Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 1 of 6
I. Review from last lecture: When you are doing a tracheotomy on a child there is a good chance that you may poke
through the child’s trachea and damage the esophagus. Another point: the recurrent laryngeal nerve ascends into the
neck between the trachea and esophagus supplies both, but the esophagus is not midline in the neck…it deviates to
the left and in the thorax it passes back over to the midline. This means that surgically an approach to the esophagus
must be made in the cervical region…it is easiest to get to it from the left side because it projects from behind the
trachea to some degree.
II. Orbit [S1]
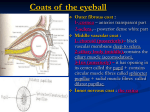
III. Bony Orbit [S2]
IV. Right Bony Orbit (Anterior View) [S3]
a. Begin with the osteology. This is the right orbit seen in anterior view.
b. The BONY ORBIT HAS FOUR MARGINS, which are formed by four bones --- frontal (above), zygomatic
(lateral), maxilla and lacrimal. Note the supraorbital and infraorbital foramina close to their respective margins.
i. Zygomatic and maxilla form the infraorbital margin.
ii. Maxilla and the lacrimal form the medial margin.
c. The bony orbit is described as being a FOUR-SIDED PYRAMID lying on its side.
i. The apex of the pyramid is posterior (in the region of the optic canal) and the base anterior from the four
margins that were just mentioned.
d. The orbit has a roof, floor, medial and lateral walls.
i. The ROOF of the pyramid is formed by the orbital plate of the frontal bone and lesser wing of the sphenoid.
The FLOOR principally by the maxilla, the LATERAL WALL by the zygomatic and greater wing of the
sphenoid and the MEDIAL WALL primarily by the orbital plate of the ethmoid (extremely thin, often referred
to as the “lamina papyracea”) and lacrimal bones.
ii. The roof, floor and medial wall are thin and easily broken.
1. The only wall that is not thin is the lateral wall.
e. Many FORAMINA communicate with the orbit.
i. The optic canal leads into the middle cranial fossa and transmits CN II and the ophthalmic a. into the orbit.
ii. The superior orbital fissure (between the lesser and greater wings) transmits CN III, IV, VI (eye muscles),
the V1 ophthalmic n. (three branches) and the ophthalmic vv. (which drain the orbit) leave the orbit through
the superior orbital fissure.
iii. The inf. orbital fissure (between the lateral wall and floor) transmits the infraorbital n., a. and v. and the
zygomatic n.
1. The infraorbital artery and vein run on the floor of the orbit, become bridged over by bone, and then
emerge on the face through the infraorbital foramen.
iv. The infraorbital n. and zygomatic n. are branches of V2—the maxillary nerve.
1. As soon as the maxillary nerve passes through this fissure, it becomes the infraorbital nerve.
2. The zygomatic nerve comes off more posterior of V2 and enters the orbit separately.
a. This nerve has a relationship to the lacrimal gland that we will discuss later.
v. The anterior and posterior ethmoidal foramina (near the junction of the roof and the medial wall) transmit
nerves and vessels of the same name out of the orbit. The ethmoidal nerves are branches of V1—the
ophthalmic nerve and the ethmoidal vessels are branches of the ophthalmic artery.
f. The fossa for the lacrimal sac lies within a depression in the lacrimal bone and partly in the maxilla.
g. [SQ]: Is “V2” referring to V2 of the trigeminal nerve? Yes.
h. [SQ]: Does V2 still go through the foramen rotundum? Yes. The V2 leaves the cranial cavity through the
foramen rotundum, but then enters a space behind the orbit called the pterygopalatine fossa and from there it
enters the orbit through the infraorbital fissure. It does not go from the foramen rotundum directly into the orbit.
