculous bronchiectasis in the upper
lobes.
Hemoptysis is thought to result from erosion of bronchiolar mucosa with resultant destruction of underlying blood vessels. Pulmonary insufficiency may result from progressive destruction of pulmonary
tissue.
Physical findings consist primarily of rales and rhonchi over the affected segments. If the condition is faradvanced,emaciation, cyanosis, and digital clubbing may appear.
B. Laboratory Findings: There are no characteristic laboratory findings. If hypoxemia is chronic and
severe, secondary polycythemia may develop. There may be either restrictive or obstructive pulmonary
function defects associated with bronchiectasis. Hypoxemia and hypocapnia or hypercapnia may also be
associated with the disease, depending on the severity of the underlying condition. .
C.X-Ray Findings: Plain films of the chest often show increased bronchopulmonary markings in affected segments; in severe cases there may be areas of radiodensities surrounding portions of
radiolucency. Early in the course of bronchiectasis, however, the chest x-ray may be normal.
Iodized contrast media instilled into the bronchial tree (a bronchogram) demonstrates saccular, cylindric,
or fusiform dilatation of small and medium bronchi with consequent loss of the normal branching pattern.
Cylindric changes of bronchiectasis that may result from acute pneumonia will revert to normal after 6-8
weeks, but saccular dilatations represent long-standing damage and permanent disease.
.
Differential Diagnosis
The differential diagnosis includes other disorders that lead to chronic cough, sputum production, and
hemoptysis, ie, chrome bronchitis, tuberculosis, and bronchogenic carcinoma. The diagnosis of
bronchiectasis is suggested by the patient's history and can be confirmed only by bronchographic
examination or histopathologic examination of surgically removed tissue.
Complications
Recurrent infection in poorly drained pulmonary segments leads to chronic suppuration and may
cause pulmonary insufficiency. Complications include hemoptysis, respiratory failure, chronic cor
pulmonale, and amyloidosis. There is also an increased incidence of brain abscess, which is thought to
be secondary to abnormal anastomoses between bronchial (systemic) and pulmonary venous circulation.
These anastomoses produce right-to-left shunts and allow for the dissemination of septic emboli.
Treatment
A. General Measures and Medical Treatment:
1. Environmental changes- The patient should avoid exposure to all common pulmonary irritants such
as smoke, fumes, and dust and should stop smoking cigarettes.
2. Control of bronchial secretions (improved drainage)a. Postural drainage often gives effective relief of symptoms and should be utilized in every case.
The patient should assume the position that gives maximum drainage, usually lying on a bed in the prone,
supine, or right or left lateral decubitus position with the hips elevated on several pillows and no pillow
under the head. Any effective position should be maintained for 10 minutes, 2-4 times a day. The first
drainage should be done upon awakening and tee last drainage at bedtime. Family members can be
trained in the art of chest percussion to facilitate drainage of secretions.
b. Liquefaction of thick sputum may be promoted by inhaling warm mists and, in some cases,
mucolytic agents such as acetylcysteine or 5% sodium bicarbonate given by aerosol may also be helpful.
3. Control of respiratory infection-Exposure to respiratory infections should be minimized and the
patient should be vaccinated against influenza and pneumococcal pneumonia. Antibiotic therapy is indicated for acute exacerbations (ie, increased production of purulent sputum, hemoptysis, etc). Long-term
or prophylactic antibiotic therapy is controversial, since it has not been conclusively shown to be of
lasting benefit. Therefore, it seems rational to treat acute exacerbations in order to control infection but
minimize the emergence of resistant strains. Because the bacteria most commonly involved are H
inftuenzae and S pneumoniae, the drug most commonly employed is ampicillin, 250-500 mg orally every
6 hours for 5 days. Alternative therapies for the penicillin-allergic patient are erythromycin, given in the
same dosage schedule as ampicillin, or trimethoprim-sulfamethoxazole, 2 double-strength tablets twice a
day for 5 days.
B. Surgical Treatment: Surgical treatment is most often .employed when hemoptysis with bronchiectasis is recurrent and severe. Despite antibiotic therapy, localized bronchiectasis (eg, in a lower lobe
or segment) with progressive uncontrolled infection and sputum production may be an indication for
surgical removal of the affected segments.
Other Considerations
Bronchiectasis is also associated with mucoviscidosis. It is thought to be secondary to the thick
viscid secretions that cannot be cleared by normal cough mechanisms and that lead to stasis of. sputum
and chronic infection. This disorder, usually associated with sinusitis, may be accompanied by other
manifestations of mucoviscidosis. Its most common organisms are S aureus or Pseudomonas
aeruginosa.
Bronchiectasis is also associated with certain abnormalities of cellular ciliary function, the most
common of which is Kartagener's syndrome, a combination of sinusitis, situs in versus, and
bronchiectasis. Patients with this disorder show immotile cilia secondary to ultrastructural abnormalities,
stasis of sputum, failure to clear secretions, and chronic pulmonary infection that results in
bronchiectasis.
Antibiotic treatment of mucoviscidosis and Kartagener's syndrome must be guided by sensitivity
studies of organisms cultured from sputum.
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 7.
Anemia.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. To give definition of the term “Anemias”
2. Physiology of erythropoiesis and iron metabolism in organism.
3. Classifications of anemias.
4. Etiology and pathogenesis of IDA.
5. Clinic of IDA.
6. The laboratory diagnostic of IDA.
7. Diagnostic criteria of IDA.
8. Treatment of IDA.
9. Preparations of iron. Their dozes and circuits of use.
10. What is indication for iron transfusion.
11. Preventive maintenance of IDA.
12. To give definition of the term “B12 and folate deficiency anemias”
13. Etiology and pathogenesis of B12 and folate deficiency anemias.
14. Clinic of B12 and folate deficiency anemias.
15. Change of nervous system at these anemias.
16. The laboratory and instrumental diagnostic at these anemias.
17. Diagnostic criteria of B12 and folate deficiency anemias.
18. Treatment of B12 and folate deficiency anemias.
19. Features of treatment at changes of nervous system.
20. Criterion efficiency of treatment of B12 and folate deficiency anemias.
21. Preventive maintenance of B12 and folate deficiency anemias.
22. Clinic, Diagnostic and Treatment of megaloblastic anemias.
23. Concept of haemolytic and aplastic anemias
24. Etiology and pathogenesis of haemolytic anemias.
25. Classifications of inherent and acquired of haemolytic anemias.
26. Clinic of Thalassemias, Favism, hereditary spherocytosis (MinkowskyChauffard’s disease).
27. Clinic of acquired of haemolytic anemias.
28. The laboratory diagnostic of haemolytic anemias.
29. Clinic and Diagnostic of Hemoglobinopathies: Paroxysmal nocturnal
hemoglobinuria, Sickle cell anemia.
30. Treatment of haemolytic anemias and their preventive maintenance.
31. Etiology and pathogenesis of aplastic anemias
32. Clinic and complications of aplastic anemias.
33. The laboratory diagnostic of aplastic anemias.
34. Diagnostic criteria of haemolytic and aplastic anemias.
35. Differential diagnostics of haemolytic and aplastic anemias.
36.Treatment of aplastic anemias and their preventive maintenance.
37.The indications to transplantation of bone marrow.
Examples of tests
1. Name daily requirement of vitamin B 12:
a. 1 – 3 μkg
b. 2 – 7 μkg
c. 15 – 20 μkg
d. 30 – 50 μkg
2. Where the normal physiology absorption of vitamin B 12 may occur?
a. in the stomach
b. in the duodenum
c. in the jejunem
d. in the terminal ileum
3. Name daily requirement of folate:
a. 100 μkg
b. 300 μkg
c. 500 μkg
d. 700 μkg
4. Name systems that may disturb in patients with vitamin B 12 deficiency anaemia:
a. hematopoietic system
b. respiratory system
c. nervous system
d. digestive system
Answers to tests:
1.
2.
3.
4.
b
d
a
a, c, d
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 326 - 375 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. – Edinburgh,
2002.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 6, section 2, Chapter 98. 100 - 102.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Anemia - is the decreasing of hemoglobin and red blood cells amount in the unit
of blood volume.
From data of WHO:
a hematocrit less than 40 in men and 37 in women, or hemoglobin less than 130 g/l
in men and less than 120 g/l in women.
Blood & Lymphocyte Development
Actuality of theme:
Anemia is very often met in 20% women of the developed countries and in 50%
women of the non-developed countries;
More than 50% patients with chronic diseases and tumors;
Considerably worsens quality of life and capacity.
Clinical classification of anemia is based on morphological prinsiple determination of mean corpuscular volume (MCV) of red blood cells
MСV- is determined by automatic laboratory analyzers or by such formula: MСV
= (hematocrit x10) / amount of RBC (in mln/l).
Classification
In the morphological approach, anemia is classified by the size of red blood cells;
this is either done automatically or on microscopic examination of a peripheral
blood smear.
The size is reflected in the mean corpuscular volume (MCV):
• If the cells are smaller than normal (under 80 fl), the anemia is said to be
microcytic;
• if they are normal size (80-100 fl), normocytic;
• and if they are larger than normal (over 100 fl), the anemia is classified as
macrocytic.
Normocytic anemia
(MCV - 80-100)
• A loss or destruction of RBC is increased
• Decreasing of RBC synthesis
• Pathology of bone marrow (for example, action of medications, infection,
aplastic anemia, myelodysplastic syndrome, plural mieloma and other
infiltrative diseases).
Causes of Normocytic anemia
• acute blood loss
• anemia of chronic disease
• aplastic anemia (bone marrow failure).
Microcytic anemia
(MCV less than 80)
Microcytic anemia is primarily a result of hemoglobin synthesis
failure/insufficiency, which could be caused by:
• Heme synthesis defect
• Globin synthesis defect
• Sideroblastic defect
Makrocytic anemia
(MCV more than 100 fl)
- Megaloblastic anemia (vitamin В12 or folic acid deficiency )
- Toxic effect of chemotherapeutic agents (methotrexate) or other medications
(zidovudine (AZT), phenytoin)
- Pathology of bone marrow
- Chronic abuse by alcohol (toxic effect)
- Liver disease
Anemia during pregnancy
Anemia affects 20% of all females of childbearing age in the United States and
Europe. Because of the subtlety of the symptoms, women are often unaware that
they have this disorder, as they attribute the symptoms to the stresses of their daily
lives. Possible problems for the fetus include increased risk of growth retardation,
prematurity, intrauterine death, rupture of the amnion and infection.
