Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
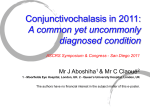
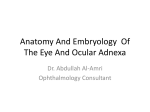
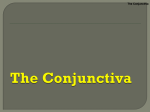
Clinical evaluations of the quantitative locator for conjunctiva resection used as an instrument for the treatment of conjunctivochalasis Keywords: conjunctivochalasis, conjunctiva resection, treatment ZHANG Xing-ru, LI Qing-song, XIANG Min-hong, ZHENG Yi-ren, ZHOU Huan-ming, ZHANG Zhen-yong , ZHANG Long Department of Ophthalmology, Putuo Hospital, Shanghai Chinese Traditional Medicine University, Shanghai 200062, China (Zhang XR, Li QS, Xiang MH, Zhou HM, Zhang ZY, Zhang L) Department of Ophthalmology, Shanghai No.10 Hospital, Tongji University, Shanghai 200072, China (Zheng YR) Correspondence to Dr. LI Qing-song, Department of Ophthalmology, Putuo Hospital, Shanghai Chinese Traditional Medicine University, Shanghai 200062, China. (E-mail: [email protected]) This study was supported by Innovative Project of Science &Technology Committee, Putuo District, Shanghai (2008-B-88,2010PTKW07) Purpose To evaluate the quantitative locator for conjunctiva resection when used as an instrument for the treatment of conjunctivochalasis (CCh). Methods Poly β-hydroxyethyl methacrylate resin / HEMA (water gel) was used as the material to make the quantitative locator which is designed to suit the specific patient. 46 patients with bilateral symptomatic CCh were included in this prospective study. Of the patients, while the right eye underwent the popularly used crescent-shaped conjunctiva resection (Group І), the left eye was treated with conjunctiva resection assisted by the quantitative locator (Group П). International Ocular Surface Disease Index (OSDI), scores of remnant conjunctiva fold, complications and conjunctival cut healing, height of tear meniscus, tear break-up time (BUT), and time of surgery were evaluated. Tasting chloromycetin test (TCT) was used to evaluate how the lacrimal duct worked. Results OSDI was significantly lower in Group П (8.82±2.36) than that in Group І (14.67.3±2.21)(t = 12.22, p <0.01). Conjunctiva fold remained in Group II was less than that in Group I. Scores of remnant conjunctiva fold in Group I were significantly 1 higher than that in Group II(t=31.8, p<0.01).While evaluation scores of conjunctival cut healing in Group I were lower than that in Group II, scores of complication in group I were significantly higher than that in Group II at 8 weeks after surgery (t = 89.60, p <0.01). There was no significant difference in eyes with normal BUT(Х2= 0.031, p=0.985)between the two groups, as it was in eyes with positive TCT(Х2 = 0.14, p = 0.93) and in eyes with normal height of tear meniscus(Х2= 0.48, p=0.78). Mean surgery time was significantly shorter in Group II (17.11±2.08 minutes) than that in Group I (25.22±4.78 minutes) (t=13.84, p<0.01). Conclusion Quantitative locator can be used as an effective, safe, and less time-consuming instrument to facilitate conjunctival excision for symptomatic CCh treatment. Conjunctivochalasis (CCh), defined as a redundant, loose, nonedematous inferior bulbar conjunctiva interposed between the globe and the lower eyelid, tends to be bilateral and is more prevalent in older populations.1,2Patients vary in the degree of their symptomology ranging from asymptomatic to experiencing ocular irritation, pain, subconjunctival hemorrhage, epiphora, dry eye, and/or ulceration. 3-5 Treatment of conjuntivochalasis varies depending on the severity of symptoms. Asymptomatic eyes can be left untreated and followed up periodically for signs of progression. If symptoms continue despite topical treatment, surgery may be needed to remove the segments of redundant conjunctiva. In view of surgical procedures, crescent-shaped conjunctiva resection, first introduced by Hughes, 5 successfully treats CCh by removing crescent-shaped conjunctiva under the lower eyelid and closing the conjunctival incision with a continuous silk suture. This approach has been widely used and demonstrated to be successful. 