Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
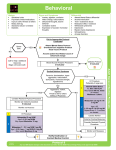
IT'S NOT THE YEARS IN YOUR LIFE THAT COUNT. IT'S THE LIFE IN YOUR YEARS.” ABRAHAM LINCOLN DELIRIUM (and DEPRESSION) Dr E Holbeach Geriatrician DELIRIUM- Outline • • • • What is it Why do we care Why does it happen What can we do CASE STUDY • Evening shift • Page- please review Mrs M bed 5B UnA. Very agitated. Need diazepam please. Delirium definition • Transient mental disorder • Impaired concentration, cognition and altered conscious state • Fluctuating course • Acute onset; Lasting days –weeks – months Criteria for delirium, according to the (DSM IV) – fluctuations of the conscious state – fluctuating wakefulness, nocturnal disturbance, poor attention, disorientation – perceptual disturbance – usually visual hallucinations, other hallucinations also common including auditory hallucinations and tactile hallucinations, misinterpretations – thinking disturbance – often persecutory delusions – Onset over short time frame – Evidence that it is secondary to medical condition/ drugs/ substance intoxication Clinical variants – Hyperactive 15-47% • Hyper-reactive, • autonomic arousal • Wandering, hallucinations, aggression, agitation. – Hypoactive 19-71% • Lethargic, drowsy • Apathetic, depressed • Quiet, confused – Mixed 43-56% Delirium- IMPORTANCE • • • • • Common problem Often unrecognized Serious complications $$$ Often preventable (40-50% cases) And importantly… • INTERNS ARE FREQUENTLY ASKED TO MANAGE THE BEHAVIOURAL PROBLEMS!!! Epidemiology Delirium Rates Hospital: -Prevalence (on admission) -Incidence (in hospital) -Post hip fracture Postoperative: Intensive care unit: Nursing home/post-acute care: Hospital mortality: One-year mortality: 10-40% 15-60% 40-55% 15-53% 70-87% 20-60% Mortality 22-76% 35-40% Delirium - importance • Increases risk of poor outcomes: – Increased risk of death – Increased risk of morbidity • ↑ 2-3 times hospital acquired complication • Eg- falls, pressure areas, pneumonia – Increased risk of functional decline • higher risk of discharge to residential care: x 3-7 – Increased length of stay: x 2.2; ≈ 5day • Cost to the healthcare system – Hospital costs – Post hospital costs DIAGNOSIS • FREQUENTLY MISSED!! • Previous studies: 32-66% cases unrecognized by physicians • Yale-New Haven Hospital study (1988-1989): – 65% (15/23) unrecognized by physicians – 43% (10/23) unrecognized by nurses CAM- Confusion Assessment Method Uses 4 criteria assessed by CAM: (1) acute onset and fluctuating course (2) inattention difficulty focusing, distractiblity, trouble following conversation (3) disorganized thinking incoherent, rambling, irrelevant conversation, illogical flow, unpredictable switching between topic (4) altered level of consciousness lethargy, stupor, hypervigilant/ hyperalert Delirium= the presence of criteria: (1), (2) and (3) or (4) Pathophysiology - Not really understood… but: - Functional rather than structural lesion - Characteristic EEG findings (generalized slowing) - Final common pathway of many pathogenic mechanisms—resulting in a failure of cholinergic transmission - Other neurotransmitters also invovled: dopaminergic excess, NA, 5HT3, GABA, cytokines etc etc etc Aetiology • Almost always multifactorial • Predisposing factors (vulnerable patients) • Precipitating factors ( noxious stimuli) • Similar to concept of seizures and seizure threshold – with enough noxious stimuli delirium can occur in “normal” brain or alternatively with minimal noxious stimuli in a “vulnerable” brain AETIOLOGYmultifactorial model Predisposing factors in hospital patients (high level of evidence) 1. 2. 3. 4. 5. 6. 7. 8. Age > 70 years ( increases with ↑ age) Blind -sensory impairment – particularly visual Cognitive impairment – dementia Co existing illness - severity, co morbidity Drugs– on more than three medications Depression Electrolyte imbalance – abnormal Na Exposure to procedures – particularly IDC, physical restraints, multiple procedures So- elderly, frail, cognitively impaired, sensory deprived with multiple medical conditions on multiple drugs…. Delirium - Management Identify precipitating factors – reverse these where possible Manage the symptoms -provide supportive care environment Prevent complications -pressure sores, falls (risk reduction measures) Educate patient carers and families -can be very scary for the patient and their family Case Study • Mrs M is a 78 year old female from home alone. Day one of admission to hospital with urinary incontinence, raised inflammatory markers, likely infective exacc COPD. Started on Ceftriaxone, Azithromycin, bronchodilators, prednisolone. Also started on Gliclazide for DM and oxycontin for back pain. • Comorbidities- T2DM, COPD, Microcytic anaemia, GORD, osteoarthritis with chronic back pain. • On review- Restless. Pulling at bed clothes, trying to get out of bed. Distracted. Starts screaming and scratching when you try to examine…. Step 1- identify precipitants • Review History • Collaborative history – Incl