During pregnancy, women should be especially aware of the symptoms of anemia,
as an adult female loses an average of two milligrams of iron daily. Therefore,
she must intake a similar quantity of iron in order to make up for this loss.
Additionally, a woman loses approximately 500 milligrams of iron with each
pregnancy, compared to a loss of 4-100 milligrams of iron with each period.
Depends on the level of hemoglobin in the blood anemia is divided on:
- mild degree (Hb 110-90 g/l),
- moderate degree (Hb 89-70 g/l),
- severe degree (Hb less than 69 g/l).
Depends on the size of RBC and their saturation by hemoglobin (from data of
colour index - CI) anemia is divided on:
-Normocytic normochromic anemia: colour of RBC is normal and CI is 0,86-1,1;
-Microcytic anemia (can be hypo- or normochromic): microcytosis ,
anizopoykilocytosis, hypochromia, CI < 0,8;
-Makrocytic anemia: makrocytosis, even megalocytosis, CI > 1,1.
ANEMIA CAUSES
• External bleeding: Loss of blood through heavy menstrual bleeding,
wounds, as well as stomach ulcers can cause anemia.
• Iron deficiency: The bone marrow needs iron to make red blood
cells.
• Anemia of chronic disease: Any long-term medical condition can
lead to anemia.
• Kidney disease: The kidneys help the bone marrow to make red
blood cells.
• Pregnancy: Water weight gain during pregnancy dilutes the red blood
cells.
• Poor nutrition: Vitamins and minerals are required to make red
blood cells.
• Alcoholism.
• Uncommon causes of anemia: bleeding disorders, liver disease,
thalassemia, infection, cancer, arthritis, enzyme deficiency, sickle cell
disease, hypothyroidism, toxins, or hereditary conditions.
Signs and symptoms
Signs of anemia may include the following:
•Black and tarry stools (sticky and foul smelling)
•Maroon, or visibly bloody stools
•Rapid heart rate
•Rapid breathing
•Pale or cold skin
•Jaundice
•Low blood pressure
•Heart murmur
•Enlargement of the spleen
Symptoms of anemia may include the following:
•Fatigue
•Trouble breathing
•Chest pain
•Abdominal pain
•Weight loss
•Weakness
•Dizziness and passing out, especially upon standing
Diagnosis
The only way to diagnose anemia is with a blood test. Generally, a full blood
count is done. Apart from reporting the amount of red blood cells and the
hemoglobin level, the automatic counters also measure the size of the red blood
cells, which is an important tool in distinguishing between the causes.
Occasionally, other tests are required to further distinguish the cause for anemia.
These are discussed with the differential diagnosis (below). The doctor may also
decide to take some other screening blood tests that might identify the cause of
fatigue; glucose levels, ESR, ferritin, renal function tests and electrolytes may
be part of such a workup.
Doctor has a lot of questions in case of patient with anemia:
1. What is the reason of anemia? Is this anemia an independent disease or only
syndrome, the complication of present patient`s pathology? Is this anemia the sign
of the blood system disease?
2. What is the minimum of diagnostic measures, necessary for finding out of
anemia character?
3. Do we need the consultation of hematologist? And if this so, what is their
urgency?
4. What is the treatment?
STANDARDS
DIAGNOSTICS AND TREATMENT OF IRON DEFICIECY ANEMIA
Iron deficiency is defined as a decreased total iron body content.
Iron deficiency anemia occurs when iron deficiency is sufficiently severe to
diminish erythropoiesis and cause the development of anemia. Iron deficiency is
the most prevalent single deficiency state on a worldwide basis.
In healthy people, the body concentration of iron (approximately 60 parts per
million [ppm]) is regulated carefully by absorptive cells in the proximal small
intestine, which alter iron absorption to match body losses of iron. Persistent errors
in iron balance lead to either iron deficiency anemia or hemosiderosis. Both are
disorders with potential adverse consequences.
Principal reasons of IDA are:
1. Diseases of GIT.
2. Diseases of kidneys which are accompanied by mikro- and makrohematuria.
3. Diseases of the cardio-vascular system.
4. Breathing diseases.
5. Pathology of the blood system.
6. Hemorrhagic diatesis.
7. Meno- and metrorhagia
8. Pregnancy
9. Invasion of intestinal worms.
10. Malignant tumors
Clinical symptoms of IDA
A. Sideropenia.
B. Circulatory-hypoxic syndrome. C. Anemic syndrome.
CLINICAL CLASSIFICATION
OF IRON DEFICIENCY ANEMIA
І. Preclinical stage
1.1. Prelatent deficit of iron.
1.2. Latent deficit of iron (bleeding, unregulated participating in a donorship,
increasing necessity in iron and others like that).
ІІ. Clinical stage
2.1. No complicated form is caused by:
2.1.1. Chronic bleeding;
2.1.2. Increased necessity in iron (pregnancy, lactation, period of growth and
ripening, for sportsmen);
2.1.3. An insufficient initial level of iron in organism;
2.1.4. Insufficient resorbtion of iron in a GIT;
2.1.5. Disturbances of transport and utilizations of iron (gipo- and atransferinemia,
enzimopathia, autoimmunic processes);
2.1.6. Alimentary insufficiency of iron;
2.2. Complicated form is caused by:
2.2.1. Anemic hypoxia (signs: light, middle and severe, severe with the dystrophic
changes of organs - hypoxic myocardial dystrophy, encephalopathia and others like
that);
2.2.2. Sideropenic syndrome (signs : neurological disorders of emotional sphere,
taste, sense of smell, dizuric disorders, changes of mucus shell of GIT, skin and its
additions and others like that);
2.2.3. Metabolic endogenous intoxication.
ІІІ. Mixed forms of iron deficiency anemia:
3.1. Dimorphic anemia (combination of iron deficiency anemia with vitamin
В12 deficiency anemia);
3.2. Combination of iron deficiency anemia with the deficit of vitamins
(group B, E, C);
3.3. Combination of iron deficiency anemia with the deficit of
microelements;
3.4. Polydeficiency anemia (combination of iron deficiency anemia with the
deficit of vitamins and microelements).
Treatment of iron deficiency anemia
- liquidation of reasons which caused the deficit of iron;
- addition to the supplies of iron (therapy of satiation): using, mainly, peroral
preparations of iron in day's dose of 2-3 mg of elementary (Fe++) iron on 1 kg of
mass.
Adopting iron is required simultaneously with ascorbic acid. More rapid getting up
of indexes of red blood is observed at simultaneous application of antioxidants.
Treatment iron is conducted 4-6 months: in a complete dose preparations appoint
to normalization of indexes of red blood, whereupon a dose is diminished half.
Basic modern drugs
A. Monocomponent preparations
- Arystiferon (ferrum sulfas)
- Ferro-gradument (ferrum sulfas)
- Ferronal (ferrum gluconas)
- Ferrogluconat (ferrum gluconas)
- Hemofer prolongatum (ferrum sulfas)
- Heferol (ferrum fumaras)
- Iron vine (ferrum sacharas)
B. Combine preparations
- Tardyferon-retard (ferrum sulfas, Vit C)
- Gyno-tardyferon (ferrum sulfas, Vit C, folic acid)
- Sorbifer-durulis (ferrum sulfas, Vit C)
- Fenuls (ferrum sulfas, Vit C, B)
- Makrofer (ferrum gluconas, folic acid)
- Aktyferrin (ferrum sulfas, D,L-seryn)
- Globiron (ferrum fumaras)
- Ranferon (ferrum fumaras, Vit C, B12, B9, Zinci sulfas)
C. Preparations for parenteral introduction
• Ferbitol
• Fercoven
• Ferrum-lek
• Venofer
• Maltofer
• Ferlecyt
• Gektofer
CRITERIA OF IRON DEFICIENCY ANAEMIA TREATMENT
EFFICIENCY
7-10 days – retikulocytes` crisis,
3-4 weeks - normalization of hemoglobin level, amount of blood red corpuscles
and hematokrit,
10-12 week - normalization of blood ferritin level.
STANDARDS OF DIAGNOSTICS AND TREATMENT OF
MEGALOBLASTIC ANEMIA
Megaloblastic anemia is anemia, caused disturbances of DNA and RNA synthesis
in erythroid cells which appear on the basis of vitamin of В12 and folic acid
deficit.
Reasons of megaloblastic anemia:
• Addison-Birmer disease (autoimmune disease, caused by the presence of
antibodies against the Kastl`s internal factor of);
• State after the resection of stomach;
• Stomach cancer;
• Diseases of thin intestine;
• Parasitizes diseases;
• Initial deficit of transcobalamin II;
• Alimentary insufficiency of vitamin В12.
This image shows a large PMN with multiple discretely-identifiable nuclear lobes, usually seen in megaloblastic
anemias. Normal PMN's have less than or equal to 5 lobes.
This picture shows large, dense, oversized, red blood cells (RBCs) that are seen in megaloblastic anemia.
Megaloblastic anemia can occur when there is a deficiency of vitamin B-12.
Diagnostic search
Conducted additionally:
- sternal punction - megaloblastic type of erythropoesis;
- fibrogastroskopia, biopsy of mucus stomach;
- establishment of reason of vitamin В12 or folic acid deficit.
Anamnesis: to pay attention to gradual development of disease, general weakness.
Clinics - characteristic triad of syndromes:
1. Anemic (pallor of skin and mycoses, subikterosis of skin and sclera);
2. Damage of digestive organs (Genter`s tongue - in the first phase bright red,
sickly, later - smooth, glossy; atrophic gastritis);
3. Neurological syndrome (funikularis myelosis).
Characteristic changes:
hyperchromic anemia (colored index > 1.0), leukopenia, can be
thrombocytopenia, in blood analysis - makrocytosis, elliptocytosis, anisocytosis,
bazofil grittiness appears in red corpuscles, red corpuscles with the Kebot`s rings
and little Zholli`s bodie, gigantic neutrophiles with the hypersegmented
kernel;analysis of gastric juice (histaminrezisten inacidity); increasing of indirect
bilirubin.
Reasons of folic acid deficit:
- alcoholism;
- liver cirrhosis;
- violation of absorption of folic acid is in a thin bowel;
-alimentary insufficiency of folic acid;
-taking some medicines (antagonists of purins, sulfanilamides).