4,6 However, it is difficult to design how much conjunctival tissue should be excised before operation as well as in the operation phase. This is usually more complicated with attendant subconjunctival hemorrhage. So if a tool could be applied to facilitate the excision of conjunctiva, it may optimize this procedure. Herein we introduce a quantitative locator for conjunctiva resection and performed it on 46 patients with bilateral symptomatic CCh. 2 METHODS Design of locator The quantitative locator used in this study is made of β-hydroxyethyl methacrylate / HEMA. It consists of a circle at the centre with a diameter in 12 mm and two arcs 5 mm posterior from the circle. A slit between the two arcs was made as an access of loose conjunctiva to the surface of the locator. Five holes each with a diameter in 1 mm at the 2, 4, 6, 8, 10-o’clock positions of the outer arc are made for the micro-forceps to pull out the conjunctiva beneath the inner face of the locator after it is placed on the eyeball.(Figures 1 and 2) Patients 46 patients (twenty males, twenty-six females; mean age, 70.77 ± 9.42 years) with bilateral symptomatic CCh but without other ocular surface diseases were included in this study. All Parents provided informed consent according to the Tenets of the Declaration of Helsinki. Of the patients, while the right eye underwent the popularly used crescent-shaped conjunctiva resection (Group І), the left eye was treated with conjunctiva resection assisted by the quantitative locator (Group П).This study was approved by the Ethnic Committee of Putuo Hospital, Shanghai Chinese Traditional Medicine University. Surgical procedures Conjunctiva excision assisted by quantitative locator 0.5% Alcaine eye drops were administered to anesthetize the conjunctiva before surgery. After the eye was exposed with a speculum, the locator (Figure 3) was placed on the eyeball with its centre coincident with the centre of cornea. A forceps was used to pull out the loose conjunctiva from the little holes located at the edge of the outer arc and next from the slit between the two arcs. In this way, loose conjunctiva can be laid on the surface of the locator without sliding, and therefore can be easily excised. After excision of the conjunctiva, the locator was lifted and the cut was sutured with a 10-0 silk suture. 0.5% gentamicin and artificial tear eye drops were administered 4 times per day for two weeks. 3 Crescent-shaped conjunctiva resection procedure After topically anesthetized with 0.5% Alcaine eye drops, the eye was exposed with a speculum and loose conjunctiva was pushed downward and the folded conjunctiva was kept 5 mm posterior from the limbus. Redundant conjunctiva was gathered together with no influencing on the eye movement and the gathered conjunctiva was excised like a crescent. The cut was approximated with a 10-0 nylon silk suture. The duration of keeping sutures should be 10~14 days during which 0.5% gentamicin and artificial eye drops were administered 4 times per day. Clinical evaluations Ocular surface symptoms evaluations OSDI was used to evaluate the ocular symptoms7as it was described by Li, et al.2 Loose conjunctiva excision evaluation At 2, 4, 8 weeks after surgery, patients were examined under the slit lamp microscope. Score was recorded as 0 with no loose conjunctiva, whereas it was recorded as 1 score with grade I conjunctival fold and recorded as 2, 3, 4 scores as such. Conjunctival wound healing evaluation Conjunctival wound healing was evaluated by healing scores. Grade A healing was recorded as 3 scores when the conjunctiva demonstrated to be fine with healing line and no scar formation; Grade B healing was recorded as 2 scores with little conjunctival scar or swelling but with no infection; and Grade C healing was recorded as 1 score with infection of