V. Relationship of Bony Orbit (Coronal Section) [S4]
a. The RELATIONSHIPS OF THE ORBIT are shown well in this coronal section.
b. Several of the paranasal air sinuses (cavities within certain bones of the skull) are closely related to the orbit.
i. Superiorly the orbit is related to the frontal air sinus.
ii. Inferiorly it is related to the maxillary air sinus.
iii. Medially the orbit is related to both the ethmoid air cells (sinus) and the sphenoid air sinus (not shown).
c. These sinuses are all closely related to the orbit. With regard to the roof of the orbit, the orbital plate of the
frontal is quite thin. A pencil or other sharp object could easily penetrate the roof of the orbit and damage the
brain. This is how they used to do frontal lobotomies.
d. The floor of the orbit is very thin and related to the maxillary sinus. Fractures of the floor of the orbit ("blowout"
fractures—where the floor fractures and contents droop down to the sinus) can increase the pressure in the orbit
and break the floor, and result in the eyeball sinking into the maxillary sinus with subsequent impairment of the
extrinsic eye muscles causing misalignment. This leads to diplopia (double vision).
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 2 of 6
VI. Relationships of Bony Orbit (Horizontal Section) [S5]
a. Medially, are the ethmoid air cells and sphenoid sinus.
b. In this horizontal section through the orbit, note the CLOSE RELATIONSHIP OF THE ETHMOID AND
SPHENOID SINUSES TO THE MEDIAL WALL OF THE ORBIT. Note the medial and lateral walls of the orbit.
c. Note the small spaces in the ethmoid bone (ethmoidal air cells) which collectively make up the ethmoid air sinus
and more posteriorly, the medial walls related to the sphenoid sinuses.
d. These air cells and their lining often get infected (sinusitis) causing an accumulation of fluid.
i. The bony medial wall is paper-thin! Careless exploration of the posterior ethmoidal cells (to clean them
from infection) can break through the lamina papyracea and has resulted in blindness due to damage to the
nearby optic n.
ii. Main point: ethmoid sinus surgery can result in blindness if the air cells are carelessly explored.
e. Lateral wall of the orbit (much stronger than other walls) is related to the middle cranial fossa (with the temporal
lobe of the brain) and more anteriorly, to the temporal fossa (containing the temporalis m.).
f. Surgical approaches to the orbit are sometimes from the lateral aspect.
g. Know the relationships of the sinuses to the orbit.
VII. Eyeball [S6]
VIII. Eyeball (Horizontal Section) [S7]
a. STUDENTS SHOULD STUDY THIS SLIDE ON THEIR OWN.
i. Read about the layers of the eye, the 3 coats of the eye, the chambers of the eye, the refractive media in
your plate notes and your textbook.
ii. Be familiar with the internal anatomy. (Also, see Dr. Zehren’s notes on his PowerPoint).
b. The retina and the optic nerve:
i. The optic nerve (sensory nerve) and the fibers that compose the optic nerve have cell bodies that lie in the
neural part of the retina called the ganglion cell layer. The axons of those ganglion cells converge at the
optic disc papilla/disc. At this point, the axons turn posteriorly, leave the retina, and form the optic nerve.
ii. The optic nerve is the central process of these ganglion cells heading back toward the optic chiasm.
iii. In the center of the optic nerve are tiny structures called CENTRAL ARTERY AND VEIN and when they
reach the optic papilla/disc, they branch to supply the retina. The central artery of the retina is the only
blood supply to the retina and if that artery becomes occluded, you go blind.
IX. Sheaths of the Optic Nerve [S8]
a. Optic nerve in cross section.
b. Since the retina and optic n. develop as an outgrowth of the diencephalon (i.e. forebrain; tract of the brain), they
are surrounded by the three meninges (dura, arachnoid, and pia) and an extension of the subarachnoid space
around the optic nerve termed the INTERVAGINAL SPACE.
c. In the subarachnoid space is CSF. The optic nerve is surrounded by CSF.
d. The central a. and v. of the retina must cross this space and pierce these meninges (they are branches of the
ophthalmic artery and vein) to reach the optic n. Hence, something like a tumor causing a rise in CSF pressure
around the optic nerve will compress the thin-walled vein and impede venous drainage from the retina.
i. This results in edema (swelling) of the optic papilla termed PAPILLEDEMA.
ii. Papilledema can be visualized with an ophthalmoscope (next slide). A swollen optic disc in a patient’s eye
could be a warning sign for this type of complication. It all goes back to the basic anatomy that there is CSF
around the optic nerve and these vessels cross that space.
e. [SQ]: Is this for a tumor anywhere in the brain? Yes. Regardless of where the tumor is, it will cause a rise in
CSF pressure.
f. [SQ]: Would the rise in pressure in the optic nerve ever present itself as a rise in intraocular pressure? Could be
possible since venous drainage is being inhibited.