Treatment of the vitamin В12 deficit:
• vitamin В12 (cyanocobalamin) in a dose 500 mkg intramuscular daily
during 2 weeks, and later - one time for a week to normalization of indexes
of red blood;
• dispansery supervision of hematologist - the vitamin В12 in a dose 500 mkg
intramuscular one time on a month during all life;
• patients with the expressed neurological syndrome during the first half-year
get the dose of vitamin В12 on 50 % more high;
• used the transfusion of red corpuscles concentrate only in extremely heavy
cases at presence of cardio-vascular insufficiency.
Treatment of the folic acid deficit:
• folic acid in the dose of 5 mg - 1-3 times per a day реr оs during 2-3 weeks
(if reason of deficit is not permanent).
• in the case of ineffectiveness of the indicated therapy patients with the
megaloblastic type of erythropoesis must be directed in a hematological
center, hematological institute for authentication of diagnosis
(eritroleukemia is possible or other pathology).
Sickle cell anemia is an inherited blood disease in which the red blood cells
produce abnormal pigment (hemoglobin). The abnormal hemoglobin causes
deformity of the red blood cells into crescent or sickle-shapes, as seen in this
photomicrograph.
Elliptocytosis is a hereditary disorder of the red blood cells (RBCs). In this
condition, the RBCs assume an elliptical shape, rather than the typical round shape.
Spherocytosis is a hereditary disorder of the red blood cells (RBCs), which may be
associated with a mild anemia. Typically, the affected RBCs are small, spherically
shaped, and lack the light centers seen in normal, round RBCs.
Sickle cell anemia is an inherited disorder in which abnormal hemoglobin (the red
pigment inside red blood cells) is produced. The abnormal hemoglobin causes red
blood cells to assume a sickle shape, like the ones seen in this photomicrograph.
Red blood cells (RBCs) are normally round. In ovalocytosis, the cells are oval.
Other conditions that produce abnormally shaped RBCs include spherocytosis and
eliptocytosis.
These crescent or sickle-shaped red blood cells (RBCs) are present with Sickle cell
anemia, and stand out clearly against the normal round RBCs. These abnormally
shaped cells may become entangled and block blood flow in the small blood
vessels (capillaries).
This photomicrograph of red blood cells (RBCs) shows both sickle-shaped and
pappenheimer bodies.
These abnormal red blood cells (RBCs) resemble targets. These cells are seen in
association with some forms of anemia, and following the removal of the spleen
(splenectomy).
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 8.
Acute and chronic leukemias.
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. To give definition of the term “HEMOBLASTOSIS”
2. Classifications of HEMOBLASTOSIS.
3. To give definition of the term “Acute leucosis (Acute Leukemias)” (AL).
4. Classifications of AL.
5. Etiology and pathogenesis of AL.
6. To list basic clinical syndromes at AL.
7. Laboratory diagnostic of AL.
8. Diagnostic criteria and Differential diagnostics of AL.
9. Treatment of AL.
10. That is complete remission of AL.
11. Diagnostic, Clinic and Treatment of hematosarcoma.
12. Classifications of myeloproliferative disease.
13. Diagnostic criteria of Chronic Myelocytic.
14. Treatment of Chronic Myelocytic.
15. Diagnostic criteria of Polycythemia.
16. Diagnostic, Clinic and Treatment of Myelofibrosis (Agnogenic Myeloid
Metaplasia; Myelofibrosis with Myeloid Metaplasia).
17. Etiology and pathogenesis of Chronic Lymphocytic.
18. Laboratory diagnostic of Chronic Lymphocytic.
19. Diagnostic criteria and Differential diagnostics of Chronic Lymphocytic.
20. Differential diagnostics of Chronic leukemia and hematosarcomas.
21. Treatment of Chronic Lymphocytic.
22. To give definition of the term “leukemoid reaction”.
23. Tape of leukemoid reaction and Differential diagnostics with AL.
24. Treatment of leukemoid reaction.
Examples of tests
1. Name etiology factors of leukaemias:
A. exposure to ionizing radiation
B. viral infection
C. chromosomal tramslocation
D. immunodeficiency disorder
E. all named above
2. In which age could you mostly see acute lymphocytic leukaemia?
A. in childhood
B. in young adults
C. in the middle age
D. in old age
3. Name main cells in CBC you can see in patients with acute leukaemia:
A. prolymphocytes
B. plasmocytes
C. blasts
D. lymphocytes
4. Name the goal of treatment in patients with acute leukaemia:
A. normal hematopoiesis with less than 20 % blast cells
B. normal hematopoiesis with less than 15 % blast cells
C. normal hematopoiesis with less than 10 % blast cells
D. normal hematopoiesis with less than 5 % blast cells
Answers to tests:
1. E, 2. A, 3. C, 4. D
References.
1. Therapy: Manual. The course of lectures/V. M. Fedosyeyeva, A. A.
Chrenov. – Simferopol, 2003. – 375 - 391 p.
2. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002.
3. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 6, section 2, Chapter 104.
4. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
What is leukemia? Leukemia is a type of cancer. Cancer is a group of many
related diseases. All cancers begin in cells, which make up blood and other tissues.
Normally, cells grow and divide to form new cells as the body needs them. When
cells grow old, they die, and new cells take their place. Sometimes this orderly
process goes wrong. New cells form when the body does not need them, and old
cells do not die when they should. Leukemia is cancer that begins in blood cells.
Blood cells form in the bone marrow. Bone marrow is the soft material in the
center of most bones. Immature blood cells are called stem cells and blasts. Most
blood cells mature in the bone marrow and then move into the blood vessels. Blood
flowing through the blood vessels and heart is called the peripheral blood.
Blood & Lymphocyte Development
The bone marrow makes different types of blood cells.
Each type has a special function:
White blood cells help fight infection
Red blood cells carry oxygen to tissues throughout the body
Platelets help form blood clots that control bleeding
Leukemia (or leukaemia) is a cancer of the blood or bone marrow characterized
by an abnormal proliferation of blood cells, usually white blood cells (leukocytes).
It is part of the broad group of diseases called hematological neoplasms.
Symptoms. Damage to the bone marrow, by way of displacing the normal marrow
cells with increasing numbers of malignant cells, results in a lack of blood
platelets, which are important in the blood clotting process. This means people
with leukemia may become bruised, bleed excessively, or develop pinprick bleeds
(petechiae). White blood cells, which are involved in fighting pathogens, may be
suppressed or dysfunctional, putting the patient at the risk of developing infections.
Finally, the red blood cell deficiency leads to anemia, which may cause dyspnea.
All symptoms may also be attributable to other diseases; for diagnosis, blood tests
and a bone marrow biopsy are required.
Some other related symptoms:
Fever, chills, and other flu-like symptoms
Weakness and fatigue
Loss of appetite and/or weight
Swollen or bleeding gums
Neurological symptoms (headache)
Enlarged liver and spleen
Leukemia is clinically and pathologically split into its acute and chronic forms
Acute leukemia is a rapidly progressing disease that affects mostly cells that are
unformed or immature (not yet fully developed or differentiated). These
immature cells cannot carry out their normal functions.
Acute forms of leukemia can occur in children and young adults. (In fact, it is a
more common cause of death for children than any other type of malignant
disease.)
Immediate treatment is required in acute leukemias due to the rapid progression
and accumulation of the malignant cells, which then spill over into the bloodstream
and spread to other organs of the body. If left untreated, the patient will die within
months or weeks.
Chronic leukemia progresses slowly and permits the growth of greater numbers
of more developed cells. In general, these more mature cells can carry out some of
their normal functions. Typically taking months to years to progress, the cells are
produced at a much higher rate than normal cells, resulting in many abnormal
white blood cells in the blood. Chronic leukemia mostly occurs in older people, but
can theoretically occur in any age group. Whereas acute leukemia must be treated
immediately, chronic forms are sometimes monitored for some time before
treatment to ensure maximum effectiveness of therapy.
Furthermore, the diseases are classified according to the type of abnormal cell
found most in the blood.
When leukemia affects lymphoid cells (lymphocytes and plasma cells), it is called
lymphocytic leukemia.
When myeloid cells (eosinophils, neutrophils, and basophils) are affected, the
disease is called myeloid or myelogenous leukemia.
The major forms of leukemia are divided into four categories. The terms
myelogenous or lymphocytic denote the cell type involved. Myelogenous and
lymphocytic leukemia each have an acute or chronic form. Thus, the four major
types of leukemia are acute or chronic myelogenous and acute or chronic
lymphocytic leukemia.
Prevalence of the four major types
Acute lymphocytic leukemia (also known as Acute Lymphoblastic Leukemia, or
ALL) is the most common type of leukemia in young children. This disease also
affects adults, especially those age 65 and older
Acute myelogenous leukemia (also known as Acute Myeloid Leukemia, or AML)
occurs more commonly in adults than in children. This type of leukemia was
previously called acute nonlymphocytic leukemia.
Chronic lymphocytic leukemia (CLL) most often affects adults over the age of 55.
It sometimes occurs in younger adults, but it almost never affects children.
Chronic myelogenous leukemia (CML) occurs mainly in adults. A very small
number of children also develop this disease.
The most common forms in adults are AML and CLL, whereas in children ALL is
more prevalent
Leukemia.Causes and Risk Factors
There is no single known cause for all of the different types of leukemia. The
different leukemias likely have different causes, and very little is certain about
what causes them. Researchers have strong suspicions about four possible causes:
- natural or artificial ionizing radiation,
- certain kinds of chemicals,
- some viruses, and
- genetic predispositions.
Leukemia, like other cancers, result from somatic mutations in the DNA which
activate oncogenes or deactivate tumor suppressor genes, and disrupt the regulation
of cell death, differentiation or division. These mutations may occur spontaneously
or as a result of exposure to radiation or carcinogenic substances and are likely to
be influenced by genetic factors.
Viruses have also been linked to some forms of leukemia. For example, certain
cases of ALL are associated with viral infections by either the human
immunodeficiency virus (HIV, responsible for AIDS) or human T-lymphotropic
virus (HTLV-1 and -2, causing adult T-cell leukemia/lymphoma).
Fanconi anemia is also a risk factor for developing acute myelogenous leukemia.
Until the cause or causes of leukemia are found, there is no way to prevent the
disease.