baseline functional status, baseline cognition – Incl ETOH/ drug history (NEVER ASSUME) • Examination/ Observation • Review Medication Chart – Then review it again • Investigations Examination NEVER EVER WRITE “UNABLE TO EXAMINE DUE TO AGITATION”you can ALWAYS observe something that is helpful in the assessment. • Conscious State/ Behaviour • Observations, including BSL, bowel chart review • FULL examination – Chest/ Abdo/ Skin/ Peripheries – Fluid status – Neuro- abbreviated examination • Limb movement/ pupils/ facial asymmetry/ cogwheel – IDC/ IVC/ telemetry leads – shackles • ANY ACUTE ILLNESS! • Don’t forget constipation, urinary retention- bladder US if unsure Medication Chart • Almost all drugs may contribute • Increased number of drugs ↑ risk • Particular medications significantly increase risk • Any psychoactive medication or medication with significant psychoactive side effects ( i.e. anticholinergic, opiates) Think Medications • Which ones?! – Sedatives – Opiates, narcotics – Anticholinergics – Steroids – Centrally acting drugs – Multiple medications- think drug-drug interactions – Diuretics –watch for hyponatraemia, dehydration, ARF Investigations • Bloods: FBE, UEC, LFT, CRP, Ca++ – Make sure B12, Fol, Vit D, TSH checked in last 3m • • • • MSU CXR B cultures Others as per clinical picture – ABG- check for hypercapnoea, hypoxia – CTB if focal neuro, hx of head trauma or delirium not resolving – Ammonia if history of CLD – Consider LP, EEG, CK, trop STEP 2- MANAGEME THE SYMPTOMS SUPPORTIVE CARE ENVIRONMENT • Environment – lighting, quiet, orientation cues • clock, familiar objects – Maintain sleep-wake cycle • • • • • • • • Avoid room changes, regular carers, staff Provide access to hearing aids, glasses Maintain oral intake, maintain hydration Maintain regular bowel function Maintain independence with ADL’s – mobility Avoid IDC, physical restraints Good communication – i.e. interpreters Use 1:1 care and family to sit with patient Escalating behaviours… • Agitation, aggression to the point that patient or others at risk • May need to use pharmacotherapy – Start low, go slow! Antipsychotic management • Haloperidol only agent in RCT, less data on atypicals • Low doses initially – – Haloperidol 0.25 mg – 0.5mg (po/ IM) – Risperidone 0. 25 – 0.5mg (po, quicklet) – Olanzapine 2.5mg - 5mg (po/ wafer/ IM) – Quetiapine 12.5 – 25mg (po) • Avoid benzodiazepines if possible as can worsen delirium unless EToH withdrawal – If you need to use (eg- parkinsons/ DLB patients, not responding to above): • Oxazepam 7.5- 15mg (po) intermediate acting benzodiazepine Antipsychotic risks • All antipsychotics cause sedation and drowsiness – which can perpetuate delirium • All can cause extra pyramidal side effects (greater with haloperidol) • All can increase QT (avoid if QTc >500) • Olanzapine/ Risperidone – increased risk stroke in elderly pts with dementia • Make a plan to wean these medications ! – IF DISCHARGED ON THESE MEDICATIONS PLEASE WRITE ON DISCHARGE SUMMARY FOR GP TO REVIEW AND REDUCE DOSAGE!! Step 3: Prevent complications • Reduce risk of falls – Hi-lo bed – 1:1 nursing – Close to nurse station – Avoid use of physical restraints ! • Reduce risk of pressure areas – Air mattress, elevate heels, reposition • reduce risk of other injury – Remove all unnecessary catheters lines etc Step 4: Education to Family • • • • Educate family as to what delirium is Educate family as to how they can help Educate family as to what to expect Educate patient as they are improving!! Delirium outcomes – only 4% completely resolved at discharge – 18% completely resolved at 6 months – 31% improved but relapsed post discharge – 31% still met DSM criteria at 6 months – Ensure discharge plan takes into consideration decreased cognition and ensure follow up is arranged DEPRESSION DEPRESSION • Common! • Often under-diagnosed and undertreated • In hospital, THINK about depression for patients with – – – – Loss of appetite, persistent nausea Non specific symptoms Not making gains/ not participating in Physio Psychomotor agitation/ retardation • Do a suicide assessment: – Thoughts versus specific plan Antidepressants • • Not every depressed patient needs antidepressants! KNOW YOUR DRUGS, know that they are also used to treat other conditions (pain) • SSRI – Eg- citalopram, escitalopram, fluoxetine, – SE: GI, Insomnia, Sedation, Sexual dysfunction, Hyponatraemia • SNRI – Eg- venlafaxine, Duloxetine – SE: GI, headache, sweating, agitation, dizzyness, sexual dysfunction, hyponatraemia • Others: – Mirtazepine; SE: sedation, increased apetite, weight gain – TCA (amitriptyline, dothiepin, doxepin: main use now is in neuropathic pain due to high SE profile – MAO A inhibitors • Drug interaction: AVOID TRAMADOL!!– Risk serotonin syndrome: • • • neuromuscular excitation: hyperreflexia, clonus, myoclonus, tremor, rigidity Autonomic effects: hyperthermia, sweating, tachycardia, mydriasis CNS effects: agitation, anxiety, confusion “Knowing is not enough; we must apply. Willing is not enough; we must do.” Goethe