X. Optic Disc (Papilla) [S9]
a. Note how the branches of the central a. and v. of the retina diverge at the optic disc. The optic disc (papilla)
becomes swollen in papilledema.
XI. Muscles [S10]
XII. Intrinsic Muscles of Eyeball [S11]
a. Comparing intrinsic vs. extrinsic eye muscles.
b. Orient: Anterior part of eyeball, note the cornea, lens, iris and pupil.
c. The eye contains THREE INTRINSIC MUSCLES (all smooth muscles under autonomic control). We will not be
dissecting any of these muscles.
d. The CILIARY M. lies in the ciliary body, which is attached to the elastic lens by the fibers of the ciliary zonule
(also known as the “suspensory ligament of the lens”).
i. When the cililary m. contracts it RELAXES the fibers of the cililary zonule, thus causing the elastic lens to
"round up" for focusing on a near object by shortening the focal length (accommodation).
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 3 of 6
ii. For an object in the distance, the lens will be flatter in appearance.
iii. The ciliary muscles are a muscle that allows your lens to change shape.
iv. This is a counterintuitive concept. When the ciliary muscle contracts it relaxes the fibers of the ciliary zonule
and causes the elastic lens to round up and become more spherical, which shortens the focal length and
allows you to focus on a near object. This is accommodation by the ciliary muscle.
e. The other two muscles are in the iris of the eye:
i. The SPHINCTER PUPILLAE M. around the margin of the pupil constricts the pupil (miosis).
ii. The DILATOR PUPILLAE M. runs radially out from the margin of the pupil & dilates the pupil (mydriasis).
1. Note: Miosis is a smaller word --- it means making the pupil smaller.
XIII. Autonomic Innervation of the Eye [S12]
a. How are these three intrinsic muscles innervated?
b. Parasympathetic fibers - blue; presynaptic fibers solid blue, postsynaptic fibers dashed blue.
c. Sympathetic fibers - red; presynaptic fibers solid red, postsynaptic fibers dashed red.
d. The PARASYMPATHETIC PATHWAY TO THE CILIARY M. & SPHINCTER PULILLAE M. have an identical
pathway and is as follows.
i. The presynaptic parasympathetic neurons lie in the accessory oculomotor (Edinger-Westphal) nucleus in
the midbrain. Their axons leave within the oculomotor n. (not labeled) to the orbit because this is one of its
functional components—GVE. In the orbit, the oculomotor n. gives off an ocular motor (parasympathetic)
root to the ciliary ganglion. After synapsing in the ganglion, postsynaptic parasympathetic fibers reach the
eyeball by traveling in several short ciliary nerves to reach the eyeball. They run within the eyeball to reach
either the ciliary muscle or the sphincter muscle.
e. The SYMPATHETIC PATHWAY TO THE DILATOR PUPILLAE M. functions under times of stress and fear,
which result in pupil dilation.
i. Presynaptic sympathetic neurons in the spinal cord (only place they can lie from T1-L2) and in the case of
the head and neck in the lateral horn of the upper thoracic spinal cord (T1-T3) send their axons into the
sympathetic. The axons ascend to the superior cervical sympathetic ganglion where they synapse.
ii. Postsynaptic fibers then travel in the plexus around the int. carotid a. and enter the cranial cavity in the
region of the cavernous sinus.
iii. Inside the skull, these postsynaptic fibers leave the int. carotid plexus and join V1.
iv. These fibers leave V1 and travel in long ciliary nn. (a branch of the nasociliary n.) carries the postsynaptic
fibers to the eyeball where they innervate the dilator muscle. This is the sympathetic pathway.