Acute leukemia. Essentials of diagnosis.
Short duration of symptoms, including fatigue, fever, and bleeding
Cytopenia or pancytopenia
More than 20 % blasts in the bone marrow
Blasts in peripheral blood in 90 %
Acute leukemia. Stages
Beginning
Developping
Remission
full – the level of blasts in the bone marrow les than 5 %, in the blood – absence,
not full – clinical & hematology recovery but blasts are present
Recidiv
Terminal
Acute leukemia. Clinics
Anemic syndrome
Hemmoragic syndrome (due to decreasing of platelets)
Infective & ulcer-necrotic complications (due to decreasing of leukocytes)
Extra-bone marrow localisation (lymphadenopathia, splenomegalia, leucemic
infiltrationsin the skin, CNS, mammory glands, testis)
Acute leukemia. Laboratory findings
Pancytopenia with circulating blasts (in 10 % blasts may be absent – aleukemic
leukemia)
The level of leucocytes may be sometimes little increase
The bone marrow is hypercellular & dominated by blasts
Acute lymphoblastic leukemia (ALL) - is a cancer of the white blood cells,
characterised by the overproduction and continuous multiplication of malignant
and immature white blood cells (referred to as lymphoblasts) in the bone marrow.
It is a hematological malignancy.
It is fatal if left untreated as ALL spreads into the bloodstream and other vital
organs quickly (hence "acute"). It mainly affects young children and adults over
50.
This picture shows the darkly-stained lymph cells (lymphoblasts) seen in acute
lymphocytic leukemia (ALL), the most common type of childhood leukemia.
ALL. Classification
Subtyping of the various forms of ALL is done according to the FAB (FrenchAmerican-British) classification, which is used for all acute leukemias (including
acute myelogenous leukemia, AML).
The FAB classification is:
ALL-L1: small uniform cells
ALL-L2: large varied cells
ALL-L3: large varied cells with vacuoles (bubble-like features)
ALL. Treatment
The earlier acute lymphocytic leukemia is detected, the more effective the
treatment. The aim is to induce a lasting remission, defined as the absence of
detectable cancer cells in the body (usually less than 5% blast cells on the bone
marrow).
Treatment for acute leukemia can include chemotherapy, steroids, radiation
therapy, intensive combined treatments (including bone marrow or stem cell
transplants), and growth factors.
ALL. Treatment
Stages:
Induction
Consolidation
CNS prophilaxis
Maintaince treatment
Prognosis
Advancements in medical technology and research over the past four decades in
the treatment of ALL has improved the overall prognosis significantly from 0 to
20-75 % survival rate, largely due to the continuous development of clinical trials
and improvements in bone marrow transplantation (BMT) and stem cell
transplanation (SCT) technology.
The prognosis for ALL differs between individuals depending on a wide variety of
factors:
Sex: females tend to fare better than males.
Ethnicity: Caucasians are more likely to develop acute leukemia than AfricanAmericans, Asians and Hispanics and tend to have a better prognosis than nonCaucasians.
Age at diagnosis: children between 1-10 years of age are most likely to be cured.
White blood cell count at diagnosis of less than 50,000
Whether the cancer has spread to the brain or spinal cord
Morphological, immunological, and genetic subtypes
Response of patient to initial treatment
Genetic disorders such as Down's Syndrome
Acute myeloid leukemia (AML)
is a cancer of the myeloid line of white blood cells, characterized by the rapid
proliferation of abnormal cells which accumulate in the bone marrow and interfere
with the production of normal blood cells.
AML is the most common acute leukemia affecting adults, and its incidence
increases with age. While AML is a relatively rare disease overall, accounting for
approximately 1.2% of cancer deaths in the United States, its incidence is expected
to increase as the population ages
Note multiple Auer rods which are found only in acute myeloid leukemias, either
myeloblastic or monoblastic. These rods consist of clumps of azurophilic granule
material.
AML. Classification
The two most commonly used classification schemata for AML, as of 2006, are
the older French-American-British (FAB) system and the newer World Health
Organization (WHO) system.
French-American-British classification
The French-American-British (FAB) classification system divided AML into 8
subtypes, M0 through to M7, based on the type of cell from which the leukemia
developed and its degree of maturity. This is done by examining the appearance of
the malignant cells under light microscopy and/or by using cytogenetics to
characterize any underlying chromosomal abnormalities. The subtypes have
varying prognoses and responses to therapy.
The
eight FAB subtypes are:
M0 (undifferentiated AML)
M1 (myeloblastic, without maturation)
M2 (myeloblastic, with maturation)
M3 (promyelocytic), or acute promyelocytic leukemia (APL)
M4 (myelomonocytic)
M4eo (myelomonocytic together with bone marrow eosinophilia)
M5 monoblastic leukemia (M5a) or monocytic leukemia (M5b)
M6 (erythrocytic), or erythroleukemia
M7 (megakaryoblastic)
Acute monocytic leukemia. These lesions are rarely found in chronic leukemia but
are a common finding in acute forms. They appear as erythematous infiltrations of
the skin, forming papules, macules, and plaques. Pruritus may be present.
World Health Organization classification
The World Health Organization (WHO) classification of acute myeloid leukemia
attempts to be more clinically useful and to produce more meaningful prognostic
information than the FAB criteria.
The WHO subtypes of AML are:
AML
with characteristic genetic abnormalities, which includes AML with
translocations between chromosome 8 and 21 [t(8;21)], inversions in chromosome
16 [inv(16)], or translocations between chromosome 15 and 17 [t(15;17)]. Patients
with AML in this category generally have a high rate of remission and a better
prognosis compared to other types of AML.
AML with multilineage dysplasia. This category includes patients who have
had a prior myelodysplastic syndrome (MDS) or myeloproliferative disease (MPD)
that transforms into AML. This category of AML occurs most often in elderly
patients and often has a worse prognosis.
AML and MDS, therapy-related. This category includes patients who have had
prior chemotherapy and/or radiation and subsequently develop AML or MDS.
These leukemias may be characterized by specific chromosomal abnormalities, and
often carry a worse prognosis.
AML not otherwise categorized. Includes subtypes of AML that do not fall into
the above categories.
Acute leukemias of ambiguous lineage. Acute leukemias of ambiguous lineage
(also known as mixed phenotype or biphenotypic acute leukemia) occur when the
leukemic cells can not be classified as either myeloid or lymphoid cells, or where
both types of cells are present.
AML. Prognosis
Acute myeloid leukemia is a curable disease; the chance of cure for a specific
patient depends on a number of prognostic factors.
The single most important prognostic factor in AML is cytogenetics, or the
chromosomal structure of the leukemic cell. About half of AML patients have
"normal" cytogenetics; they fall into an intermediate risk group. A number of other
cytogenetic abnormalities are known to associate with a poor prognosis and a high
risk of relapse after treatment.
AML which arises from a pre-existing myelodysplastic syndrome or
myeloproliferative disease (so-called secondary AML) has a worse prognosis, as
does treatment-related AML arising after chemotherapy for another previous
malignancy. Both of these entities are associated with a high rate of unfavorable
cytogenetic abnormalities.
In some studies, age >60 years and elevated lactate dehydrogenase level were
also associated with poorer outcomes. As with most forms of cancer, performance
status (i.e. the general physical condition and activity level of the patient) plays a
major role in prognosis as well.
Cure rates in clinical trials have ranged from 20-45%; however, it should be
noted that clinical trials often include only younger patients and those able to
tolerate aggressive therapies. The overall cure rate for all patients with AML
(including the elderly and those unable to tolerate aggressive therapy) is likely
lower.
AML. Treatment
Treatment of AML consists primarily of chemotherapy, and is divided into two
phases:
induction
postremission (or consolidation) therapy.
The goal of induction therapy is to achieve a complete remission by reducing the
amount of leukemic cells to an undetectable level;
the goal of consolidation therapy is to eliminate any residual undetectable disease
and achieve a cure.
Chronic myelogenous leukemia (CML)
is a form of chronic leukemia characterized by increased and unregulated clonal
production of predominantly myeloid cells in the bone marrow.
CML is a myeloproliferative disease associated with a characteristic
chromosomal translocation called the Philadelphia chromosome.
Historically, it has been treated with chemotherapy, interferon and bone marrow
transplantation, although targeted therapies introduced at the beginning of the 21st
century have radically changed the management of CML.
The Philadelphia chromosome as seen by metaphase FISH
CML. Essentials of diagnosis
Strikingly elevated white blood count
Markedly left-shifted myeloid series but with a low percentage of promyelocytes
and blasts
Presence of Philadelphia chromosome or bcr-abl gene
Oil immersion field demonstrating myeloid cells of all degrees of maturity
This high-power microscopic view of a blood smear from a person with classical
CML shows predominantly normal-appearing cells with intermediate maturity
CML. Phases
CML is often divided into three phases based on clinical characteristics and
laboratory findings. In the absence of intervention, CML typically begins in the
chronic phase, and over the course of several years progresses to an accelerated
phase and ultimately to a blast crisis. Blast crisis is the terminal phase of CML and
clinically behaves like an acute leukemia. One of the drivers of the progression
from chronic phase through acceleration and blast crisis is the acquisition of new
chromosomal abnormalities (in addition to the Philadelphia chromosome). Some
patients may already be in the accelerated phase or blast crisis by the time they are
diagnosed.
Low power view showing marked hypercellularity with a broad-spectrum of
myeloid and erythroid cell types and marked myeloid hyperplasia
CML. Treatment
General strategies for management include a variety of options:
Leukapheresis, also known as a peripheral blood stem cell transplant, with stem
cell cryopreservation (frozen storage) prior to any other treatment. The patient's
blood is passed through a machine that removes the stem cells and then returns the
blood to the patient. Leukapheresis usually takes 3 or 4 hours to complete. The
stem cells may or may not be treated with drugs to kill any cancer cells. The stem
cells then are stored until they are transplanted back into the patient.
CML. Treatment
HLA (human leukocyte antigen) typing of all patients under age 60, as well as
typing of siblings, parents, and children, if available. This procedure will determine
whether a compatible donor is available for stem cell transplantation.
Pre-treatment fertility measures (e.g., cryopreservation of semen prior to
treatment; completion of a pregnancy prior to treatment) in young patients who
have not completed their families.