conjunctiva. This classification and healing scores respectively were documented at 2, 4, 8 weeks after surgery. Complications evaluation Below are the main complications after CCh surgery: conjunctival fold remaining, roughness of conjunctival cut, scar, restriction of eye movement, shallow conjunctival sac, cut break, and infection. If one complication occurred, 1 score was recorded; two 4 complications occurred, 2 scores was recorded as such. No complication was recorded as 0 score. Tear meniscus and BUT evaluation Height of tear meniscus was measured by micro-scale in the slit lamp and defined abnormal when it was lower than 0.3 mm or the tear meniscus was irregular, dry or broken. BUT was measured and evaluated as described in ophthalmic textbook. Lacrimal duct function evaluation Tasting chloromycetin test (TCT), described by Zhang, et al in their early report, 8 was used to evaluate how the lacrimal duct worked. Statistical analysis All statistical analyses were performed with a statistics program SAS 6.0. Statistical significance was evaluated usingX2 and t-test. P <0.05 was considered significant. RESULTS Ocular surface symptoms evaluations OSDI scores were significantly lower in Group II than that in Group I at all time points. There was a decrease in OSDI scores from a mean value of 30.28 at baseline before surgery to 8.82 at 8 weeks after surgery in Group II, as it was from 30.43 to 14.67 in Group I (Table 1). Table 1 OSDI in two groups before and after surgery at all time points Surgical procedures Locator-assisted conjunctiva excision Crescent-shaped conjunctiva resection eyes OSDI Pre-op 2 weeks 4 weeks 8 weeks 46 30.28±5.68 22.08±3.13 16.95±2.77 8.82±2.36 46 30.43± 5.04 24.56±3.30 21.71±2.88 14.67 ±2.51 t=5.04,p<0.01, t=10.80 , p<0.01 t=12.22 , p<0.01 Loose conjunctiva excision evaluation Conjunctiva fold remained in Group II was less than that in Group I. Scores of remnant conjunctiva fold in Group I were significantly higher than that in Group II (t=31.8, p<0.01)At 8 weeks after surgery, 2 eyes with Grade I CCh were observed 5 in Group II whereas 5 eyes with Grade I and 2 eyes with Grade II CCh appeared in Group I (Table 2). A normal conjunctival surface with no folded conjunctiva was observed at 8 weeks after locator-assisted conjunctiva excision (Figure 4). Table 2 . Scores of remnant conjunctiva evaluation after surgery at all time points Surgical procedures Locator-assis ted conjunctiva excision Crescent-sha ped conjunctiva resection eyes 2 weeks after surgery 4 weeks after surgery 0、 I 、II 、III scores 8 weeks after surgery 0、 I 、II 、 scores 0、 I 、II 、III scores III 46 42、4、0、0 4 43、3、0、0 3 44、2、0、0 2 46 37、6、3、0 12 39、5、2、0 9 39、5、2、0 9 t=40.75, p<0.01 t=30.57, p<0.01 t=31.85, p<0.01 Evaluation of conjunctival wound healing There was no significant difference in scores of conjunctival wound healing evaluation between the two groups at 2 weeks after surgery (t = 1.43, p = 0.159), but not at 4 weeks (t = 3.760, p <0.01) and 8 weeks (t = 5.62, p <0.01) (Table 3) . A smooth conjunctiva surface with no evident cut line was observed at 8 weeks after locator-assisted conjunctival excision (Figure 4). Table 3. Scores of conjunctival wound healing evaluation Surgical procedures eyes Scores 2 weeks 4 weeks 8 weeks Locator-assisted conjunctiva excision 46 84 103 126 Crescent-shaped conjunctiva resection 46 82 92 103 t=1.43, p=0.159 t = 3.76,p<0.01 t= 5.62,p<0.01 Evaluation of the height of tear meniscus and BUT There was no significant difference in BUT(Х2= 0.031,p=0.985)between the two groups, as it was in the height of tear meniscus(Х2= 0.48, p=0.78). While there was a normal height of tear meniscus in 40 eyes (86.9%) and a normal BUT (≥10 s) in 33 eyes (71.7%)in Group II at 8 weeks after surgery, the height of tear meniscus and BUT were respectively normal in 32 eyes(69.5%)and 30 eyes(65.5%)in Group I at this time point.