XIV.
Position of Ciliary Ganglion [S13]
a. It is a tiny parasympathetic ganglion that is very difficult to find. Note that it lies in the posterior part of the orbit,
just lateral to the optic nerve and just medial to the lateral rectus m. It is about the size of the head of a pen.
It will look like a small glob of fat.
b. Also, note the short ciliary nerves that lead from the ganglion to the eyeball. This will help to identify.
c. The position of the ganglion in Netter’s Atlas is a little misleading. This picture was included from Grant’s Atlas.
XV. Extrinsic Eye Muscles (Right Lateral View) [S14]
a. In contrast to intrinsic eye muscles, extrinsic eye muscles are not confined to the eyeball. They originate outside
of the eye, insert into the sclera, and move the eyeball within the orbit.
b. There are SIX EXTRINSIC (EXTRAOCULAR) EYE MUSCLES --- 4 recti (rectus means “straight”) and two
obliques (superior and inferior).
c. The four recti (sup., inf., med., and lat.) all arise from the common tendinous ring (annular tendon) that
surrounds the optic canal. This fibrous ring is the origin of the 4 rectus muscles. They pass anteriorly, diverging
to insert into the anterior part of the sclera, the white of the eye, just behind the junction with the cornea.
d. The sup. oblique arises from the posterior part of the orbit, but not from the common tendinous ring. It arises
from the body of the sphenoid bone in the posterior part of the orbit and passes anteriorly, but it makes a sharp
bend after passing through the trochlea (a fibrocartilaginous pulley) to insert into the posterolateral (hence the
name “oblique”) part of the sclera more posteriorly than the rectus muscles.
i. Note: from a FUNCTIONAL viewpoint think of the trochlea as the origin of the sup. oblique m.
1. In other words, the trochlea is its functional origin even though anatomically it originates from the
body of the sphenoid.
e. The inf. oblique has an origin entirely separate from the other muscles. It arises from the floor of the orbit
(anteromedial corner) and passes below the eyeball posterolaterally to insert into the sclera.
XVI.
Orbital Axis Not the Same as Visual Axis [S15]
a. Orient: Superior view of the two bony orbits
b. Medial walls of the two orbits are parallel to each other; lateral walls are perpendicular to each other.
c. Eyeballs are shown in the primary position (i.e., directed straight ahead).
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 4 of 6
i. In the primary position, the visual axis (anteroposterior axis of eyeball) does not correspond to the orbital
axis (longitudinal axis of orbit).
d. This is important to keep in mind, because the function of the extrinsic muscles depends on whether the eyeball
is in the primary position, is turned inward (adduction) or is turned outward (abduction).
e. One muscle have one function in a particular position, but as the eye is adducted that function changes.
XVII. Movements Around the Vertical Axis [S16]
a. Orient: In this slide and the following two slides, the RIGHT eyeball is shown in superior view (note the med. &
lat.; ant. & post. directions) and in the primary position.
b. In addition, the axis around which the eyeball moves is indicated by a red dot or a red line.
c. There are three axis on which the eyeball can rotate:
i. The vertical axis (passes inferior to superior right in the center of the eye) of the eyeball permits the
movements of:
1. adduction (pupil or center of cornea moves toward midline)
2. abduction (pupil moves laterally)
ii. The MEDIAL RECTUS M. ADDUCTS THE EYE & The LATERAL RECTUS M. ABDUCTS THE EYE.
These are the only functions of the medial and lateral recti. If one glances to one side, the medial rectus of
one eye acts in concert with the lateral rectus of the other eye.
d. The superior and inferior rectus mm. as they pass toward their insertion also assist in adduction when the
eyeball is in the primary position because they are slightly on the medial side of the vertical axis.
e. Similarly, the superior and inferior oblique mm. in passing on the medial side from their origin (more anterior) to
their insertion (more posterior) assist in abduction.