Interferon-alpha (INF-a) therapy
Chemotherapy with drugs such as hydroxyurea (Hydrea®), busulfan
(Myleran®) or imatinib mesylate (Gleevec™).
In general, CML treatment options are divided into 2 groups:
- those that do not increase survival
- and those that do.
CML. Prognosis
The prognosis of CML depends on a number of different parameters. Two
different scoring systems are in use: one by Sokal et al (1984) and one by Hasford
et al (1998).
In the past, median survival was 3-4 years. With interferon-based therapy, this
was increased to 5-6 years.
Chronic lymphocytic leukemia (CLL)
is a type of leukemia in which too many lymphocytes are produced. Although the
malignant lymphocytes in CLL may look normal and mature, they are not and
these cells may not cope effectively with infection.
CLL is the most common form of leukemia in adults. Men are twice as likely to
develop CLL as women. However, the key risk factor is age. Over 75% of new
cases are diagnosed in patients over age 50. More than 7,000 new cases of CLL are
diagnosed in the U.S. each year.
CLL. Essentials of diagnosis.
Most patients asymptomatic at presentation
Splenomegaly typical
Lymphocytosis > 5000/l
Mature appearance of lymphocytes
Co-expression of CD19, CD5
Peripheral blood smear showing CLL cells
This is a microscopic view of bone marrow from a person with chronic
lymphocytic leukemia; it shows predominantly small, mature lymphocytes
The Rai or Binet staging systems
These systems consider:
The elevation of blood and marrow lymphocyte counts;
The size and distribution of lymph nodes;
The
spleen size;
The degree of anemia and the extent of the decrease of the blood platelet count.
The Rai staging system
O stage – lymphocytosis only
I stage - lymphocytosis +lymphadenopathy
II stage - organomegaly
III stage - anemia
IV stage - trombocytopenia
The Binet staging system
A – lymphadenopathy in less than 3 areas
B – lymphadenopathy in more than 3 areas
C – anemia, trombocytopenia
CLL. Treatment
Indications for treatment are:
falling hemoglobin or platelet count
progression to a later stage of disease
painful, disease-related overgrowth of lymph nodes or spleen
lymphocyte doubling time (an indicator of lymphocyte reproduction) of fewer
than 12 months
CLL. Treatment
CLL treatment focuses on controlling the disease and its symptoms rather than on
an outright cure. CLL is treated by chemotherapy, radiation therapy, biological
therapy, or bone marrow transplantation. Symptoms are sometimes treated
surgically (splenectomy removal of enlarged spleen) or by radiation therapy ("debulking" swollen lymph nodes).
oThe
myeloproliferative diseases ("MPD"s) are a group of diseases of the bone
marrow in which excess cells are produced. They are related to, and may evolve
into, myelodysplastic syndrome and acute myeloid leukemia, although the
myeloproliferative diseases on the whole have a much better prognosis than these
conditions. The concept of myeloproliferative disease was first proposed in 1951
by the eminent hematologist William Dameshek. The myeloproliferative diseases
are:
•Chronic myelogenous leukemia (CML)
•Polycythemia vera (PCV)
•Essential thrombocytosis (ET)
•Myelofibrosis (increased connective tissue with decreased room for production of
normal blood cells).
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 9.
Multiple myeloma. Lymphomas
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. To give definition of the term “Multiple myeloma” (MM).
2. Etiology and pathogenesis of MM.
3. Clinic of MM.
4. Laboratory and instrumental diagnostic of MM.
5. Stage of MM.
6. Diagnostic criteria and MM.
7. Differential diagnostics of MM with Waldenström's Macroglobulinemia.
8. Treatment of MM.
9. The basic preparations for treatment of MM.
10. Radial therapy of MM.
Examples of tests
1. What is this multiple myeloma?
A. the lymphomas
B. the paraproteinaemias
C. the leukaemias
D. the haemolytic anaemia
2. Multiple myeloma is malignant proliferation of which cells in bone marrow?
A. Lymphocytes
B. Monocytes
C. Basophiles
D. Plasmatic cells
3. Name laboratory changes of Multiple myeloma asymptomatic stage.
A. increased ESR, leucocytosis, trombocytopenia
B. increased ESR, M-protein, proteinuria
C. never changes
D. leucocytosis, anaemia
4. Which symptoms will be present in case of effected bones in patients with Multiple myeloma?
A. Bone pain
B. neoplasm
C. Fracture
D. All named above
5. What could you see on bone marrow aspirate or trephine biopsy?
A. Leucocytes infiltration
B. Plasma cell infiltration
C. T-lymphocyte infiltration
D. B- lymphocyte infiltration
Answers to tests:
1. B, 2. D, 3. B, 4. D, 5. B
References.
1. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002.
2. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 6, section 2, Chapter 105, 106.
3. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Multiple Myeloma(Myelomatosis; Plasma Cell Myeloma)
Multiple myeloma is a cancer of plasma cells that produce monoclonal immunoglobulin
and invade and destroy adjacent bone tissue. Common manifestations include bone pain, renal
insufficiency, hypercalcemia, anemia, and recurrent infections. Diagnosis requires demonstration
of M-protein (sometimes present in urine and not serum) and either lytic bone lesions, lightchain proteinuria, or excessive marrow plasma cells. A bone marrow biopsy is usually needed.
Specific treatment includes conventional chemotherapy with the addition of bortezomib,
lenalidomide, thalidomide, corticosteroids, and high-dose melphalan followed by autologous
peripheral blood stem cell transplantation.
The incidence of multiple myeloma is 2 to 4/100,000. Male:female ratio is 1.6:1, and the
median age is about 65 yr. Prevalence in blacks is twice that in whites. Etiology is unknown,
although chromosomal and genetic factors, radiation, and chemicals have been suggested.
Pathophysiology
The M-protein produced by the malignant plasma cells is IgG in about 55% of myeloma
patients and IgA in about 20%; of patients producing either IgG or IgA, 40% also have Bence
Jones proteinuria, which is free monoclonal κ or λ light chains in the urine. In 15 to 20% of
patients, plasma cells secrete only Bence Jones protein. IgD myeloma accounts for about 1% of
cases.
Diffuse osteoporosis or discrete osteolytic lesions develop, usually in the pelvis, spine, ribs,
and skull. Lesions are caused by bone replacement by expanding plasmacytomas or by cytokines
that are secreted by malignant plasma cells that activate osteoclasts and suppress osteoblasts. The
osteolytic lesions are usually multiple; occasionally, they are solitary intramedullary masses.
Enhanced bone loss may also lead to hypercalcemia. Extraosseous solitary plasmacytomas are
unusual but may occur in any tissue, especially in the upper respiratory tract.
Renal failure (myeloma kidney) occurs in many patients at diagnosis or during the course
of the disorder due to many causes, most commonly from deposition of light chains in the distal
tubules and hypercalcemia. Patients also often develop anemia usually from kidney disease or
suppression of erythropoiesis by cancer cells.
Susceptibility to bacterial infection may occur in some patients. Viral infections, especially
herpetic infections, are increasingly occurring as a result of newer treatment modalities.
Secondary amyloidosis (see Amyloidosis: Secondary amyloidosis (AA)) occurs in 10% of
myeloma patients, most often in patients with Bence Jones proteinuria of λ-type.
Variant expressions of multiple myeloma occur: Plasma Cell Disorders: Variant
Expressions of Multiple Myeloma ).
Symptoms and Signs
Persistent bone pain (especially in the back or thorax), renal failure, and recurring bacterial
infections are the most common problems on presentation, but many patients are identified when
routine laboratory tests show an elevated total protein level in the blood or show proteinuria.
Pathologic fractures are common, and vertebral collapse may lead to spinal cord compression
and paraplegia. Symptoms of anemia predominate or may be the sole reason for evaluation in
some patients, and a few patients have manifestations of hyperviscosity syndrome (see Plasma
Cell Disorders: Symptoms and Signs). Peripheral neuropathy, carpal tunnel syndrome, abnormal
bleeding, and symptoms of hypercalcemia (eg, polydipsia) are common. Patients may also
present with renal failure. Lymphadenopathy and hepatosplenomegaly are unusual.
Diagnosis
• CBC with platelets, peripheral blood smear, ESR, chemistry panel (BUN, creatinine, Ca,
uric acid, LDH)
• Serum and urine protein electrophoresis, followed by immunofixation
• X-rays (skeletal survey)
• Bone marrow examination
Multiple myeloma is suspected in patients > 40 yr with persistent unexplained bone pain,
particularly at night or at rest, other typical symptoms, or unexplained laboratory abnormalities,
such as elevated blood protein or urinary protein, hypercalcemia, renal insufficiency, or anemia.
Laboratory evaluation includes routine blood tests, protein electrophoresis, x-rays, and bone
marrow examination.
Routine blood tests include CBC, ESR, and chemistry panel. Anemia is present in 80% of
patients, usually normocytic-normochromic anemia with formation of rouleau, which are clusters
of 3 to 12 RBCs that occur in stacks. WBC and platelet counts are usually normal. ESR usually
is > 100 mm/h; BUN, serum creatinine, LDH, and serum uric acid are frequently elevated. Anion
gap is sometimes low. Hypercalcemia is present at diagnosis in about 10% of patients.
Protein electrophoresis is done on a serum sample and on a urine sample concentrated from
a 24-h collection to quantify the amount of urinary M-protein. Serum electrophoresis identifies
M-protein in about 80 to 90% of patients. The remaining 10 to 20% are usually patients with
only free monoclonal light chains (Bence Jones protein) or IgD. They almost always have Mprotein detected by urine protein electrophoresis. Immunofixation electrophoresis can identify
the immunoglobulin class of the M-protein and can often detect light-chain protein if the serum
immunoelectrophoresis is falsely negative; immunofixation electrophoresis is done even if the
serum test is negative if multiple myeloma is strongly suspected. Light-chain analysis with
delineation of κ and λ ratios helps confirm the diagnosis. Light-chain analysis can also be used to
follow efficacy of therapy and provide prognostic data. Serum level of β2-microglobulin is
measured if diagnosis is confirmed or very likely; it frequently is elevated, and albumin may be
decreased. A new international staging system uses the levels of serum albumin and β2microglobulin to indicate severity of disease and subsequent prognosis.