(Table 4,5) 6 Table 4 Evalution of the height of tear meniscus Surgical procedures Eyes with normal height of tear meniscus (% ) Eyes pre-op Locator-assisted excision Crescent-shaped resection conjunctiva conjunctiva 2 weeks 4 weeks 8 weeks 46 0(0.0%) 30(65.2%) 38(82.6%) 40(86.9%) 46 0(0.0%) 29(63.0%) 29(63.0%) 32(69.5%) Table 5 BUT before and after surgery at all time points Surgical procedures Locator-assisted excision Crescent-shaped resection Eyes with BUT≥10s(%) Eyes conjunctiva conjunctiva pre-op 2 weeks 4 weeks 8 weeks 46 8(17.3%) 30(65.2%) 32(69.5%) 33(71.7%) 46 9(19.5%) 28(60.8%) 28(60.8%) 30(65.5%) Evaluation of complications Scores of complications in group I were significantly higher than that in Group II (t = 89.60, p <0.01). Fewer complications occurred in locator-assisted conjunctiva excision. (Table 6) Table 6 Scores of complications evaluation Surgical procedures Eyes Locator-assisted conjunctiva excision Crescent-shaped conjunctiva resection 46 46 Scores 2 weeks 4 weeks 8 weeks 21 51 12 33 9 30 t=55.56,p<0.01 t=57.90,p<0.01 t=89.60,p<0.01 Evaluation of lacrimal duct function There was no significant difference in TCT between the groups(Х2=0.14, p=0.93) (Table 7). Larimal duct function respectively resumed in 23 eyes(50.0%) in Group II and 20 eyes (43.4%)in Group I at 8 weeks after surgery. Table 7 Evaluation of lacrimal duct function Surgical procedures Locator-assisted conjunctiva excision Crescent-shaped conjunctiva resection Eyes with positive TCT(%) Eyes pre-op 2 weeks 4 weeks 8 weeks 46 0(0.0%) 8(17.3%) 21(45.6%) 23(50.0%) 46 0(0.0%) 8(17.3%) 18(39.1%) 20(43.4%) Х2=0.14, p=0.93 7 Surgical time Mean surgery time was significantly shorter in Group II (17.11±2.08 minutes) than that in Group I (25.22±4.78 minutes)((t=13.84, p<0.01). DISCUSSION The crescent excision of the inferior bulbar conjunctiva has been advised as a surgical procedure in the management of conjunctivochalasis refractory to medical treatments. 9,10 In this procedure, it is of vital to design delicately how much bulbar conjunctiva should be excised. As Liu4 has cautioned, overzealous resection of the conjunctival tissue may result in a compromised lower fornix, which may restrict motility or cause incision broken and corneal problems whereas underestimated resection would cause loose conjunctiva remain. This study highlighted an instrument termed as quantitative locator for conjunctiva resection. This locator is made of β-hydroxyethyl methacrylate acetate / HEMA (water gel) with chemical stability, bringing no stimulations. As it becomes soft in water, it is easy to be implanted into conjunctival sac without scratching. By using the locator, the operator can accurately design how much conjunctiva tissue should be excised. Since excessive or insufficient conjunctiva excision could possibly be avoided, this procedure is superior to currently used crescent-shaped conjunctiva resection as evidenced by an array of clinical evaluations in this report. OSDI is widely accepted and used as a method for the study concerned with ocular surface disease. Scores of OSDI is lower in locator-assisted conjunctiva excision than that in crescent-shaped resection. This might be attributable to the improvement in relatively accurate loose conjunctiva excision as shown by evaluations of remnant conjunctiva fold and wound healing in this study. As for the insignificant differences in evaluations of the height of tear meniscus, BUT, and TCT between the two surgical procedures, it may lie in the similar resolving of mechanical problems caused by the interposed conjunctiva fold between the globe and the lower eyelid. Among the advantages of locator-assisted conjunctiva excision, its fewer complications may encourage a most liberal use. However, this procedure is limited by its inevitable suturing of conjunctiva cut which may carry risks of suture-related disadvantages and complications such as postoperative discomfort, abscesses, granuloma formation, and 8 giant papillary conjunctivitis. In this regard, suture-related complications could be reduced by amniotic membrane transplantation after conjunctiva is approximated by suture.11 Also, fibrin glue may offer a novel way of repairing conjunctival defects and has been shown to avoid suture-related complications, decrease surgical time, and decrease ocular inflammation and discomfort postoperatively. 