XVIII. Movements Around the Lateromedial (Transverse) Axis [S17]
a. The lateromedial (transverse) axis of the eyeball permits the movements of elevation (pupil moves superiorly)
and depression (pupil moves inferiorly).
b. ELEVATION OF THE EYE IS PRODUCED BY THE SUP. RECTUS AND INF. OBLIQUE MM.
i. Elevation – turn the eye around the axis so that the pupil moves upward
c. DEPRESSION OF THE EYE IS PRODUCED BY THE INF. RECTUS AND SUP. OBLIQUE MM.
d. There are two elevators and two depressors when the eyeball is in the primary position.
e. Proceeded to [S18] and returned to [S17]. Italicized notes are notes from [S17] once he returned.
f. To produce pure elevation from the primary position, both the superior rectus and inferior oblique must work
together.
i. This is because when the eye is in the primary position (as shown here), the tendency of the sup. rectus
(elevates) to adduct and intort the eye simultaneously is counterbalanced by the tendency of the inf.
oblique (elevates) to abduct and extort. You get pure elevation when these muscles contract.
ii. On the other hand, to produce elevation of the eyeball when it has already been abducted (by the lateral
rectus) the visual axis will coincide with the superior rectus, only the superior rectus is an effective elevator.
iii. Similarly, to produce elevation of the eyeball when it has already been adducted (by the medial rectus) the
visual axis will be changed, only the inferior oblique is an effective elevator.
g. There are handout(s) of function of extrinsic eye muscles in your syllabus.
XIX.
Movements Around the A-P Axis [S18]
a. Orient: right eye in anterior view.
b. The anteroposterior axis permits the movements of intorsion and extorsion.
c. In intorsion and extorsion, the pupil does not move b/c the A-P axis passes directly through it.
d. Rather, a wedge-shaped piece of the cornea (the “twelve o’clock” part of the cornea) moves medially (intorsion)
or laterally (extorsion) (see arrows).
e. The SUPERIOR RECTUS & SUPERIOR OBLIQUE PRODUCE INTORSION.
f. The INFERIOR RECTUS & INFERIOR OBLIQUE PRODUCE EXTORSION.
g. Returned to previous slide and explained how muscles act in pairs to produce a pure movement.
XX. Innervation of Extrinsic Eye Muscles (SO4, LR6, R3) ( [S19]
a. The INNERVATION OF THE EXTRINSIC EYE MUSCLES is expressed as a simple "formula": SO4 (LR6) R3.
b. Thus, the Sup. Oblique is innervated by IV, the Lat. Rectus by VI, and the remaining muscles by III.
i. The superior oblique is the only muscle innervated by CN IV coming off dorsal to the midbrain going
through the superior orbital fissure and will see it in the orbit entering the posterior-superior part of that
muscle. This is all CN IV does. One muscle.
ii. Likewise, the lateral rectus (cut and reflected here) is innervated by the CN VI that enters the orbit through
the superior orbital fissure and immediately sinks into the deep/medial aspect of the lateral rectus. You
have to pull that nerve away from the muscle to identify it. This is all CN VI does. One muscle.
c. All the remaining muscles are innervated by CN III.
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 5 of 6
d. Note that III divides into two divisions (sup. and inf.) just as it enters the orbit through the superior orbital fissure
(shown but not labeled).
e. As might be expected, the sup. division supplies the sup. rectus (and the overlying levator palpebrae superioris
– muscle of upper eyelid, does not insert into eyeball) while the inf. division supplies the inf. rectus, inf. oblique
and med. rectus. The functional component all the nerves supplying all of these muscles is GSE.
i. (But the smooth muscle is GVE)
f. Recall that III, IV & VI all enter the orbit through the superior orbital fissure.
g. Note that the branch of the inferior division of the oculomotor is the one that caries parasympathetic fibers
coming off the ciliary ganglion.
XXI.