X-rays include a skeletal survey. Punched-out lytic lesions or diffuse osteoporosis is
present in 80% of cases. Radionuclide bone scans usually are not helpful. MRI can provide more
detail and is obtained if specific sites of pain or neurologic symptoms are present.
Bone marrow aspiration and biopsy are done and reveal sheets or clusters of plasma cells;
myeloma is diagnosed when > 10% of the cells are of this type. However, marrow involvement
is patchy; therefore, some samples from patients with myeloma may show < 10% plasma cells.
Still, the number of marrow plasma cells is rarely normal. Plasma cell morphology does not
correlate with the class of immunoglobulin synthesized. Chromosomal studies on bone marrow
may reveal specific karyotypic abnormalities in plasma cells associated with differences in
survival.
In patients without serum M protein, myeloma is indicated by Bence Jones proteinuria >
300 mg/24 h, osteolytic lesions (without evidence of metastatic cancer or granulomatous
disease), and sheets or clusters of marrow plasma cells.
Prognosis
The disease is progressive and incurable, but median survival has recently improved to > 5
yr as a result of advances in treatment. Unfavorable prognostic signs at diagnosis are lower
serum albumin and higher β2-microglobulin levels. Patients presenting with renal failure also do
poorly unless kidney function improves with therapy.
Because multiple myeloma is ultimately fatal, patients are likely to benefit from
discussions of end-of-life care that involve their doctors and appropriate family and friends.
Points for discussion may include advance directives, the use of feeding tubes, and pain relief.
Treatment
• Chemotherapy for symptomatic patients
• Thalidomide SOME TRADE NAMES THALOMID , bortezomib SOME TRADE
NAMES VELCADE , or lenalidomide with corticosteroids and/or chemotherapy
• Possibly maintenance therapy
• Possibly stem cell transplantation
• Possibly radiation therapy
• Treatment of complications (anemia, hypercalcemia, renal insufficiency, infections,
skeletal lesions)
Treatment of myeloma has improved in the past decade, and long-term survival is a
reasonable therapeutic target. Therapy involves direct treatment of malignant cells in
symptomatic patients and the treatment of the complications. Asymptomatic patients probably do
not benefit from treatment, which is usually withheld until symptoms or complications develop.
However, patients with evidence of lytic lesions or bone loss (osteopenia or osteoporosis) should
be treated with monthly infusions of zoledronic acid SOME TRADE NAMES
ZOMETA or pamidronate SOME TRADE NAMES AREDIA to reduce the risk of skeletal
complications.
Treatment of malignant cells: Until recently, conventional chemotherapy consisted only of
oral melphalan SOME TRADE NAMES ALKERAN and prednisone SOME TRADE NAMES
DELTASONE given in cycles of 4 to 6 wk with monthly evaluation of response. Recent studies
show superior outcome with the addition of either bortezomib SOME TRADE NAMES
VELCADE or thalidomide SOME TRADE NAMES THALOMID . Other chemotherapeutic
drugs, including other alkylating drugs (eg, cyclophosphamide SOME TRADE NAMES
CYTOXAN, doxorubicin SOME TRADE NAMES ADRIAMYCIN and its newer analog
liposomal pegylated doxorubicin SOME TRADE NAMES ADRIAMYCIN ) also are more
effective when combined with thalidomide SOME TRADE NAMES THALOMID or
bortezomib SOME TRADE NAMES VELCADE . Many other patients are effectively treated
with bortezomib SOME TRADE NAMES VELCADE , thalidomide SOME TRADE NAMES
THALOMID , or lenalidomide plus glucocorticoids and/or chemotherapy.
Chemotherapy response is indicated by decreases in serum or urine M-protein, increases in
RBCs, and improvement in renal function among patients presenting with kidney failure.
Autologous peripheral blood stem cell transplantation may be considered for patients who
have adequate cardiac, hepatic, pulmonary, and renal function, particularly those whose disease
is stable or responsive after several cycles of initial therapy. Allogeneic stem cell transplantation
after non-myeloablative chemotherapy (eg, low-dose cyclophosphamide SOME TRADE
NAMES CYTOXAN and fludarabine SOME TRADE NAMES FLUDARA ) or low-dose
radiation therapy can produce myeloma-free survival of 5 to 10 yr in some patients. However,
allogeneic stem cell transplantation remains experimental because of the high morbidity and
mortality from graft vs. host disease.
In relapsed or refractory myeloma, combinations of bortezomib SOME TRADE NAMES
VELCADE , thalidomide SOME TRADE NAMES THALOMID, or its newer analog
lenalidomide with chemotherapy or corticosteroids may be used. These drugs are usually
combined with other effective drugs that the patient has not yet been treated with, although
patients with prolonged remissions may respond to retreatment with the same regimen that led to
the remission.
Maintenance therapy has been tried with nonchemotherapeutic drugs, including interferonα, which prolongs remission but does not improve survival and is associated with significant
adverse effects. Following a response to corticosteroid-based regimens, corticosteroids alone are
effective as a maintenance treatment. Thalidomide SOME TRADE NAMES THALOMID may
also be effective as a maintenance treatment, and studies are evaluating maintenance therapy
with bortezomib SOME TRADE NAMES VELCADE and lenalidomide among patients who
have responded to these drugs alone or in combination therapeutic regimens.
Treatment of complications: In addition to direct treatment of malignant cells, therapy must
also be directed at complications, which include anemia, hypercalcemia, renal insufficiency,
infections, and skeletal lesions.
Anemia can be treated with recombinant erythropoietin (40,000 units sc q wk) in patients
whose anemia is inadequately relieved by chemotherapy. If anemia produces cardiovascular or
significant systemic symptoms, packed RBCs are transfused. Plasmapheresis is indicated if
hyperviscosity develops (see Plasma Cell Disorders: Symptoms and Signs).
Hypercalcemia is treated with saluresis, IV bisphosphonates, and sometimes with
prednisone SOME TRADE NAMES DELTASONE . Most patients do not require allopurinol
SOME TRADE NAMES ZYLOPRIM . However, allopurinol SOME TRADE NAMES
ZYLOPRIM is indicated for patients with high levels of serum uric acid or high tumor burden
and a high risk of tumor lysis syndrome with treatment.
Renal compromise can be ameliorated with adequate hydration. Even patients with
prolonged, massive Bence Jones proteinuria (≥ 10 to 30 g/day) may have intact renal function if
they maintain urine output > 2000 mL/day. Dehydration combined with high-osmolar IV
contrast may precipitate acute oliguric renal failure in patients with Bence Jones proteinuria.
Infection is more likely during chemotherapy-induced neutropenia. In addition, infections
with the herpes zoster virus are occurring more frequently in patients treated with newer
antimyeloma drugs. Documented bacterial infections should be treated with antibiotics; however,
prophylactic use of antibiotics is not routinely recommended. Prophylactic use of antiviral drugs
may be indicated for patients receiving specific drugs. Prophylactic IV immune globulin may
reduce the risk of infection but is generally reserved for patients with recurring infections.
Pneumococcal and influenza vaccines are indicated to prevent infection.
Skeletal lesions require multiple supportive measures. Maintenance of ambulation and
supplemental Ca and vitamin D help preserve bone density. Analgesics and palliative doses of
radiation therapy (18 to 24 Gy) can relieve bone pain. However, radiation therapy may impair
the patient's ability to receive cytotoxic doses of systemic chemotherapy. Most patients,
especially those with lytic lesions and generalized osteoporosis or osteopenia, should receive a
monthly IV bisphosphonate (either pamidronate SOME TRADE NAMES AREDIA or
zoledronic acid SOME TRADE NAMES ZOMETA). Bisphosphonates reduce skeletal
complications and lessen bone pain and may have an antitumor effect.
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate
Methodological Instruction to Lesson № 10.
Bleeding Disorder (Hemorrhagic diathesis)
Hours: 5.
Working place: classroom, hospital wards.
Questions.
1. To give definition of the term “Hemorrhagic diathesis” (HD).
2. Classification of HD.
3. Homeostasis system and it physiology.
4. Types of a bleeding at HD.
5. Diagnostic criteria of Hemophilia.
6. Treatment and preventive maintenance of Hemophilia.
7. Diagnostic criteria of Willebrand's Disease.
8. Diagnostic criteria of Thrombocytopenic purpura.
9. Treatment of Werlhof’s disease.
10. Diagnostic criteria of Thrombocytopathy and Glanzmann's disease.
11. Variants of hemorrhagic vasculitis and clinic depending on variant of illness.
12. Differential diagnostics of hemorrhagic vasculitis.
13. Diagnostic criteria of Rendu-Osler-Weber Syndrome.
Examples of tests
1. The hemorrhagic diathesis which are caused by changes of abnormal blood
vessels is all but one:
a. Henoch-Schönlein Purpura
d. Hemorrhagic vasculitis
b. Rendu-Osler-Weber Syndrome
e. Willebrand's Disease
c. Hemangioma
2. The hematomic type of hemorrhagic is at:
a. Hemorrhagic vasculitis
d. Hemophilia
b. Werlhof’s disease
e. Glanzmann's disease
c. Hemorrhagic telangiectasia
3. The petechialic type of hemorrhagic is at:
a. Thrombocytopenic and thrombocytopathy
b. Rendu-Osler-Weber Syndrome
c. Hemorrhagic vasculitis
d. Hemophilia
e. Werlhof’s disease
4. The patient 35 years during 5 years has nasal bleeding, ecchymosis on a skin.
Two weeks back after nasal of a bleeding there was a weakness, faint. The patient
has pallor, ecchymosis on a skin. The analysis of blood: er. – 4.2*1012/l, Hb – 90
g/l, chromatic parameter – 0.7, L. – 6.4* 109/l, stab n.- 3%, seg. – 67%, e. – 2%, l.
– 23%, m – 5%, thrombocytes – 10*109/l , ESR – 15mm/ hour. With is diagnosis
at the patient?
a. Aplastic anemia
d. Iron deficiency Anemias
b. Hemorrhagic vasculitis
e. Thrombocytopenic purpura
c. Hemophilia
References.
4. Davidson’s Principles and practice of medicine (nineteenth
edition)/Christopher Haslett, Edvin R. Chilvers and others. –
Edinburgh, 2002.
5. Harrisons Principle if internal medicine (seventeenth Edition)/Fauci,
Braunwald, Hasper and other. – Part 6, section 2, Chapter 109, 110.