12,13The use of fibrin glue has been proven to be rather safe, but the potential for side effects cannot be ruled out given that many of the constituents are derived from human blood plasma. 14 Both these two approaches may achieve a good therapeutic result for CCh when used as adjunctive methods for conjuntiva excision to better reconstruct the conjunctival surface. Further studies are warranted to investigate if the locator-assisted conjunctiva excision would be more effective in treating CCh under the help of amniotic membrane transplantation or fibrin glue. In conclusion, quantitative locator can be used as an effective, safe, and less time-consuming instrument to facilitate conjunctival excision for symptomatic CCh treatment. 9 Right Eye Left Eye Figure 1. A schematic diagram illustrating the design of the locator. It consists of a circle at the centre with a diameter in 12 mm and two arcs 5 mm posterior from the limbus. A slit between the two arcs was made as an access of loose conjunctiva to the surface of the locator (arrows). Five holes with a diameter in 1 mm at the 2, 4, 6, 8, 10-o’clock positions of the outer arc are made for the micro-forceps to pull out the conjunctiva beneath the inner face of the locator after it is placed on the eyeball. Figure 2. The locator made of β-hydroxyethyl methacrylate / HEMA Figure 3. The locator is placed on eyeball and the loose conjunctiva is pulled out from the little holes located at the edge of the outer arc and from the slit between the two arcs. 10 Figure 4. A 76-year-old male patient with CCh. A) before surgery; B) 8 weeks after locator-assisted conjunctiva excision. REFERENCES 1. Mimura T, Yamagami S, Usui T, et al. Changes of conjunctivochalasis with age in a hospital-based study. Am J Ophthalmol. 2009; 147:171-177. 2. Li QS, Zhang XR , Zou HM, et al. Epidemiologic study of conjunctivochalasis in populations equal or over 60 years old in Caoyangxincun community of Shanghai, China. Chin J Ophthalmol. 2009; 45:793-798. (Chinese) 3. Meller D, Tseng SCG. Conjunctivochalasis: literature review and possible pathophysiology. Surv Ophthalmol. 1998;43:225–232. 4. Liu D. Conjunctivochalasis: a cause of tearing and its management. Ophthal Plast Reconstr Surg 1986; 2:25–28. 5. Hughes WL. Conjunctivochalasis. Am J Ophthalmol. 1942; 25: 48–51. 6. Yamamoto M, Hirano N, Haruta Y,et al. Bulbar conjunctival laxness and idiopathic subconjunctival hemorrhage. Atarashii Ganka.1994;11:1103–1106. 7. Ozcura F,Aydin S,Helvaci MR.Ocular surface disease index for the diagnosis of dry eye syndrome. Ocul Immunol Inflamm.2007;15:389-393. 8. Zhang X, Li Q, Xu Y. Observation of long-term effect of conjunctivochalasis surgery. Chinese Journal of Ocular Trauma & Occupational Eye Disease. 2004; 26: 683-685.(Chinese) 9. Jordan DR, Pelletier CR. Conjunctivochalasis. Can J Ophthalmol. 1996;31:192–3. 10. Serrano F, Mora LM. Conjunctivochalasis: a surgical technique. Ophthal Surg 1989;20:883–884. 11. Meller D, Maskin SL, Pires RT, et al. Amniotic membrane transplantation for symptomatic conjunctivochalasis refractory to medical treatments. Cornea 2000;19:796–803. 12. Uy HS, Reyes JM, Flores JD, et al. Comparison of fibrin glue and sutures for attaching conjunctival autografts after pterygium excision. Ophthalmology. 2005;112:667–671. 13. Koranyi G, Seregard S, Kopp ED. Cut and paste: a no suture, small incision approach to pterygium surgery. Br J Ophthalmol. 2004;88:911–914. 14. Brodbaker E, Bahar I, Slomovic AR. Novel use of fibrin glue in the treatment of conjunctivochalasis. Cornea 2008;27:950–952. 11