Muscles of the Upper Eyelid [S20]
a. TWO MUSCLES serve to elevate the upper lid:
i. 1) LEVATOR PALPEBRAE SUPERIORIS (palpebrae – “eyelid”) – lies directly to superior to sup. rectus
ii. 2) SUP. TARSAL M.
b. The levator is a voluntary (skeletal) muscle innervated by the sup. division of III. It originates from the lesser
wing of the sphenoid bone (roof of the orbit) and forms an aponeurosis, which inserts into the front of the
superior tarsal plate and into the skin of the upper lid.
c. The sup. tarsal m. is involuntary (smooth) and originates from the levator palpebrae superioris (but unlike the
levator it is smooth muscle) and inserts into the superior tarsal plate. The superior tarsal m. is innervated by
postsynaptic sympathetic fibers under autonomic control. Their cell bodies line the sup. cervical ganglion just
like for the dilator pupillae
d. Two muscles can elevate the eyelid and open the palpebral (orbital) fissure.
e. Paralysis of either muscle due to a lesion of III or the cervical part of the sympathetic trunk causes PTOSIS
(drooping) of the upper eyelid. Remember one of the symptoms of Horner’s Syndrome when you lesion the
cervical sympathetic trunk is a dropped upper eyelid because you are cutting off the sympathetic innervation to
the superior tarsal muscle.
f. There is an excess of fat in the orbit and the optic nerve takes a wavy-course to the eyeball so it does not
restrict the movements of the eyeball.
XXII. Periorbita & Fascia [S21]
XXIII. Periorbita and Fascia [S22]
a. STUDENTS SHOULD STUDY THIS SLIDE ON THEIR OWN on plates notes and lecturer notes
b. The periosteum (connective tissue) aligning the bones of orbit is termed PERIORBITA.
c. The eyeball and extrinsic muscles are surrounded by a fascial sheath
i. (E.g. BULBAR SHEATH and CHECK LIGAMENTS).
XXIV. Nerves [S23]
XXV. Ophthalmic Nerve (V1) [S24]
a. The chief sensory nerve of the orbit (other than the optic n.) is the OPHTHALMIC N. (V1).
i. V1 is the first of the three divisions of the trigeminal n. (CNV) and begins as a branch of the trigeminal
ganglion (located in the middle cranial fossa)
ii. (Review: V1 – superior orbital fissure, V2 – foramen rotundum, V3 – foramen ovale, foramen spinosum –
middle meningeal artery, fold of dura that covers the pituitary - diaphragma sellae)
iii. As it leaves the ganglion, V1 has only one functional component (GSA), but its branches may secondarily
pick up other functional components from other nerves.
1. CN V as a whole only has GSA and SVE components. All of the SVE goes out with the mandibular
nerve. V1 and V2 as they leave the ganglion are purely GSA.
b. As V1 approaches the sup. orbital fissure it trifurcates (BEFORE it reaches the superior orbital fissure) into its
terminal branches: “NFL”
i. 1) Nasociliary n. – deeper
ii. 2) Frontal n.
iii. 3) Lacrimal n.
c. The FRONTAL N. proceeds directly anteriorly and divides into two branches:
i. 1) supratrochlear n. (which leaves the orbit superior to the trochlea)
ii. 2) supraorbital n. (which leaves the orbit through the supraorbital notch or foramen).
iii. Both the supratrochlear and supraorbital nn. are sensory to the upper eyelid, forehead and scalp. They are
just traveling through the orbit and going to the face.
1. Note: It is easy to mistake the bifurcation of the supraorbital nerve and misidentify the medial branch
as the supratrochlear. The supratrochlear is the smaller of the two and usually branches further
posteriorly and if you trace it back far enough it will leave just above the trochlea, it does not go
through the supraorbital foramen. Be careful when distinguishing these two.
d. The LACRIMAL N. runs along the lateral aspect of the orbit and is sensory to the lacrimal gland & upper eyelid.