6. The Merck Manual of Diagnosis and Therapy (seventeenth Edition)/
Robert Berkow, Andrew J. Fletcher and others. – published by Merck
Research Laboratories, 1999.
Short theoretic material
Classification of hemorrhagic diathesis
Thrombocytopenia and platelet dysfunction:
Idiopatic thrombocytopenic purpura (ITP);
Thrombocytopenia other causes;
Thrombocytopenia due splenic sequestration;
Thrombotic thrombocytopenic purpura (TTP);
Hemolitic uremic syndrom (HUS);
Hereditary disorders of platelet function
Coagulation disorders:
Circulating anticoagulants;
Disseminated intravascular coagulation (DIC);
Hemophilia;
Uncomon hereditary coagulation disorders
Bleeding due to abnormal blood vessels:
Autoerythrocyte sensitization;
Disprteinemias causing vascular purpura;
Hereditary hemorrhagic teleangiectasia;
Purpura simplex;
Senile purpura
Unusual or excessive bleeding includes unexplained nosebleeds (epistaxis),
excessive or prolonged menstrual blood loss (menorrhagia), prolonged
bleeding after minor cuts or trauma, easy bruising into tissues (ecchymoses)
or skin (petechial or purpuric lesions), and unexplained gingival bleeding
after tooth brushing;
Systemic bleeding can result from defects in blood vessels (connective tissue
diseases, vitamin C deficiency, hereditary hemorrhagic telangiectasia) or,
more commonly, quantitative or qualitative disorders of platelets or of
coagulation.
Etiology and Pathophysiology of Thrombocytopenia
Platelets are cell fragments that function in the clotting system.
Thrombopoietin, primarily produced in the liver in response to
decreased numbers of marrow megakaryocytes and circulating
platelets, stimulates the bone marrow to synthesize platelets from
megakaryocytes. Platelets circulate for 7 to 10 days. About 1⁄3 are
always transiently sequestered in the spleen. red in the spleen. The
platelet count is normally 140,000 to 440,000/μL.
The risk of bleeding is inversely proportional to the platelet count.
When the platelet count is < 50,000/μL, minor bleeding occurs easily
and the risk of major bleeding increases. Counts between 20,000 and
50,000/μL predispose to bleeding with trauma, even minor trauma;
with counts < 20,000/μL, spontaneous bleeding may occur; with
counts < 5000/μL, severe spontaneous bleeding is more likely.
However, patients with counts < 10,000/μL may be asymptomatic for
years.
Symptoms and Signs
Platelet disorders result in a typical pattern of bleeding: multiple petechiae in
the skin, typically most evident on the lower legs; scattered small ecchymoses
at sites of minor trauma; mucosal bleeding (epistaxis, bleeding in the GI and
GU tracts, vaginal bleeding); and excessive bleeding after surgery. Heavy GI
bleeding and bleeding into the CNS may be life threatening. However, massive
bleeding into tissues (eg, deep visceral hematomas or hemarthroses) does not
commonly occur and suggests a coagulation disorder (hemophilia).
Treatment
In patients with thrombocytopenia or platelet dysfunction, drugs that
further impair platelet function should be avoided, particularly aspirin
and other NSAIDs.
Patients may require platelet transfusion, but only in limited situations.
Prophylactic transfusions are used sparingly because they may lose their
effectiveness with repeated use due to the development of platelet
alloantibodies.
In platelet dysfunction or thrombocytopenia caused by decreased
production, transfusions are reserved for active bleeding or severe
thrombocytopenia (eg, platelet count < 10,000/μL). In thrombocytopenia
caused by platelet destruction, transfusions are reserved for lifethreatening or CNS bleeding.
Hereditary Intrinsic Platelet Disorders Von Willebrand's Disease
Von Willebrand's disease is a hereditary deficiency of von Willebrand's
factor (VWF), which causes platelet dysfunction.
Von Willebrand's factor (VWF) is synthesized and secreted by vascular
endothelium to form part of the perivascular matrix. VWF promotes the
platelet adhesion phase of hemostasis by binding with a receptor on the
platelet surface membrane (glycoprotein Ib-IX), which connects the platelets
to the vessel wall. VWF is also required to maintain normal plasma factor
VIII levels.
Disorders of amplification of platelet activation are the most common
hereditary intrinsic platelet disorders and produce mild bleeding. They may
result from decreased of adenosine diphosphate in the platelet granules
(storage pool deficiency), from an inability to generate thromboxane A2
from arachidonic acid, or from an inability of platelets to aggregate in
response to thromboxane A2.
Thrombasthenia (Glanzmann's disease) is a rare autosomal recessive
disorder producing a defect in the platelet glycoprotein IIb-IIIa complex;
platelets cannot aggregate. Patients may experience severe mucosal bleeding
(eg, nosebleeds that stop only after nasal packing and transfusions of platelet
concentrates).
Bernard-Soulier syndrome is another rare autosomal recessive disorder. It
impairs platelet adhesion via a defect in the glycoprotein Ib-IX complex.
Bleeding may be severe. Platelets are unusually large. They do not aggregate
with ristocetin but aggregate normally with ADP, collagen, and epinephrine.
Large platelets associated with functional abnormalities also occur in the
May-Hegglin anomaly, a thrombocytopenic disorder with abnormal WBCs,
and in the Chédiak-Higashi syndrome
Symptoms and Signs of Von Willebrand's Disease
Bleeding manifestations are mild to moderate and include easy bruising;
bleeding from small skin cuts that may stop and start over hours; sometimes,
increased menstrual bleeding; and abnormal bleeding after surgical procedures
(eg, tooth extraction, tonsillectomy).
Diagnosis of Von Willebrand's Disease
VWD is suspected in patients with bleeding disorders, particularly those
with a family history of the disorder.
Definitive diagnosis requires measuring total plasma VWF antigen; VWF
function, as determined by the ability of the plasma to support
agglutination of normal platelets by ristocetin (ristocetin cofactor
activity); and plasma factor VIII level.
Treatment of Von Willebrand's Disease
Patients are treated only if they are actively bleeding or are undergoing
an invasive procedure (surgery, dental extraction).
Treatment involves replacement of VWF by infusion of pasteurized
intermediate-purity factor VIII concentrates which contain components
of VWF. These concentrates are virally inactivated and therefore do not
transmit HIV infection or hepatitis. Because they do not cause
transfusion-transmitted infections, these concentrates are preferred to the
previously common use of cryoprecipitate.
High-purity factor VIII concentrates are prepared by immunoaffinity
chromatography and contain no VWF.
Idiopathic Thrombocytopenic Purpura (ITP)
Idiopathic (immunologic) thrombocytopenic purpura is a bleeding
disorder caused by thrombocytopenia not associated with a systemic
disease. Typically, it is chronic in adults but is usually acute and selflimited in children. Spleen size is normal. Diagnosis requires that other
disorders be excluded through selective tests.
Idiopathic thrombocytopenic purpura (ITP) usually results from
development of an antibody directed against a structural platelet antigen
(an autoantibody). In childhood ITP the autoantibody may be triggered
by binding of viral antigen to megakaryocytes.
Symptoms, Signs, and Diagnosis
spleen is of normal size unless it is enlarged by a coexistent childhood viral
infection.
ITP is suspected in patients with unexplained thrombocytopenia. Peripheral
blood is normal except for reduced platelet numbers.
Bone marrow is examined if blood counts or blood smear reveals
abnormalities in addition to thrombocytopenia. Bone marrow examination
reveals normal or possibly increased numbers of megakaryocytes in an
otherwise normal marrow.
Because diagnostic findings are nonspecific, diagnosis requires exclusion of
other thrombocytopenic disorders suggested by clinical or laboratory test
data.
Because HIV-associated thrombocytopenia may be otherwise
indistinguishable from ITP, HIV testing is performed if the patient has risk
factors for HIV infection.
Treatment includes of ITR
Corticosteroids (prednisone 1 mg/kg once/day) initially. In the patient who
responds, the platelet count rises to normal within 2 to 6 wk).
Splenectomy (can achieve a remission in about 2⁄3 of these patients),
Immunosuppressive
treatment
(cyclophosphamide,
azathioprine,
rituximab),
Platelet transfusions,
IV immune globulin. In a child or adult with ITP and life-threatening
bleeding, rapid phagocytic blockade is attempted by giving IV immune
globulin 1 g/kg once/day for 1 to 2 days. This usually causes the platelet
count to rise within 2 to 4 days but only for 2 to 4 wk.
Thrombocytopenia: Other Causes
Acute respiratory distress syndrome
Blood transfusions
Connective tissue and lymphoproliferative disorders
Drug-induced immunologic destruction (Quinidine, sulfa preparations,
carbamazepine, methyldopa, aspirin, oral antidiabetic drugs, gold salts, and
rifampin, heparin)
Gram-negative sepsis
HIV
Thrombocytopenia Due to Splenic Sequestration
Increased splenic platelet sequestration can occur in various disorders that
produce splenomegaly. Sequestration is expected in patients with congestive
splenomegaly caused by advanced cirrhosis. The platelet count usually is >
30,000/μL unless the disorder producing the splenomegaly also impairs platelet
production (eg, in myelofibrosis with myeloid metaplasia).
Thrombotic Thrombocytopenic Purpura (TTP) and Hemolytic-Uremic
Syndrome (HUS)
unexplained thrombocytopenia and microangiopathic hemolytic anemia are
sufficient evidence for a presumptive diagnosis.
TTP-HUS is suspected in patients with suggestive symptoms,
thrombocytopenia, and anemia. If the disease is suspected, urinalysis,
peripheral blood smear, reticulocyte count, serum LDH, renal functions,
serum bilirubin (direct and indirect), and Coombs' test are obtained. The
diagnosis is suggested by thrombocytopenia and anemia, with fragmented
RBCs on the blood smear (helmet cells, triangular-shaped RBCs, distortedappearing RBCs-these changes describe microangiopathic hemolysis);
evidence of hemolysis (falling Hb level, polychromasia, elevated
reticulocyte count, elevated serum LDH); and negative direct antiglobulin
(Coombs') test.
Prognosis and Treatment
Epidemic HUS in children associated with enterohemorrhagic infection
usually spontaneously remits and is treated with supportive care and not
plasma exchange. In other cases, untreated TTP-HUS is almost always fatal.
With plasma exchange, however, about 85% of patients recover completely.