Gross: 8:00 - 9:00
Scribe: Ryan O’Neill
Thursday, February 5, 2009
Proof: Strud Tutwiler
Dr. Zehren
Orbit
Page 6 of 6
i. It has a palpebral twig, which helps supply the upper eyelid (GSA component).
ii. Secondly, it also conveys postsynaptic parasympathetic secretomotor fibers to the gland.
e. [SQ] How does supratrochlear leave the orbital? Just above the trochlea. There is not special foramen.
XXVI. Ophthalmic Nerve (V1) Deep Dissection [S25]
a. Orient: This is a deeper dissection (both the lev. palpebrae sup. and sup. rectus have been removed) to show
the NASOCILIARY N. & ITS BRANCHES.
b. The nasociliary n. runs anteromedially just superior to the optic n.
c. The nasociliary n. gives off a couple of long ciliary nn. (very delicate strands) which are sensory to the eyeball
(including the cornea, but not the retina). The afferent fibers of the corneal reflex are traveling back to the brain
via the long ciliary nerves and the nasociliary ophthalmic and trigeminal.
d. The long ciliary nn. also convey postsynaptic sympathetic fibers to the dilator pupillae m.
i. These sympathetic fibers have their somata in the sup. cervical ganglion.
e. Near the medial wall of the orbit the nasociliary n. gives off ant. and post. ethmoidal nn.
i. These nerves leave the orbit through the anterior and posterior ethmoidal foramina and innervate the
mucosa lining the ethmoidal air cells.
ii. The ant. ethmoidal n. also enters the nasal cavity (through the nasal slit near the crista galli) where it gives
off general sensory (GSA) branches. It finally appears on the face (as the ext. nasal n.) to supply the skin of
the lower one-half of the nose. At this point it is called the external nasal nerve. It begins in the orbit and
ends on the tip of the nose.
f. In addition to the ant. ethmoidal n., the nasociliary n. has one other terminal branch --- the infratrochlear n.
i. This nerve leaves the orbit below the trochlea and supplies the skin over the upper one-half of the nose.
XXVII. Vessels [S26]
XXVIII. Ophthalmic Artery [S27]
a. The OPHTHALMIC A. is the chief artery supplying the orbit; the infraorbital a. (runs in the floor of the orbit) also
contributes.
b. The ophthalmic a. arises from the int. carotid a. (just before it terminates) and immediately enters the orbit
through the optic canal (with II). It arises in the middle cranial fossa, enters the optic canal, runs below the optic
nerve, then winds around above the optic nerve, and pursues an oblique course in conjunction with the
nasociliary nerve. The artery and nerve run together.
c. The ophthalmic a. has numerous branches in the orbit.
d. They can be grouped into OCULAR BRANCHES (to the eyeball) and ORBITAL BRANCHES (to extraocular
structures).
e. The most imp. ocular branch is the central a. of the retina --- it pierces the optic n. to reach the retina, to which it
is the sole arterial supply.
f. The orbital branches of the ophthalmic a. include the lacrimal a. and the supraorbital and supratrochlear aa. (to
the forehead and scalp).
g. As the ophthalmic a. passes through the orbit it runs anteromedially just superior to II, in company with the
nasociliary n.
h. Most of the branches of V1 have arteries running with them.
XXIX. Ophthalmic Veins [S28]
a. VENOUS DRAINAGE OF THE ORBIT IS VIA THE SUP. AND INF. OPHTHALMIC VV.
i. These veins receive tributaries corresponding to the branches of the ophthalmic a.
ii. They also receive the four vorticose vv., which drain the choroid layer of the eye.
b. The ophthalmic vv. communicate anteriorly with the angular v. (=upper end of facial v.) and posteriorly with the
cavernous sinus.
c. Since these ophthalmic veins are valve-less, blood can travel in both directions and infection can spread from
the face via the ophthalmic veins into the cavernous sinus.
d. The inf. ophthalmic v. also communicates with the pterygoid plexus in the infratemporal fossa via the inf. orbital
fissure.
XXX. End of Lecture [S29]
[end 54:33 min]