Plasma exchange is continued daily until evidence of disease activity has
subsided, which may be several days to many weeks
Corticosteroids and antiplatelet drugs (aspirin) have also been used but are
controversial.
Coagulation Disorders Caused by Circulating Anticoagulants (CA)
CA are usually autoantibodies that neutralize specific clotting factors in vivo
(autoantibody against factor VIII or factor V) or inhibit protein-bound
phospholipid in vitro;
antibodies bind to prothrombin-phospholipid complexes, inducing
hypoprothrombinemia; these patients may bleed excessively;
Factor VIII autoantibodies also arise occasionally in nonhemophilic patients,
eg, in a postpartum woman as a manifestation of underlying systemic
autoimmune disease or in elderly patients without overt evidence of other
underlying disease. Patients with a factor VIII anticoagulant can develop
life-threatening hemorrhage.
Therapy with cyclophosphamide and corticosteroids may suppress
autoantibody production in patients without hemophilia.
Disseminated Intravascular Coagulation(DIC) (Consumption Coagulopathy;
Defibrination Syndrome)
DIC involves abnormal, excessive generation of thrombin and fibrin in the
circulating blood. During the process, increased platelet aggregation and
coagulation factor consumption occur. DIC that evolves slowly (over weeks or
months) causes primarily venous thrombotic and embolic manifestations; DIC
that evolves rapidly (over hours or days) causes primarily bleeding.
Etiology and Pathophysiology of DIC
Complications of obstetrics—eg, abruptio placentae, saline-induced
therapeutic abortion, retained dead fetus or products of conception, or
amniotic fluid embolism.
Infection, particularly with gram-negative organisms.
Malignancy, particularly mucin-secreting adenocarcinomas of the
pancreas and prostate and acute promyelocytic leukemia.
Shock from any cause.
severe tissue damage from head trauma, burns, frostbite, or gunshot
wounds; complications of prostate surgery;
venomous snake bites in which enzymes enter the circulation that
activate one or several coagulation factors and generate thrombin or
directly convert fibrinogen to fibrin;
profound intravascular hemolysis;
aortic aneurysms or cavernous hemangiomas (Kasabach-Merritt
syndrome) associated with vessel wall damage and areas of blood stasis.
Symptoms and Signs of DIC
In slowly evolving DIC, symptoms of venous thrombosis and pulmonary
embolism may be present.
In severe, rapidly evolving DIC, skin puncture sites (eg, IV or arterial
punctures) bleed persistently, ecchymoses form at sites of parenteral
injections, and serious GI bleeding may occur. Delayed dissolution of fibrin
polymers by fibrinolysis may result in the mechanical disruption of RBCs
and mild intravascular hemolysis. Occasionally, microvascular thrombosis
and hemorrhagic necrosis produce dysfunction and failure in multiple
organs.
Diagnosis of DIC
decreasing plasma fibrinogen;
increased plasma d-dimer (an indication of in vivo fibrin deposition and
degradation);
thrombocytopenia, a normal to minimally prolonged PT (results are
typically reported as INR);
factor VIII is reduced in DIC because of the thrombin-induced generation
of activated protein C, which proteolyses factor VIII.
Treatment of DIC
Immediate correction of the underlying cause is the priority (eg, broadspectrum antibiotic treatment of suspected gram-negative sepsis, evacuation
of the uterus in abruptio placentae).
If treatment is effective, DIC should subside quickly. If bleeding is severe,
adjunctive eplacement therapy is indicated, consisting of platelet
oncentrates to correct thrombocytopenia;
cryoprecipitate to replace fibrinogen and factor VIII;
and fresh frozen plasma to increase levels of other clotting factors and
natural anticoagulants (antithrombin, proteins C and S).
Hemophilia
Hemophilias are common hereditary bleeding disorders caused by
deficiencies of either clotting factor VIII or IX.
Hemophilia A (factor VIII deficiency), which affects about 80% of
hemophilic patients, and hemophilia B (factor IX deficiency) have
identical clinical manifestations, screening test abnormalities, and Xlinked genetic transmission.
Because these genes are located on the X chromosome, hemophilia
affects males almost exclusively. Daughters of hemophilic males are
obligate carriers, but sons are normal. Each son of a carrier has a 50%
chance of having hemophilia, and each daughter has a 50% chance of
being a carrier.
Diagnosis
Patients with hemophilia bleed into tissues (eg, hemarthroses, muscle
hematomas, retroperitoneal hemorrhage), and the bleeding may be
delayed after trauma. Hemarthroses can lead to synovitis and arthropathy
family history
PTT is prolonged, but the PT and platelet count are normal.
Decrease of Factor VIII and IX.
Prevention and Treatment
should avoid aspirin and NSAIDs. The COX-2 inhibitors have little
antiplatelet activity, may produce fewer GI erosions than aspirin or other
NSAIDs, and can be used with caution in hemophilia.
To avoid surgical operations. Drugs should be given orally or IV.
In hemophilia A, factor VIII.
In hemophilia B, factor IX.
Desmopressin (SOME TRADE NAMES DDAVP, STIMATE) may
temporarily raise factor VIII levels.
An antifibrinolytic agent (ε- aminocaproic acid SOME TRADE NAMES
AMICAR 2.5 to 4 g po qid for 1 wk or tranexamic acid SOME TRADE
NAMES CYKLOKAPRON 1.0 to 1.5 g po tid or qid for 1 wk) should be
given to prevent late bleeding after dental extraction or other
oropharyngeal mucosal trauma (tongue laceration).
BLEEDING DUE TO ABNORMAL BLOOD VESSELS
Bleeding may result from abnormalities in platelets, coagulation factors, or
blood vessels. Vascular bleeding disorders are caused by defects in blood
vessels, typically producing petechiae, purpura, and bruising but seldom leading
to serious blood loss. Bleeding may result from deficiencies of vascular and
perivascular collagen in Ehlers-Danlos syndrome and in other rare hereditary
connective tissue disorders (pseudoxanthoma elasticum, osteogenesis
imperfecta, Marfan syndrome). Hemorrhage may be a prominent feature of
scurvy or of Henoch-Schönlein purpura, a hypersensitivity vasculitis common
during childhood. In vascular bleeding disorders, tests of hemostasis are usually
normal. Diagnosis is clinical.
Henoch-Schönlein Purpura (HSP)
Henoch-Schönlein purpura is vasculitis that affects primarily small vessels.
It occurs most often in children.
Common manifestations include palpable purpura, arthralgias, GI
symptoms and signs, and glomerulonephritis.
Diagnosis is clinical in children but usually warrants biopsy in adults.
Disease is usually self-limited.
Corticosteroids can relieve arthralgias and GI symptoms but do not alter the
course of the disease. Progressive glomerulonephritis may require highdose corticosteroids and cyclophosphamide.
Symptoms and Signs of HSP
The disease begins with a sudden palpable purpuric rash typically occurring
on the feet, legs, and arms and as a strip across the buttocks. The purpura
may start as small areas of urticaria that become indurated and palpable.
Crops of new lesions may appear over days to several weeks. Many patients
also have fever and polyarthralgia with periarticular tenderness and swelling
of the ankles, knees, hips, wrists, and elbows.
GI symptoms are common and include colicky abdominal pain, abdominal
tenderness, and melena.
Symptoms usually remit after about 4 wk. In most patients, the disorder
subsides without serious sequelae; however, some patients develop chronic
renal failure.
Diagnosis of HSP
Biopsy of skin lesions
The diagnosis is suspected in patients, particularly children, with typical skin
findings. It is confirmed by biopsy of skin lesions when leukocytoclastic
vasculitis with IgA in the vessel walls is identified.
Urinalysis is done; hematuria, proteinuria, and RBC casts indicate renal
involvement.
If renal function is deteriorating, renal biopsy may help define the prognosis.
Diffuse glomerular involvement or crescent formation in most glomeruli
predicts progressive renal failure.
Treatment of HSP
treatment is symptomatic. Corticosteroids (prednisone 2 mg/kg up to a total of
50 mg po once/day) may help control abdominal pain and are occasionally
needed to treat severe joint pain or renal disease. Pulse IV methylprednisolone
followed by oral and cyclophosphamide can be given to attempt to control
inflammation when the kidneys are severely affected. However, the effects of
corticosteroids on renal manifestations are not clear.
Autoerythrocyte Sensitization (Gardner-Diamond Syndrome)
Autoerythrocyte sensitization is a rare disorder affecting women. It is
characterized by local pain and burning preceding painful ecchymoses
that occur primarily on the extremities.
In women with autoerythrocyte sensitization, intradermal injection of 0.1
mL of autologous RBCs or RBC stroma may result in pain, swelling, and
induration at the injection site.
Diagnosis is based on examination of the site of intradermal injection of
autologous RBCs and of a separate control injection site (without RBCs)
24 to 48 h after injection.
Dysproteinemias Causing Vascular Purpura
Amyloidosis causes amyloid deposition within vessels in the skin and
subcutaneous tissues, which may increase vascular fragility, producing purpura.
In some patients, coagulation factor X is adsorbed by amyloid and becomes
deficient, but this usually is not the cause of bleeding. Periorbital purpura or a
purpuric rash that develops in a nonthrombocytopenic patient after gentle
stroking of the skin suggests amyloidosis.
Hereditary Hemorrhagic Telangiectasia (Rendu-Osler-Weber Syndrome)
Hereditary hemorrhagic telangiectasia is a hereditary disease of
vascular malformation transmitted as an autosomal dominant trait
affecting men and women.
telangiectatic lesions on the face, lips, oral and nasal mucosa, and tips of
the fingers and toes.
Some patients have pulmonary arteriovenous fistulas. These fistulas may
produce significant right-to-left shunts, which can result in dyspnea,
fatigue, cyanosis, or polycythemia.
However, the first sign of their presence may be a brain abscess, transient
ischemic attack, or stroke as a result of infected or noninfected emboli.
Cerebral or spinal arteriovenous malformations occur in some families
and may cause subarachnoid hemorrhage, seizures, or paraplegia.
Treatment
Treatment for most patients is supportive, but accessible telangiectases (in
the nose or GI tract via endoscopy) may be treated with laser ablation.
Arteriovenous fistulas may be treated by surgical resection or
embolotherapy.
Iron therapy
Prepared by Orlovsky A. V., assistant, D.Ph.,
Murenets N. A., postgraduate